

Abstract
The increasing popularity and success of hip arthroscopy has led to the development of related techniques for treating hip pathologies external to the joint proper. These minimally invasive endoscopic procedures serve in a diagnostic role to complement clinical evaluations and offer a therapeutic alternative to traditional open techniques. The indications for extra-articular hip endoscopy continue to expand. Recent literature describes applications for treating greater trochanteric pain syndrome, internal snapping hip, deep gluteal syndrome, and subspine impingement and for diagnosing and treating extra-articular sources of hip pain in patients who have undergone hip arthroplasty.
Keywords: Hip arthroscopy, Hip endoscopy, Greater trochanteric pain syndrome, Snapping hip, Deep gluteal syndrome, Subspine impingement, Postarthroplasty arthroscopy
Introduction
Intra-articular hip arthroscopy has increased in both popularity and success. Due to arthroscopic advancements, there has been a logical progression to treating extra-articular hip pathology with similar techniques. Inherent in these procedures is the advantage that surgery can be performed in a less invasive fashion. The origins of hip arthroscopy trace back to 1931 [1], and it came into clinical practice in the1980s [2, 3], with extra-articular hip endoscopic procedures being reported since the late 1990s [4]. With hip endoscopy still in its infancy, understanding the evidence supporting these novel techniques and their indications for use is of critical importance. The indications for treating extra-articular hip pathologies continue to expand and are summarized in Table 1. These indications are discussed in further detail, individually, in this review.
Table 1.
Indications for extra-articular hip endoscopy
| Diagnosis | Included Pathologies |
|---|---|
| Greater trochanteric pain syndrome | Greater trochanter bursitis |
| Gluteus medius tear | |
| Gluteus minimus tear | |
| External snapping hip | |
| Internal snapping hip | Internal snapping hip |
| Deep gluteal pain syndrome | Sciatic nerve entrapment |
| Piriformis syndrome | |
| Anterior inferior iliac spine/subspine impingement | Anterior inferior iliac spine/subspine impingement |
| Post-hip arthroplasty pain | Unknown (diagnostic endoscopy) |
| Iliopsoas impingement |
Relevant anatomy/surgical technique
The hip can be divided into four zones or compartments: the central (intra-articular), peripheral, peritrochanteric (lateral or third compartment), and subgluteal space. The central compartment includes the articular surfaces of the acetabulum and femoral head, the ligamentum teres, and the endoarticular labrum. The peripheral compartment includes the nonarticulating aspect of the femoral head, the iliopsoas tendon, the outer labral rim, the femoral neck, and the joint capsule. The peritrochanteric compartment consists of the greater trochanter and its bursa, the iliotibial band, and the gluteus medius and minimus tendons. The deep subgluteal space contains the short external rotator muscles, the piriformis, and the sciatic nerve [3, 5–7].
The operative setup for hip endoscopy is similar to that for hip arthroscopy with respect to patient positioning and instrumentation. The procedure can be performed in the supine or lateral position, as previously described by Byrd [8] and Glick et al. [2], respectively. Extra-articular hip endoscopy frequently follows arthroscopic evaluation and treatment of any central or peripheral hip pathology. After completion of the intra-articular components of the procedure, traction on the lower extremity should be released and the perineal post removed to reduce trauma on the adjacent soft tissue and neurovascular structures. Removal of the post also facilitates a more thorough dynamic examination when treating pathologies such as cam lesions and musculotendinous and nerve kinematics. Various portals have been described for use in diagnosis and treatment of extra-articular hip pathology, which vary depending on surgeon preference and the pathology being treated; we describe these within each pathology-specific section below and acknowledge that there are multiple ways to perform these procedures successfully. Recently published literature has been dedicated to outlining in great detail relevant surgical anatomy [5, 6]. We strongly recommend studying these publications, as well as the pathology-specific references cited.
Greater trochanteric pain syndrome
Greater trochanteric bursitis
Greater trochanteric pain syndrome (GTPS) is a broad diagnostic category that groups together many pathologies lateral to the hip joint, including greater trochanteric bursitis (GTB), gluteus medius and minimus tears, and external snapping hip. The gluteus medius inserts into the superoposterior and lateral facets of the greater trochanter; the subgluteus medius bursa lies over the lateral facet. The gluteus minimus tendon attaches to the anterior facet of the greater trochanter, with the subgluteus minimus bursa sitting deep to the tendon about the anterior facet and anterior hip capsule. The trochanteric bursa, the largest bursa, sits deep to the fibers of the gluteus maximus and tensor fascia lata (TFL) as they form the iliotibial band (ITB) while covering the posterior facet, the distal-lateral medius tendon at the lateral facet, and the proximal vastus lateralis insertion [9–12]. True GTB is inflammation of one of the bursae about the greater trochanter, most commonly those associated with the gluteus medius and minimus tendons, ITB, or TFL, resulting in lateral hip pain [13–15]. This inflammation is thought to be the result of preexisting gait abnormalities such as with spinal pathology, gynecoid pelvis, or tight TFL or gluteal musculature with repetitive activity [13, 15–18].
Patients complain of lateral hip pain exacerbated by direct pressure, prolonged standing or upright activity, and resisted abduction [13, 15, 17, 18]. Diagnosis of GTB is confounded by the general nature of the symptoms, which may be attributed to alternative intra- or extra-articular pathologies of the hip joint. Furthermore, GTB is commonly associated with the spectrum of GTPS diagnoses, clouding the true etiology of the patient’s symptoms and delaying the physician’s ability to treat them appropriately [13–15, 17, 18].
Greater trochanteric bursitis is a clinical diagnosis of exclusion. Evaluation includes plain radiographs for assessment of alternative pathology. Intrabursal calcifications may be noted but are nonspecific [13, 15–17]. Dynamic ultrasound and computed tomography (CT) have been found useful as additional modalities in excluding other causes of lateral hip pain but do not regularly make the diagnosis of GTB [19–21]. Magnetic resonance imaging (MRI) is currently considered the gold standard imaging test for diagnosing GTB [13, 15, 16, 19].
First-line treatment for GTB is nonoperative. Rest, avoidance of the inciting activity, weight loss, oral antiinflammatory medications, and physical therapy are recommended [9, 13, 14]. In the setting of persistent pain despite noninvasive treatments, a local injection of corticosteroid and local anesthetics may be indicated for both diagnosis and treatment [9]. Failure of nonoperative treatment has led to the development of surgical approaches for treatment of GTB. Originally described as open procedures, the preferred method is now endoscopic.
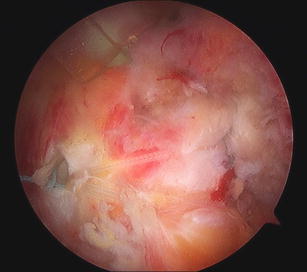
Endoscopic treatment of GTB has been described by a number of authors. The most commonly cited method is endoscopic bursectomy [6, 22–24]. In the practice of the senior author (M.J.S.), the supine position is preferred for treatment of disease processes in the peritrochanteric space. A standard anterolatral (AL) portal is created initially. If there is no concern for intra-articular pathology, the portal may be moved slightly more superior to allow for better visualization of the insertion of the gluteus medius and minimus tendons. We prefer to slide the initial trochar under the ITB, although an outside-in technique of creating a cross type incision in the ITB has also been described. Once we have established our AL portal, a 70° scope is used to visualize the peritrochanteric space, which is often found to be occupied by copious amounts of thickened bursa (Fig. 1). We then create a distal AL (DAL) portal in line with the initial AL portal to be used as a working portal. The lateral decubitus position is preferred by some authors, with entry into the lateral compartment using an anterior portal and a distal posterior portal to allow for visualization and adequate access to the peritrochanteric space. Bursectomy is performed to allow for improved visualization, followed by inspection of the ITB and gluteal insertions [6, 22, 23]. A thorough bursectomy is complete when it extends to the insertion of the gluteus maximus and when the gluteus medius and minimus insertions are clearly visualized. This step is accomplished with a motorized shaver and a radiofrequency device to maintain hemostasis. Release of the posterior third of the ITB has been shown to be beneficial in cases where direct wear on the greater trochanter is seen or in patients with known recalcitrant external snapping hip symptoms [23]. Baker et al., in a prospective study of 25 patients who underwent arthroscopic bursectomy and were assessed at a mean follow-up of 26 months, showed significant improvement in Visual Analog Score (VAS; 7.2–3.1), Harris Hip Scores (HHS; 51–77), and short-form 36 scores from the preoperative status scores [22]. Variations on the endoscopic bursectomy have been described, including an ITB release either preceding [23] or subsequent to the bursectomy [25], with favorable results. Similarly, successful treatment of GTB secondary to gluteus medius and minimus calcific tendonitis has been described by Kandemir et al. [26].
Fig. 1.

Initial view of an inflammatory and thickened trochanteric bursa as initially visualized from the anterolateral portal with a 70° arthroscope
Gluteus medius and minimus tears
As was described in the previous section, the gluteus medius inserts into the superoposterior and lateral facets of the greater trochanter, and the gluteus minimus inserts into the anterior facet of the greater trochanter [9–12]. Functioning much like a rotator cuff of the hip, the gluteus medius and minimus muscles act to stabilize the hip joint and initiate abduction [11, 27]. Tears of these tendons, much like those in the shoulder, occur most commonly at the footprint on the greater trochanter. They may be intrasubstance, partial, or complete [11, 27, 28]. Clinically, they may be difficult to diagnose, even with direct endoscopic visualization due to the articular-sided nature of the tear, which may be obscured by unaffected bursal-sided tendon substance [11, 20, 29]. Patients with gluteal tendon pathology present with symptoms similar to those of GTB: lateral hip pain and pain worsened by direct pressure, weight bearing, and resisted abduction [13, 16–18, 27, 28]. The evaluation of patients with gluteal tendinopathy is very similar to that of GTB, with the history and physical often yielding generalized findings. Clinical evaluation is important to rule out spinal, hip joint, and other extra-articular pathologies.
Plain radiographs are generally of low yield but are necessary for excluding other sources of pain. They can be helpful in defining osteophytes off the greater trochanter over which the gluteus tendon may be draped, leading to a painful lateral hip condition. MRI is a commonly used evaluation of gluteus medius and minimus tears with high sensitivity and positive predictive value [19, 21]. It must be noted, however, that there is a high rate of false positive findings, up to 88 % in one series, making the clinician’s clinical evaluation of great importance in the overall diagnosis [20]. Ultrasound has been shown to have a sensitivity of 79 % and a positive predictive value of 100 %, rivaling that of MRI, and may be a reliable alternative to MRI [21].
Initial treatment of gluteal tendinopathy is identical to that of GTB: rest, avoidance of inciting activities, oral antiinflammatories, and physical therapy. A precise diagnosis of gluteal tendonopathy may be overlooked, with the patient’s findings being categorized under the broader diagnosis of GTPS [16–18]. Injection of corticosteroid may offer some relief if placed within the gluteus medius or minimus bursae; however, failure of injection often leads to further imaging and to realizing the true etiology of the symptoms [9].
Endoscopic debridement and repair of gluteus medius and minimus tendinopathy has been described by a number of authors, with the setup and approach identical to that performed for treating GTB for entry into the peritrochanteric compartment of the hip [6, 11, 29]. The construct preferred by the senior author is one of a transosseous equivalent double row repair technique, which has been shown to offer a biomechanically superior construct (Figs. 2 and 3) [30]. A prospective study by Voos et al. of 10 patients showed 100 % resolution of pain and return of full strength in the hip abductors at an average follow-up of 25 months. HHS at 1 year follow-up averaged 94, and Hip Outcomes Scores averaged 93. There were no adverse outcomes; 7/10 reported that their hip was normal, and 3/10 said that they were nearly normal [29].
Fig. 2.

Gluteus medius tear viewed arthroscopically with foot print prepared and tendon prepared for repair
Fig. 3.
Gluteus medius tendon repair performed with a double row transosseous equivalent repair construct
External snapping hip
External coxa saltans or external snapping hip can occur as a result of a thickening of the posterior ITB, the TFL, or the gluteus maximus as they slide over the greater trochanter during hip flexion [31–34]. This frictional irritation may also lead to GTB [31]. As with internal snapping hip, patients will describe a snapping sensation that occurs with exercise or routine activities; they will be able to localize their pain and recreate the snap. The Ober test may be positive with tightness of the ITB. Applying pressure over the greater trochanter as the patient flexes at the hip may prevent the snap [31, 35].
Imaging consists of x-rays of the pelvis to exclude other pathologies causing hip pain [32, 33, 35]. Ultrasound and MRI may complement the history and physical exam but are probably unnecessary, except for cases in which there is concern for additional pathologies [35].
Nonoperative treatment is the first step for patients with symptomatic external coxa saltans. Rest, avoiding activities that lead to pain, oral antiinflammatory medications, and physical therapy are important. Physical therapy and steroid injections into the bursa may be tried if pain persists with routine daily activities [31, 32, 35]. In patients with recalcitrant symptoms, open surgical release of the ITB can be accomplished by resection [36, 37], step-cuts [38], or Z-plasty [39, 40].
Endoscopic approaches have also been effective for treating external snapping hip. Ilizaliturri et al. [32] placed the patient in the lateral position and used superior and inferior trochanteric portals. Working from the outside surface of the ITB, they resected subcutaneous fat in order to expose the ITB. Once visualized, they created a diamond-shaped resection and release, after which, the trochanteric bursa was debrided [32]. Ten of 11 hips (10 patients) were relieved of their snapping, and all were relieved of pain at a minimum of 1-year follow-up. No patient required revision surgery, and all patients returned to preoperative levels of activity [32]. In order to preserve the shape of the lateral thigh and the biomechanics of the ITB, Polesello et al. [33] performed a gluteus maximus tenotomy to decrease tension on the iliotibial band. They placed the patient in the supine position and used superior and inferior trochanteric portals. After placing their cannula through the ITB, an inside-out technique was performed to expose and transect the gluteus maximus tendon close to the linea aspera. Seven of 9 hips (8 patients) were relieved of pain and snapping postoperatively, with 1 patient requiring a revision operation. All patients returned to their preoperative level of activity, and no patients complained of weakness at a minimum follow-up of 22 months [33].
Internal snapping hip
Internal coxa saltans or snapping hip occurs when the iliopsoas slides over the iliopectineal ridge [31, 35, 41] or the anterior capsulolabral complex and femoral head [31, 35, 42]. It can be asymptomatic but may result in an audible and painful snap [31, 35, 43]. It occurs when the hip is extended from a flexed, abducted, and externally rotated position or is internally rotated and adducted from an externally rotated and abducted position [31, 35, 43, 44, 45•]. Patients with internal snapping hip often complain of a painful snapping sensation that occurs with exercise and may be reproducible in the office by the patient or on physical exam. Applying pressure to the iliopsoas tendon may prevent the snap [31]. Diagnosis may be obscured because mechanical intra-articular pathology can cause similar symptoms [35].
Radiographs are not necessary to make the diagnosis of internal snapping hip, and there is nothing pathognomonic that will be identified on plain films. They are nonetheless an essential part of the workup to identify anatomic abnormalities, but they should not be used in isolation [42, 45•, 46]. Iliopsoas bursography [47], dynamic ultrasound [48], CT, and MRI can all be used to assist in the diagnosis [46].
Initial treatment for internal snapping hip is nonoperative. It is recommended that the patient rest, use oral antiinflammatory medications, avoid activities that reproduce the snapping, and participate in physical therapy [31]. If the pain becomes more persistent and occurs with routine activities, physical therapy and steroid injections are indicated [31, 49]. For patients who do not respond to nonoperative treatment, surgical intervention is appropriate. Traditionally, this was done with an open approach [31], but more recently, endoscopy has been popularized.
Two techniques of hip endoscopy have been described for treating internal snapping hip [35, 50]. The iliopsoas tendon can be released either at its insertion into the lesser trochanter or via a transcapsular technique at the level of the hip joint [35, 49, 50]. These procedures can be successfully done either from the lateral decubitus position [42, 49] or from the supine position [35, 44, 51–53]. Iliopsoas release is preceded by diagnostic hip arthroscopy and treatment of concurrent femoroacetabular impingement (FAI) lesions, chondral damage, and labral tears if indicated [35, 42, 49–53]. By releasing at the lesser trochanter, a number of authors have reported completely relieving snapping in patients and that, after initial hip flexion weakness, strength is ultimately restored and patients return to their preoperative level of activity and work [42, 52], including competitive athletics [51]. Results have also been promising with the transcapsular approach [49, 53], which is the senior author’s preferred approach when this is to be performed, although currently, in our practice, the indications for psoas release are extremely limited. In a prospective randomized study of 19 patients comparing the two techniques, Ilizaliturri et al. found that at an average follow-up of 20 months, all patients treated by either technique were relieved of their snapping without complications, and there were no differences in their Western Ontario and McMaster Universities osteoarthritis scores [49]. Recently, Fabricant et al. investigated the effect of femoral anteversion on clinical outcomes after arthroscopic iliopsoas tendon lengthening and found excessive anteversion to be correlated with poorer clinical scores pre- and postoperatively [44].
Sciatic nerve entrapment and deep gluteal syndrome
The sciatic nerve exits the pelvis through the sciatic notch, usually inferior to the piriformis muscle, although variations are common [54, 55]. Within the deep gluteal region, it is covered by the gluteus maximus and passes between the ischial tuberosity and the greater trochanter [56, 57]. Entrapment of the nerve may occur as a consequence of a number of anatomic features within the deep gluteal space and, as such, may be broadly termed deep gluteal syndrome (DGS) [58]. Patients with sciatic nerve entrapment due to compression in the deep gluteal region are commonly unable to sit for more than 30 min and may have paresthesias and radicular pain in the affected limb [59]. Patients may have posterior hip tenderness and pain with active and passive piriformis stretch testing [56, 60•].
Evaluation of patients with suspected sciatic nerve impingement starts with the history and a physical. Lumbar spine, sacroiliac joint, and femoroacetabular pathology must be excluded as the source of pain, as well as lumbar spine radiculopathy [55, 56, 60•]. Imaging focuses on the lumbosacral spine, pelvis, and hips and includes plain radiographs, CT, MRI, and magnetic resonance arthrography to demonstrate aberrant anatomy and pathology [55, 56, 60•, 61]. Electrodiagnostic studies may also be useful [55, 58, 61].
Initial treatment for DGS is nonoperative. Noninvasive means of correcting abnormal biomechanics, such as with orthotics and physical therapy, are first line, along with oral antiinflammatory medications. Steroid or anesthetic injections are considered in unresponsive cases [58, 61, 62]. Surgical sciatic nerve decompression is a last resort. This procedure can be accomplished via an open approach to the hip [55] or with a focused endoscopic technique. Dezawa et al. [63] first described a dry arthroscopic technique for piriformis release under local anesthetic in eight limbs, and Hwang et al. endoscopically decompressed a perineural cyst and released the piriformis in 1 patient [64].
The endoscopic treatment of DGS was well described by Martin et al., as are clinical outcomes from their series of 35 patients [56, 60•]. They described using the supine position with nerve conduction and electromyographic monitoring to evaluate for nerve changes after release [60•]. The AL and posterolateral (PL) portals can be used to evaluate the peritrochanteric space; an auxillary PL portal 3 cm posterior and 3 cm superior to the greater trochanter enables the surgeon to view the nerve up to the sciatic notch. Decompression starts distal to the quadratus femoris and then proceeds proximally, releasing any fibrovascular bands around the sciatic nerve up to the sciatic notch. Evaluation of possible impinging anatomy includes fibers of the hamstrings, gemelli-obturator internus complex, quadratus femoris, and the piriformis tendon [56, 60•]. At an average of 1-year follow-up, 83 % of patients reported no sciatic nerve sitting pain (inability to sit for >30 min), the modified Harris Hip Scores (MHHS) increased from 54 to 78, and VAS decreased from 6.9 ± 2.0 to 2.4 ± 2.6. Five of 35 patients were considered to have low improvement as determined by their MHHS and amount of pain relief, which may be related to previous abdominal surgery, trauma, or decreased femoral version [56].
Anterior inferior iliac spine/subspine impingement
An emerging literature is shedding light on extra-articular hip impingement, caused when the anterior aspect of the femoral head and neck impacts the anterior inferior iliac spine (AIIS) as a result of AIIS hypertrophy, prior avulsion injuries, or pelvic osteotomies. Diagnosis of AIIS impingement may be increasing in incidence [65, 66]. Patients with AIIS or subspine impingement describe hip pain that occurs with hip flexion and internal rotation, tenderness over the AIIS, and only partial pain relief after intra-articular anesthetic injections [65, 66].
Pelvic x-rays and CT scans are important in diagnosis and preoperative planning [65, 66]; three-dimensional CT reconstructions are also valuable [65, 67•]. These may show a hypertrophic AIIS that extends inferiorly to or below the level of the anterior superior acetabular rim [65, 66, 67•]. There may also be decreased femoral head–neck offset [65, 66, 67•], a retroverted acetabulum, impingement cysts in the femoral neck more distal than might be expected with acetabular impingement [65, 67•], normal center–edge angles, and increased alpha angles [67•].
Symptomatic avulsion fractures of the AIIS have previously been treated with open reduction internal fixation and debridement of excessive callus [68]. Pan et al. reported the first case of AIIS impingement [66], using a Smith–Peterson approach. They observed that when the hip was flexed to approximately 90°, the anterior aspect of the femoral head and neck impinged on the AIIS. The AIIS was resected down to normal size, and the patient was able to flex to 120° and had normal internal rotation without pain [66].
In 2011, Larson et al. published the first case series of 3 patients with AIIS impingement that they successfully treated endoscopically [65]. Matsuda et al. treated a 13-year-old male with AIIS apophyseal avulsion injury leading to FAI that was treated with arthroscopic labral repair, femoroplasty, acetabuloplasty, and spinoplasty. The patient developed heterotopic ossification in spite of antiinflammatory prophylaxis but returned asymptomatically to sport [69]. Hetsroni et al. reported on their series of 10 patients with AIIS impingement treated endoscopically. When indicated, intra-articular pathology was treated first, with the endoscopic portion following. The authors used the AL and mid-anterior portals to dissect to the AIIS and burr down the prominence [67•]. There were no reported complications, and average hip flexion increased almost 20°. MHHS scores increased 34 points, and all competitive athletes in the study were able to return to training and competition at 6 months postoperatively [67•].
Iliopsoas tendonopathy after hip arthroplasty
In spite of the success of hip arthroplasty procedures, pain accompanies some patients postoperatively. It can occur after resurfacing or replacement procedures, and there are many different presentations of hip pain in these patients. Hip or groin pain can result from a host of causes, including, but not limited to, infection, aseptic loosening, synovitis, periprosthetic fracture, osteolysis, nerve injury, iliopsoas tendonopathy, or complex regional pain syndrome [70]. Iliopsoas impingement was found to affect 4.3 % of patients with pain after total hip arthroplasty (THA) [71]. There are a number of reasons why it can occur [70, 72, 73], but ultimately the tendon becomes inflamed and painful.
Patients with iliopsoas impingement and tendonitis present, after an asymptomatic period following hip arthroplasty, with groin pain worsened by hip extension. Anterior groin palpation can reproduce the pain, hip extension is painful, and patients have difficulty with straight leg raises (SLR) [70, 72, 74]. After the history and physical exam, plain radiographs should be obtained to evaluate for loosening, fracture, wear, or malpositioned implants. Infection should be ruled out with c-reactive protein, erythrocyte sedimentation rates, and possibly joint aspirations and cultures. Metal hypersensitivities must also be considered in the differential. Ultrasound, CT, and MRI assist with the diagnosis [70, 72, 74]. NSAIDs and therapy are first-line treatment modalities, followed by steroid injections for therapeutic and diagnostic roles. Surgical intervention can be performed to correct the causal factor, such as a malpositioning of the acetabular component and release of the inflamed psoas tendon [72, 74].
Recent studies have shown that hip endoscopy can be used to treat iliopsoas pathology after hip arthroplasty. Van Riet et al. describe a transcapsular approach for successful iliopsoas release after hip resurfacing, THA, and revision THA. The authors describe positioning the patient supine and using the AL working portal and DAL viewing portal. The joint is distended, but depending on the prior procedure and implant used, neocapsular scarring may be an obstacle. Cultures were obtained, and the authors recommend obtaining synovial biopsies. After evaluation of the prosthesis, an anterior capsulotomy is made to access the iliopsoas tendon and perform the release. Hip Osteoarthritis Outcome Scores were not significantly different pre- and postoperatively, but all patients demonstrated full flexion strength 1 month after surgery, and 6 of 9 patients had complete relief of pain with SLR [74].
When the etiology of groin pain is unclear after appropriate examination, imaging, and laboratory studies, endoscopy has proven useful. Arthroscopic and endoscopic evaluation can be used for diagnostic purposes to obtain a definitive diagnosis or to confirm or modify a provisional diagnosis, providing visualization of the joint and surrounding tissues, as well as access for biopsies to investigate infectious and metal ion disease. It also provides for a simple transition into therapeutic procedures for debriding postoperative adhesions, synovitis, and bursitis and for performing tendon releases if indicated [75, 76].
Conclusions
Extra-articular hip endoscopic techniques are being used to treat an increasingly large breadth of hip pathologies. Much of the current literature consists of case reports and small case series, but with promising results. As these techniques become more widespread and follow-up periods expand, the indications for hip endoscopy and the role that these minimally invasive procedures have in treating pathologies traditionally addressed with open techniques will become clearer.
Compliance with ethics guidelines
Conflict of interest
Michael S. Reich, Claire Shannon, Eugene Tsai, and Michael J. Salata declare that they have no conflict of interest.
Human and animal rights and informed consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Contributor Information
Michael S. Reich, Phone: +1-216-8443233, FAX: +1-216-8448181, Email: Michael.Reich@uhhospitals.org
Claire Shannon, Phone: +1-216-8443233, FAX: +1-216-8448181, Email: Claire.Shannon@uhhospitals.org.
Eugene Tsai, Phone: +1-216-8443233, FAX: +1-216-8448181, Email: Eugene.Tsai@uhhospitals.org.
Michael J. Salata, Phone: +1-216-8446097, FAX: +1-216-8445970, Email: Michael.Salata@uhhospitals.org
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
- 1.Burman MS. Arthrosocpy or the direct visualization of joints: an experimental cadaver study. J Bone Joint Surg Am. 1931;13(4):669–95. doi: 10.1097/00003086-200109000-00003. [DOI] [PubMed] [Google Scholar]
- 2.Glick JM, Sampson TG, Gordon RB, et al. Hip arthroscopy by the lateral approach. Arthroscopy. 1987;3(1):4–12. doi: 10.1016/S0749-8063(87)80003-8. [DOI] [PubMed] [Google Scholar]
- 3.Dorfmann H, Boyer T. Hip arthroscopy utilizing the supine position. Arthroscopy. 1996;12(2):264–7. doi: 10.1016/S0749-8063(96)90028-6. [DOI] [PubMed] [Google Scholar]
- 4.Bradley DM, Dillingham MF. Bursoscopy of the trochanteric bursa. Arthroscopy. 1998;14(8):884–7. doi: 10.1016/S0749-8063(98)70027-1. [DOI] [PubMed] [Google Scholar]
- 5.Byrd JWT. Routine arthroscopy and access: central and peripheral compartments, iliopsoas bursa, peritrochanteric, and subgluteal spaces. In: Byrd JWT, editor. Operative hip arthroscopy. New York: Springer; 2013. pp. 131–60. [Google Scholar]
- 6.Voos JE, Rudzki JR, Shindle MK, et al. Arthroscopic anatomy and surgical techniques for peritrochanteric space disorders in the hip. Arthroscopy. 2007;23(11):1246.e1241–e1245. [DOI] [PubMed]
- 7.Dorfmann H, Boyer T. Arthroscopy of the hip: 12 years of experience. Arthroscopy. 1999;15(1):67–72. doi: 10.1053/ar.1999.v15.015006. [DOI] [PubMed] [Google Scholar]
- 8.Byrd JW. Hip arthroscopy utilizing the supine position. Arthroscopy. 1994;10(3):275–80. doi: 10.1016/S0749-8063(05)80111-2. [DOI] [PubMed] [Google Scholar]
- 9.Shbeeb MI, O'Duffy JD, Michet CJ, Jr, et al. Evaluation of glucocorticosteroid injection for the treatment of trochanteric bursitis. J Rheumatol. 1996;23(12):2104–6. [PubMed] [Google Scholar]
- 10.Dwek J, Pfirrmann C, Stanley A, et al. MR imaging of the hip abductors: normal anatomy and commonly encountered pathology at the greater trochanter. Magn Reson Imaging Clin N Am. 2005;13(4):691–704. doi: 10.1016/j.mric.2005.08.004. [DOI] [PubMed] [Google Scholar]
- 11.Domb BG, Nasser RM, Botser IB. Partial-thickness tears of the gluteus medius: rationale and technique for trans-tendinous endoscopic repair. Arthroscopy. 2010;26(12):1697–705. doi: 10.1016/j.arthro.2010.06.002. [DOI] [PubMed] [Google Scholar]
- 12.Pfirrmann CW, Chung CB, Theumann NH, et al. Greater trochanter of the hip: attachment of the abductor mechanism and a complex of three bursae–MR imaging and MR bursography in cadavers and MR imaging in asymptomatic volunteers. Radiology. 2001;221(2):469–77. doi: 10.1148/radiol.2211001634. [DOI] [PubMed] [Google Scholar]
- 13.Williams BS, Cohen SP. Greater trochanteric pain syndrome: a review of anatomy, diagnosis and treatment. Anesth Analg. 2009;108(5):1662–70. doi: 10.1213/ane.0b013e31819d6562. [DOI] [PubMed] [Google Scholar]
- 14.Lustenberger DP, Ng VY, Best TM, Ellis TJ. Efficacy of treatment of trochanteric bursitis: a systematic review. Clin J Sport Med. 2011;21(5):447–53. doi: 10.1097/JSM.0b013e318221299c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tibor LM, Sekiya JK. Differential diagnosis of pain around the hip joint. Arthroscopy. 2008;24(12):1407–21. doi: 10.1016/j.arthro.2008.06.019. [DOI] [PubMed] [Google Scholar]
- 16.Del Buono A, Papalia R, Khanduja V, et al. Management of the greater trochanteric pain syndrome: a systematic review. Br Med Bull. 2012;102:115–31. doi: 10.1093/bmb/ldr038. [DOI] [PubMed] [Google Scholar]
- 17.Fearon AM, Scarvell JM, Neeman T, et al. Greater trochanteric pain syndrome: defining the clinical syndrome. Br J Sports Med. 2013;47:649–53. [DOI] [PubMed]
- 18.Segal NA, Felson DT, Torner JC, et al. Greater trochanteric pain syndrome: epidemiology and associated factors. Arch Phys Med Rehabil. 2007;88(8):988–92. doi: 10.1016/j.apmr.2007.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Blankenbaker DG, Ullrick SR, Davis KW, et al. Correlation of MRI findings with clinical findings of trochanteric pain syndrome. Skeletal Radiol. 2008;37(10):903–9. doi: 10.1007/s00256-008-0514-8. [DOI] [PubMed] [Google Scholar]
- 20.Kong A, Van der Vliet A, Zadow S. MRI and US of gluteal tendinopathy in greater trochanteric pain syndrome. Eur Radiol. 2007;17(7):1772–83. doi: 10.1007/s00330-006-0485-x. [DOI] [PubMed] [Google Scholar]
- 21.Westacott DJ, Minns JI, Foguet P. The diagnostic accuracy of magnetic resonance imaging and ultrasonography in gluteal tendon tears–a systematic review. Hip Int. 2011;21(6):637–45. doi: 10.5301/HIP.2011.8759. [DOI] [PubMed] [Google Scholar]
- 22.Baker CL, Jr, Massie RV, Hurt WG, Savory CG. Arthroscopic bursectomy for recalcitrant trochanteric bursitis. Arthroscopy. 2007;23(8):827–32. doi: 10.1016/j.arthro.2007.02.015. [DOI] [PubMed] [Google Scholar]
- 23.Farr D, Selesnick H, Janecki C, Cordas D. Arthroscopic bursectomy with concomitant iliotibial band release for the treatment of recalcitrant trochanteric bursitis. Arthroscopy. 2007;23(8):905.e1–e5. [DOI] [PubMed]
- 24.Fox JL. The role of arthroscopic bursectomy in the treatment of trochanteric bursitis. Arthroscopy. 2002;18(7):E34. doi: 10.1053/jars.2002.35143. [DOI] [PubMed] [Google Scholar]
- 25.Govaert LHM, van Dijk CN, Zeegers AVCM, Albers GHR. Endoscopic bursectomy and iliotibial tract release as a treatment for refractory greater trochanteric pain syndrome: a new endoscopic approach with early results. Arthrosc Tech. 2012;1(2):e161–4. doi: 10.1016/j.eats.2012.06.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kandemir U, Bharam S, Philippon MJ, Fu FH. Endoscopic treatment of calcific tendinitis of gluteus medius and minimus. Arthroscopy. 2003;19(1):E4. doi: 10.1053/jars.2003.50021. [DOI] [PubMed] [Google Scholar]
- 27.Bunker TD, Esler CN, Leach WJ. Rotator-cuff tear of the hip. J Bone Joint Surg Br. 1997;79(4):618–20. doi: 10.1302/0301-620X.79B4.7033. [DOI] [PubMed] [Google Scholar]
- 28.Kagan A., 2nd Rotator cuff tears of the hip. Clin Orthop Relat Res. 1999;368:135–40. doi: 10.1097/00003086-199911000-00016. [DOI] [PubMed] [Google Scholar]
- 29.Voos JE, Shindle MK, Pruett A, et al. Endoscopic repair of gluteus medius tendon tears of the hip. Am J Sports Med. 2009;37(4):743–7. doi: 10.1177/0363546508328412. [DOI] [PubMed] [Google Scholar]
- 30.Dishkin-Paset JG, Salata MJ, Gross CE, et al. A biomechanical comparison of repair techniques for complete gluteus medius tears. Arthroscopy. 2012;28(10):1410–6. doi: 10.1016/j.arthro.2012.03.002. [DOI] [PubMed] [Google Scholar]
- 31.Allen WC, Cope R. Coxa saltans: the snapping hip revisited. J Am Acad Orthop Surg. 1995;3(5):303–8. doi: 10.5435/00124635-199509000-00006. [DOI] [PubMed] [Google Scholar]
- 32.Ilizaliturri VM, Jr, Martinez-Escalante FA, Chaidez PA, Camacho-Galindo J. Endoscopic iliotibial band release for external snapping hip syndrome. Arthroscopy. 2006;22(5):505–10. doi: 10.1016/j.arthro.2005.12.030. [DOI] [PubMed] [Google Scholar]
- 33.Polesello GC, Queiroz MC, Domb BG, et al. Surgical technique: endoscopic gluteus maximus tendon release for external snapping hip syndrome. Clin Orthop Relat Res. 2013;471:2471–6. [DOI] [PMC free article] [PubMed]
- 34.Brignall CG, Brown RM, Stainsby GD. Fibrosis of the gluteus maximus as a cause of snapping hip. A case report. J Bone Joint Surg Am. 1993;75(6):909–10. doi: 10.2106/00004623-199306000-00012. [DOI] [PubMed] [Google Scholar]
- 35.Byrd JWT. Snapping hip. Oper Techn Sport Med. 2005;13(1):46–54. doi: 10.1053/j.otsm.2004.09.003. [DOI] [Google Scholar]
- 36.Larsen E, Johansen J. Snapping hip. Acta Orthop Scand. 1986;57(2):168–70. doi: 10.3109/17453678609000894. [DOI] [PubMed] [Google Scholar]
- 37.Zoltan DJ, Clancy WG, Jr, Keene JS. A new operative approach to snapping hip and refractory trochanteric bursitis in athletes. Am J Sports Med. 1986;14(3):201–4. doi: 10.1177/036354658601400304. [DOI] [PubMed] [Google Scholar]
- 38.White RA, Hughes MS, Burd T, et al. A new operative approach in the correction of external coxa saltans: the snapping hip. Am J Sports Med. 2004;32(6):1504–8. doi: 10.1177/0363546503262189. [DOI] [PubMed] [Google Scholar]
- 39.Nam KW, Yoo JJ, Koo KH, et al. A modified Z-plasty technique for severe tightness of the gluteus maximus. Scand J Med Sci Sports. 2011;21(1):85–9. doi: 10.1111/j.1600-0838.2009.01011.x. [DOI] [PubMed] [Google Scholar]
- 40.Brignall CG, Stainsby GD. The snapping hip. Treatment by Z-plasty. J Bone Joint Surg Br. 1991;73(2):253–4. doi: 10.1302/0301-620X.73B2.2005149. [DOI] [PubMed] [Google Scholar]
- 41.Adler RS, Buly R, Ambrose R, Sculco T. Diagnostic and therapeutic use of sonography-guided iliopsoas peritendinous injections. AJR Am J Roentgenol. 2005;185(4):940–3. doi: 10.2214/AJR.04.1207. [DOI] [PubMed] [Google Scholar]
- 42.Ilizaliturri VM, Jr, Villalobos FE, Jr, Chaidez PA, et al. Internal snapping hip syndrome: treatment by endoscopic release of the iliopsoas tendon. Arthroscopy. 2005;21(11):1375–80. doi: 10.1016/j.arthro.2005.08.021. [DOI] [PubMed] [Google Scholar]
- 43.Schaberg JE, Harper MC, Allen WC. The snapping hip syndrome. Am J Sports Med. 1984;12(5):361–5. doi: 10.1177/036354658401200504. [DOI] [PubMed] [Google Scholar]
- 44.Fabricant PD, Bedi A, De La Torre K, Kelly BT. Clinical outcomes after arthroscopic psoas lengthening: the effect of femoral version. Arthroscopy. 2012;28(7):965–71. doi: 10.1016/j.arthro.2011.11.028. [DOI] [PubMed] [Google Scholar]
- 45.Ilizaliturri VM, Jr, Camacho-Galindo J. Endoscopic release of the iliopsoas tendon and iliotibial band. Oper Techn Sport Med. 2011;19:114–24. doi: 10.1053/j.otsm.2010.11.001. [DOI] [Google Scholar]
- 46.Wunderbaldinger P, Bremer C, Matuszewski L, et al. Efficient radiological assessment of the internal snapping hip syndrome. Eur Radiol. 2001;11(9):1743–7. doi: 10.1007/s003300100886. [DOI] [PubMed] [Google Scholar]
- 47.Harper MC, Schaberg JE, Allen WC. Primary iliopsoas bursography in the diagnosis of disorders of the hip. Clin Orthop Relat Res. 1987;221:238–41. [PubMed] [Google Scholar]
- 48.Cardinal E, Buckwalter KA, Capello WN, Duval N. US of the snapping iliopsoas tendon. Radiology. 1996;198(2):521–2. doi: 10.1148/radiology.198.2.8596860. [DOI] [PubMed] [Google Scholar]
- 49.Ilizaliturri VM, Jr, Chaidez C, Villegas P, et al. Prospective randomized study of 2 different techniques for endoscopic iliopsoas tendon release in the treatment of internal snapping hip syndrome. Arthroscopy. 2009;25(2):159–63. doi: 10.1016/j.arthro.2008.08.009. [DOI] [PubMed] [Google Scholar]
- 50.Wettstein M, Jung J, Dienst M. Arthroscopic psoas tenotomy. Arthroscopy. 2006;22(8):907.e1–e4. [DOI] [PubMed]
- 51.Anderson SA, Keene JS. Results of arthroscopic iliopsoas tendon release in competitive and recreational athletes. Am J Sports Med. 2008;36(12):2363–71. doi: 10.1177/0363546508322130. [DOI] [PubMed] [Google Scholar]
- 52.Flanum ME, Keene JS, Blankenbaker DG, Desmet AA. Arthroscopic treatment of the painful "internal" snapping hip: results of a new endoscopic technique and imaging protocol. Am J Sports Med. 2007;35(5):770–9. doi: 10.1177/0363546506298580. [DOI] [PubMed] [Google Scholar]
- 53.Contreras ME, Dani WS, Endges WK, et al. Arthroscopic treatment of the snapping iliopsoas tendon through the central compartment of the hip: a pilot study. J Bone Joint Surg Br. 2010;92(6):777–80. doi: 10.1302/0301-620X.92B6.22797. [DOI] [PubMed] [Google Scholar]
- 54.Beaton LE, Anson BJ. The relation of the sciatic nerve and of its subdivisions to the piriformis muscle. Anat Rec. 1937;70(1):1–5. doi: 10.1002/ar.1090700102. [DOI] [Google Scholar]
- 55.Byrd JWT. Piriformis syndrome. Oper Techn Sport Med. 2005;13(1):71–9. doi: 10.1053/j.otsm.2004.09.008. [DOI] [Google Scholar]
- 56.Martin HD, Shears SA, Johnson JC, et al. The endoscopic treatment of sciatic nerve entrapment/deep gluteal syndrome. Arthroscopy. 2011;27(2):172–81. doi: 10.1016/j.arthro.2010.07.008. [DOI] [PubMed] [Google Scholar]
- 57.Miller SL, Gill J, Webb GR. The proximal origin of the hamstrings and surrounding anatomy encountered during repair. A cadaveric study. J Bone Joint Surg Am. 2007;89(1):44–8. doi: 10.2106/JBJS.F.00094. [DOI] [PubMed] [Google Scholar]
- 58.McCrory P, Bell S. Nerve entrapment syndromes as a cause of pain in the hip, groin and buttock. Sports Med. 1999;27(4):261–74. doi: 10.2165/00007256-199927040-00005. [DOI] [PubMed] [Google Scholar]
- 59.Benson ER, Schutzer SF. Posttraumatic piriformis syndrome: diagnosis and results of operative treatment. J Bone Joint Surg Am. 1999;81(7):941–9. [PubMed] [Google Scholar]
- 60.Martin HD, Hatem M, Palmer IJ. Endoscopic sciatic nerve decompression: operative technique. Oper Techn Sport Med. 2012;20(4):325–32. doi: 10.1053/j.otsm.2012.09.005. [DOI] [Google Scholar]
- 61.Barton PM. Piriformis syndrome: a rational approach to management. Pain. 1991;47(3):345–52. doi: 10.1016/0304-3959(91)90227-O. [DOI] [PubMed] [Google Scholar]
- 62.Meknas K, Kartus J, Letto JI, et al. A 5-year prospective study of non-surgical treatment of retro-trochanteric pain. Knee Surg Sports Traumatol Arthrosc. 2009;17(8):996–1002. doi: 10.1007/s00167-009-0750-z. [DOI] [PubMed] [Google Scholar]
- 63.Dezawa A, Kusano S, Miki H. Arthroscopic release of the piriformis muscle under local anesthesia for piriformis syndrome. Arthroscopy. 2003;19(5):554–7. doi: 10.1053/jars.2003.50158. [DOI] [PubMed] [Google Scholar]
- 64.Hwang DS, Kang C, Lee JB, et al. Arthroscopic treatment of piriformis syndrome by perineural cyst on the sciatic nerve: a case report. Knee Surg Sports Traumatol Arthrosc. 2010;18(5):681–4. doi: 10.1007/s00167-009-1013-8. [DOI] [PubMed] [Google Scholar]
- 65.Larson CM, Kelly BT, Stone RM. Making a case for anterior inferior iliac spine/subspine hip impingement: three representative case reports and proposed concept. Arthroscopy. 2011;27(12):1732–7. doi: 10.1016/j.arthro.2011.10.004. [DOI] [PubMed] [Google Scholar]
- 66.Pan H, Kawanabe K, Akiyama H, et al. Operative treatment of hip impingement caused by hypertrophy of the anterior inferior iliac spine. J Bone Joint Surg Br. 2008;90(5):677–9. doi: 10.1302/0301-620X.90B5.20005. [DOI] [PubMed] [Google Scholar]
- 67.Hetsroni I, Larson CM, Dela Torre K, et al. Anterior inferior iliac spine deformity as an extra-articular source for hip impingement: a series of 10 patients treated with arthroscopic decompression. Arthroscopy. 2012;28(11):1644–53. doi: 10.1016/j.arthro.2012.05.882. [DOI] [PubMed] [Google Scholar]
- 68.Rajasekhar C, Kumar KS, Bhamra MS. Avulsion fractures of the anterior inferior iliac spine: the case for surgical intervention. Int Orthop. 2001;24(6):364–5. doi: 10.1007/s002640000184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Matsuda DK, Calipusan CP. Adolescent femoroacetabular impingement from malunion of the anteroinferior iliac spine apophysis treated with arthroscopic spinoplasty. Orthopedics. 2012;35(3):e460–3. doi: 10.3928/01477447-20120222-44. [DOI] [PubMed] [Google Scholar]
- 70.Duffy P, Masri BA, Garbuz D, Duncan CP. Evaluation of patients with pain following total hip replacement. Instr Course Lect. 2006;55:223–32. [PubMed] [Google Scholar]
- 71.Bricteux S, Beguin L, Fessy MH. Iliopsoas impingement in 12 patients with a total hip arthroplasty. Rev Chir Orthop Reparatrice Appar Mot. 2001;87(8):820–5. [PubMed] [Google Scholar]
- 72.Lachiewicz PF, Kauk JR. Anterior iliopsoas impingement and tendinitis after total hip arthroplasty. J Am Acad Orthop Surg. 2009;17(6):337–44. doi: 10.5435/00124635-200906000-00002. [DOI] [PubMed] [Google Scholar]
- 73.Malik A, Maheshwari A, Dorr LD. Impingement with total hip replacement. J Bone Joint Surg Am. 2007;89(8):1832–42. doi: 10.2106/JBJS.F.01313. [DOI] [PubMed] [Google Scholar]
- 74.Van Riet A, De Schepper J, Delport HP. Arthroscopic psoas release for iliopsoas impingement after total hip replacement. Acta Orthop Belg. 2011;77(1):41–6. [PubMed] [Google Scholar]
- 75.Pattyn C, Verdonk R, Audenaert E. Hip arthroscopy in patients with painful hip following resurfacing arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2011;19(9):1514–20. doi: 10.1007/s00167-011-1463-7. [DOI] [PubMed] [Google Scholar]
- 76.Bajwa AS, Villar RN. Arthroscopy of the hip in patients following joint replacement. J Bone Joint Surg Br. 2011;93(7):890–6. doi: 10.1302/0301-620X.93B7.24902. [DOI] [PubMed] [Google Scholar]