

Abstract
Background
Untreated celiac disease is traditionally believed to be associated with malabsorption and underweight. However, studies describing body mass index (BMI) in individuals at the time of diagnosis have shown contradictory results. We investigated the differences in weight, height, and BMI in 12- year-old children with screening-detected celiac disease compared to their healthy peers.
Methods
In a population-based screening study of 12,632 12-year-old children, blood samples were analyzed for markers of celiac disease. Children with elevated markers were referred for a small bowel biopsy. Weight and height were measured in 239 out of 242 children with screening-detected celiac disease (57.3% girls) and in 12,227 children without celiac disease (48.5% girls). BMI was categorized according to the International Obesity Task Force. Age- and sex-specific cut-off points for underweight, normal weight, and overweight were used.
Results
Children with celiac disease weighed less and were shorter than their peers (median weight 45.2 kg, interquartile range (IQR) 40.2–52.2 kg vs. 47.0 kg, IQR 41.1–54.4 kg, respectively, p = 0.01; median height 156.5 cm, IQR 151.0–162.0 cm vs. 157.5 cm, IQR 152.0–163.0 cm, respectively, p = 0.04). In comparing those with celiac disease to their healthy peers, 4.2% vs. 5.2% were underweight, 82.0% vs. 72.8% were normal weight, and 13.8% vs. 21.9% were overweight, respectively. There was no association between being underweight and the risk of having undiagnosed celiac disease (Odds ratio (OR) 1.3, 95% CI 0.7–2.4), but the risk was significantly lower among overweight children (OR 0.56, 95% CI 0.4–0.8). Median BMI was slightly lower among the children with screening-detected celiac disease compared to their healthy peers (18.6 kg/m2, IQR 17.1–19.8 kg/m2 vs. 18.8 kg/m2, IQR 17.2–21.1 kg/m2, respectively, p = 0.05), but most of the celiac disease cases had a normal BMI.
Conclusions
At a population level, children with celiac disease weigh less, are shorter, and have a lower BMI compared to their peers without celiac disease, and this emphasizes the importance of early recognition and treatment of the condition. However, at an individual level, growth parameters are not reliable in establishing the diagnosis.
Keywords: Body mass index, Celiac disease, Children, Height, Screening study, Weight
Background
Celiac disease is one of the most common chronic diseases in childhood and affects approximately 0.5%–3% of the population in the Western world [1-3]. It is characterized by an autoimmune response triggered by gluten and other environmental cofactors that leads to small-intestinal mucosal injury [4]. The disease can have its onset at any age throughout life, and its clinical expression is heterogeneous. The classic presentation of celiac disease is commonly described as diarrhea, abdominal distention, malnutrition, and failure to thrive [5-7]. Younger children often present with gastrointestinal symptoms and weight loss, but the clinical presentation seems to have changed in recent decades and the proportions of patients suffering from classical gastrointestinal symptoms, including weight loss, are decreasing. More patients now suffer from extra-intestinal symptoms or have no symptoms and are found in screening studies [8,9]. In contrast to previous beliefs, it is now well established that many adult patients with celiac disease have a high or normal body mass index (BMI) at diagnosis [10-13]. Some studies show that BMI increases on a gluten-free diet, especially in those who adhere closely to the diet [14]. However, other studies describing BMI in individuals at diagnosis of celiac disease and/or after introduction of a gluten-free diet have shown contradictory results. Few studies examining BMI and other growth parameters have been performed in children, and the findings of those studies have been inconclusive [15-17].
The main objective of this study was to examine weight, height, and BMI in 12-year-old children with untreated screening-detected celiac disease and to compare these parameters with their healthy peers.
Methods
Study design
The present investigation was based on the children included in the ETICS study (Exploring the Iceberg of Celiacs in Sweden). Details of the celiac disease screening strategy and descriptions of the included children have been published previously [3,18]. In brief, ETICS is a school-based cross-sectional multicenter national screening study for celiac disease in 12-year-old children and is part of the Prevent-CD European project [19]. Participating families gave their signed informed consent before the children were enrolled. Children with an existing diagnosis of celiac disease (n = 96) were excluded from this study. Blood samples from all children were analyzed for anti-human tissue transglutaminase (tTG) and, if borderline values were obtained, also for endomysial antibodies. Children with values above a predefined cut-off were referred to the closest pediatric clinic for a small-intestinal biopsy [20,21]. Criteria for diagnosis were Marsh 3a-c enteropathy or a combination of Marsh 1 and Marsh 2 enteropathy, HLA-DQ2/DQ8 haplotype, and symptoms and/or signs compatible with celiac disease [21]. Genotyping for HLA alleles encoding for HLA-DQ2/DQ8 was performed by oligonucleotide probe hybridization and was verified in all screening-detected cases. The study was approved by the Regional Ethical Review Board of Umeå University, Umeå, Sweden.
Anthropometric assessment
Weight and height were measured at the time of the screening for celiac disease according to standard procedures. All school nurses were given uniform instructions on how to carry out these measurements. The scales were all recently calibrated, and a wall-mounted stadiometer was used for measuring height. The children wore light clothing and no shoes and were measured with their body in a straight line and their head in an appropriate position. BMI was calculated as weight (kg) divided by the square of the height (m2) and categorized using the cut-off points recommended by the International Obesity Task Force (IOTF) [22]. Age- and sex-specific cut-off points corresponding to the adult BMI value of <18.5 (defined as underweight) and ≥ 25 (defined as overweight) were used. As a reference, adult BMI 25 corresponds to 21.22 for 12-year-old boys and to 21.68 for 12-year-old girls and adult BMI 18.5 corresponds to 15.35 for 12-year-old boys and to 15.62 for 12-year-old girls [22,23].
Statistical analysis
Microsoft Access 2010 (Microsoft, Redmond, WA) was used for handling the ETICS database, and statistical analysis was performed using SPSS Statistics for Windows (Version 21.0, IBM Corp, Armonk, NY). Continuous variables are reported as the median and interquartile range (IQR) because of unequal sample size and skewed distributions. The 25th and 75th percentiles are described in the text. Categorical variables are reported as the number and percentage of subjects with the characteristic of interest. Between-group comparisons were performed with the Wilcoxon–Mann–Whitney test for continuous variables and with chi-square or Fisher’s exact test for categorical variables as appropriate. These tests were performed on the whole group as well as after stratifications. Univariate logistic regression models tested the odds of having celiac disease while being underweight or being overweight. Statistical significance was defined as a two-sided P ≤ 0.05 or an odds ratio (OR) with a 95% confidence interval (CI) not including 1.
Results
In total, 12,632 children (69% of those invited) participated. Details regarding the prevalence of celiac disease have been published previously [3,18]. In total, 242 newly detected celiac disease cases were identified within the study as a result of the screening. Weight and height were available in 239 (99%) children with newly detected celiac disease (57.3% girls) and in 12,227 (99%) of the study participants without celiac disease (48.5% girls) (Figure 1).
Figure 1.
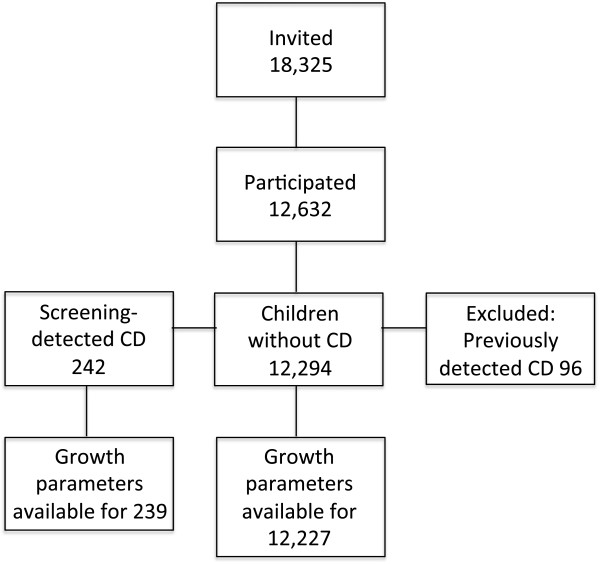
Flowchart depicting the screening procedure. Cross-sectional screenings performed in 12-year-old children across Sweden to investigate the prevalence of celiac disease (CD) and to assess the growth parameters in comparison with healthy children. The numbers of children are given in the boxes.
The children with screening-detected celiac disease weighed less on average compared to the children without celiac disease (median weight 45.2 kg, IQR 41.1–54.4 kg vs. 47.0 kg, IQR 40.2–52.2 kg, p = 0.01) (Table 1). There was no statistically significant difference in weight between girls and boys within the celiac disease group (p = 0.86). The children with screening-detected celiac disease were also significantly shorter compared to the children without celiac disease (median height 156.5 cm, IQR 151.0–162.0 cm vs. 157.5 cm, IQR 152.0–163.0 cm, p = 0.04).
Table 1.
Comparison of BMI, weight and height between children without celiac disease (CD) and children with screening-detected celiac disease
| Groups, n (%) | No CD n = 12,227 | CD n = 239 | P-value a |
|---|---|---|---|
| Girls, n (%) |
5932 (48.5) |
137 (57.3) |
|
| Age-and sex-adjusted BMI, n (%) |
|
|
|
| <18.5 kg/m2 |
641 (5.2) |
10 (4.2) |
|
| 18.5-24.9 kg/m2 |
8906 (72.8) |
196 (82.0) |
|
| ≥25 kg/m2 |
2680 (21.9) |
33 (13.8) |
0.01* |
| BMI (kg/m2) median (IQR) |
|
|
|
| All |
18.8 (3.85) |
18.6 (3.15) |
0.05* |
| Girls |
18.8 (3.84) |
18.6 (3.37) |
0.22 |
| Boys |
18.8 (3.88) |
18.6 (2.67) |
0.13 |
| Weight (kg) median (IQR) |
|
|
|
| All |
47.0 (13.3) |
45.2 (12.0) |
0.01* |
| Girls |
47.1 (12.9) |
44.9 (13.0) |
0.07 |
| Boys |
47.0 (13.6) |
46.2 (11.0) |
0.09 |
| Height (cm) median (IQR) |
|
|
|
| All |
157.5 (11.0) |
156.5 (11.0) |
0.04* |
| Girls |
158.0 (9.9) |
156.0 (10.4) |
0.04* |
| Boys | 157.0 (11.2) | 157.0 (12.6) | 0.32 |
aStatistical significance defined as P ≤ 0.05 and marked with *.
The distribution of underweight, normal weight, and overweight differed significantly between the groups. Among the patients with screening-detected celiac disease, 4.2% were underweight, 82.0% were of normal weight, and 13.8% were overweight. In the group of healthy children, the proportions were 5.2%, 72.8% and 21.9%, respectively (Table 1). Using children with normal weight as a reference group, there was no association between being underweight and the risk of having undiagnosed celiac disease (OR 1.3, 95% CI 0.7–2.4). However, the risk of having celiac disease was significantly lower among overweight children (OR 0.56, 95% CI 0.4–0.8).
BMI was slightly lower among the children with screening-detected celiac disease compared to their healthy peers (median 18.6 kg/m2, IQR 17.1–19.8 kg/m2 vs. 18.8 kg/m2, IQR 17.2–21.1 kg/m2, p = 0.05).
Among the girls with screening-detected celiac disease (n = 137), 2.2% were underweight, 83.9% were of normal weight, and 13.9% were overweight compared to 6.6%, 73.8%, and 19.8% of their healthy peers, respectively (p = 0.02). The girls with screening-detected celiac disease were also significantly shorter compared to their healthy peers (median height 156.0 cm, IQR 151.6–162.0 cm vs. 158.0 cm, IQR 153.0–162.9 cm, p = 0.039). Among the boys with screening-detected celiac disease (n = 102), 6.9% were underweight, 79.4% were of normal weight, and 13.7% were overweight compared to 4.0%, 72.0%, and 24.1%, respectively, among their healthy peers (p = 0.03). Over all, the distribution of underweight, normal weight, and overweight in sex-stratified subgroups showed a similar pattern as the whole group (Table 2).
Table 2.
Comparison of BMI between girls and boys without celiac disease (CD) and girls and boys with screening-detected celiac disease
| Groups, n (%) | No CD | CD | P-value a |
|---|---|---|---|
| Girls |
5932 (48.5) |
137 (57.3) |
|
| Age- and sex-adjusted BMI |
|
|
|
| <18.5 kg/m2 |
391 (6.6) |
3 (2.2) |
|
| 18.5-24.9 kg/m2 |
4376 (73.8) |
115 (83.9) |
|
| ≥25 kg/m2 |
1165 (19.6) |
19 (13.9) |
0.02* |
| Boys |
6295 (51.5) |
102 (42.7) |
|
| Age- and sex-adjusted BMI |
|
|
|
| <18.5 kg/m2 |
250 (4.0) |
7 (6.9) |
|
| 18.5-24.9 kg/m2 |
4530 (72.0) |
81 (79.4) |
|
| ≥25 kg/m2 | 1515 (24.0) | 14 (13.7) | 0.03* |
aStatistical significance defined as P ≤ 0.05 and marked with *.
Discussion
In this large population-based celiac disease screening study, we found that children with untreated celiac disease were moderately shorter, weighed less, and had a slightly lower BMI compared to their healthy peers. Even though having undiagnosed celiac disease was not associated with being underweight, only a few were overweight and the majority of the children with screening-detected celiac disease had a normal weight.
In 2004, an American study found that children with tTG-positive screening-identified celiac disease weighed less compared to healthy children and other recent studies have found that children with celiac disease are less frequently overweight or obese and more often underweight than controls [15,17]. Some studies in patients with celiac disease have also found other factors associated with low BMI such as the extent of mucosal injury, presentation with diarrhea and female sex [12]. Studies performed in adults have shown similar results as in this study with regard to BMI [10,24].
Even if celiac disease is classically associated with malabsorption and weight loss, one must bear in mind that children with undiagnosed celiac disease can have different body compositions. The fact that the proportion of underweight children with celiac disease in our study was only 4.2% emphasizes that celiac disease should not be considered primarily as a malabsorption disorder. In addition, although celiac disease was found in this study to be distinctly less common among overweight children, being overweight does not necessarily rule out celiac disease.
In some studies, overweight has been found to be more common in boys with celiac disease than in girls [12,25]. In contrast, the same weight pattern was found to apply to both boys and girls and no indications of any gender differences in the proportion of overweight within the celiac disease group were found in the present study. In the current study, girls with celiac disease were significantly shorter than their healthy peers. This is consistent with other studies, including one study conducted in Finland that found that the screening-detected adolescent celiac disease subjects were not only shorter but one third also had nutritional abnormalities [16,26]. Even more extensive nutritional deficiencies were found in a recently conducted Dutch study in which 7.5% of the individuals with celiac disease were found to be underweight but the nutritional deficiencies were present even in obese patients [27]. This is important to keep in mind when considering the need for more active screening for the disease in order to prevent the progression of nutritional deficiencies.
The results regarding height are more inconsistent than those for weight. In some studies, adult men with celiac disease have been found to be shorter [24,28], but another study indicated that the mean adult height of patients with celiac disease was the same as that of the general population. In a subgroup analysis, reduced height was observed in the older, but not younger, birth cohorts with celiac disease [29]. Some other studies found that celiac disease diagnosed in childhood results in catch-up growth once a gluten-free diet is introduced, but still others found that men and women with celiac disease were shorter compared to controls [30-32]. Part of the differences found regarding height in the above-mentioned studies might be explained by differences in the investigated age span in the study populations. In the present study, it is likely that a majority of the girls at 12 years of age have reached the onset of puberty and that they are in the middle of their growth spurt. The onset of puberty corresponds to a biological (i.e., skeletal) age of approximately 11 years in girls and 13 years in boys. The timing of the pubertal growth spurt occurs earlier in girls and tends not to reach the same magnitude as that of boys. Girls average a peak growth velocity of 9 cm/year at age 12 and a total gain in height of 25 cm during the pubertal growth period. Boys attain an average peak growth velocity of 10.3 cm/year – which occurs about 2 years later than in girls – and gain 28 cm in height during the pubertal growth period [33-35]. This means that the majority of the girls participating in this study were in the middle of their peak height velocity when the study took place. It is possible, therefore, that untreated celiac disease gives them worse preconditions for the growth spurt or that the disease influences the onset of puberty and results in a delay in peak growth velocity. Additional epidemiologic research is needed to confirm these results, and more research needs to be done to understand the pathogenesis of short stature in patients with celiac disease.
The present investigation was based on a nationwide, contemporary study on celiac disease in 12,632 children. The screening-detected cases were ascertained by small-intestinal biopsies and HLA-DQ testing. However, the study has some limitations that merit consideration. First, the growth parameters, and thus the BMI, of the children were available only at the time of the screening. Repeated weight and height measurements following the initiation of a gluten-free diet would permit an evaluation of the effect of the diet on the nutritional status of the children. Although this is an important question that warrants further research, it is beyond the scope of this study. Furthermore, evaluating growth parameters at the time of the screening without the children knowing their diagnosis provides only a snapshot of the nutritional status in these children with untreated celiac disease compared to their healthy peers. Second, although the screening study included 12,632 children, statistical power might still constitute a limitation of the current study. There were only 239 children with celiac disease in this cohort, and only 102 were boys. The relatively low number of children with celiac disease might explain why no statistically significant differences in anthropometric measurements were found in this subgroup. However, at a population level, the growth parameters tended to be affected in the same way in boys as in girls and in the celiac disease cohort as a whole.
Overall, this study still has several strengths. To the best of our knowledge, it is the first large cross-sectional study where all the children enrolled were of the same age. The weight and height measurements were also performed according to standard procedures (as opposed to self-reported), and this makes them very reliable and comparable. Also, the celiac disease diagnosis was established using state of the art techniques including serologic markers and small-intestinal biopsies.
Conclusions
The majority of the children with screening-detected celiac disease were of normal weight and there was no association between being underweight and the risk of having undiagnosed celiac disease. At a population level, the 12-year-old children with screening-detected celiac disease weighed less and were shorter compared to their peers without celiac disease, and this indicates a need to detect and treat celiac disease. However, at the individual level growth parameters are not reliable in predicting celiac disease. Although celiac disease is less common in the overweight subgroup, being overweight does not necessarily rule out celiac disease.
Abbreviations
tTG: Transglutaminase; BMI: Body mass index; OR: Odds ratio; CI: Confidence interval.
Competing interest
The authors declare no competing interests.
Authors’ contributions
AI and AC designed the study and were responsible for the overall supervision of the study. All authors participated in the development of the study protocol and in carrying out the study, and each was responsible for one of the study sites. MP, LH and SH performed the clinical evaluations. AR performed quality control on the clinical data. FN was responsible for the database and for statistical support. MP and AM performed the data analyses and drafted the manuscript. All authors participated in the data interpretation and critical revision of the manuscript and approved its final version.
Pre-publication history
The pre-publication history for this paper can be accessed here:
Contributor Information
Maria van der Pals, Email: maria.vanderpals@med.lu.se.
Anna Myléus, Email: anna.myleus@epiph.umu.se.
Fredrik Norström, Email: Fredrik.norstrom@epiph.umu.se.
Solveig Hammarroth, Email: solveig.hammarroth@tiohundra.se.
Lotta Högberg, Email: lotta.hogberg@lio.se.
Anna Rosén, Email: anna.rosen@epiph.umu.se.
Anneli Ivarsson, Email: anneli.ivarsson@epiph.umu.se.
Annelie Carlsson, Email: annelie.carlsson@med.lu.se.
Acknowledgements
We thank all participating children and their families and all personnel working with the study including research nurses, laboratory personnel, administrative staff, and collaborators within the school health services and pediatric departments. The study was performed in cooperation with the county councils of Västerbotten, Stockholm, Östergötland, Kronoberg, and Skåne and was undertaken within the Centre for Global Health at Umeå University with support from FAS, the Swedish Council for Working Life and Social Research. The study was funded by the Swedish Research Council (grants 521-2004-7093 and 521-2007-2953), the Swedish Research Council for Environment, Agricultural Sciences and Spatial Planning (grants 222-2004-1918 and 222-2007-1394), and the Swedish Council for Working Life and Social Research (grants 2005-0802). In addition, a minor contribution was made by the Skåne County Council. The study was part of the European Union-supported project FP6-2005-FOOD-4B-36383-PREVENTCD. Phadia (Freiburg, Germany) and Eurospital SpA (Trieste, Italy) contributed with analysis of coded serum samples.
References
- Green PH, Cellier C. Celiac disease. N Engl J Med. 2007;357(17):1731–1743. doi: 10.1056/NEJMra071600. [DOI] [PubMed] [Google Scholar]
- Mustalahti K, Catassi C, Reunanen A, Fabiani E, Heier M, McMillan S, Murray L, Metzger MH, Gasparin M, Bravi E, Mäki M. and the members of the coeliac EU Cluster, Epidemiology. The prevalence of celiac disease in Europe: results of a centralized, international mass screening project. Ann Med. 2010;42(8):587–595. doi: 10.3109/07853890.2010.505931. [DOI] [PubMed] [Google Scholar]
- Myleus A, Ivarsson A, Webb C, Danielsson L, Hernell O, Hogberg L, Karlsson E, Lagerqvist C, Norstrom F, Rosen A, Sandstrom O, Stenhammar L, Stenlund H, Wall S, Carlsson A. Celiac disease revealed in 3% of Swedish 12-year-olds born during an epidemic. J Pediatr Gastroenterol Nutr. 2009;49(2):170–176. doi: 10.1097/MPG.0b013e31818c52cc. [DOI] [PubMed] [Google Scholar]
- Green PH, Jabri B. Coeliac disease. Lancet. 2003;362(9381):383–391. doi: 10.1016/S0140-6736(03)14027-5. [DOI] [PubMed] [Google Scholar]
- Lionetti E, Catassi C. New clues in celiac disease epidemiology, pathogenesis, clinical manifestations, and treatment. Int Rev Immunol. 2011;30(4):219–231. doi: 10.3109/08830185.2011.602443. [DOI] [PubMed] [Google Scholar]
- Zawahir S, Safta A, Fasano A. Pediatric celiac disease. Curr Opin Pediatr. 2009;21(5):655–660. doi: 10.1097/MOP.0b013e32832f5b9d. [DOI] [PubMed] [Google Scholar]
- Gee S. On the coeliac affection. St Bart Hosp Rep. 1890. pp. 17–20.
- Murray JA, Van Dyke C, Plevak MF, Dierkhising RA, Zinsmeister AR, Melton LJ 3rd. Trends in the identification and clinical features of celiac disease in a North American community, 1950-2001. Clin Gastroenterol Hepatol. 2003;1(1):19–27. doi: 10.1053/jcgh.2003.50004. [DOI] [PubMed] [Google Scholar]
- Rampertab SD, Pooran N, Brar P, Singh P, Green PH. Trends in the presentation of celiac disease. The American journal of medicine. 2006;119(4):355. doi: 10.1016/j.amjmed.2005.08.044. e359-314. [DOI] [PubMed] [Google Scholar]
- Olen O, Montgomery SM, Marcus C, Ekbom A, Ludvigsson JF. Coeliac disease and body mass index: a study of two Swedish general population-based registers. Scand J Gastroenterol. 2009;44(10):1198–1206. doi: 10.1080/00365520903132013. [DOI] [PubMed] [Google Scholar]
- Dickey W, Kearney N. Overweight in celiac disease: prevalence, clinical characteristics, and effect of a gluten-free diet. Am J Gastroenterol. 2006;101(10):2356–2359. doi: 10.1111/j.1572-0241.2006.00750.x. [DOI] [PubMed] [Google Scholar]
- Cheng J, Brar PS, Lee AR, Green PH. Body mass index in celiac disease: beneficial effect of a gluten-free diet. J Clin Gastroenterol. 2010;44(4):267–271. doi: 10.1097/MCG.0b013e3181b7ed58. [DOI] [PubMed] [Google Scholar]
- Ukkola A, Maki M, Kurppa K, Collin P, Huhtala H, Kekkonen L, Kaukinen K. Changes in body mass index on a gluten-free diet in coeliac disease: a nationwide study. Eur J Intern Med. 2012;23(4):384–388. doi: 10.1016/j.ejim.2011.12.012. [DOI] [PubMed] [Google Scholar]
- Kabbani TA, Goldberg A, Kelly CP, Pallav K, Tariq S, Peer A, Hansen J, Dennis M, Leffler DA. Body mass index and the risk of obesity in coeliac disease treated with the gluten-free diet. Aliment Pharmacol Ther. 2012;35(6):723–729. doi: 10.1111/j.1365-2036.2012.05001.x. [DOI] [PubMed] [Google Scholar]
- Brambilla P, Picca M, Dilillo D, Meneghin F, Cravidi C, Tischer MC, Vivaldo T, Bedogni G, Zuccotti GV. Changes of body mass index in celiac children on a gluten-free diet. Nutr Metab Cardiovasc Dis. 2013;23(3):177–182. doi: 10.1016/j.numecd.2011.10.002. [DOI] [PubMed] [Google Scholar]
- Haapalahti M, Kulmala P, Karttunen TJ, Paajanen L, Laurila K, Maki M, Mykkanen H, Kokkonen J. Nutritional status in adolescents and young adults with screen-detected celiac disease. J Pediatr Gastroenterol Nutr. 2005;40(5):566–570. doi: 10.1097/01.mpg.0000154658.16618.f9. [DOI] [PubMed] [Google Scholar]
- Hoffenberg EJ, Emery LM, Barriga KJ, Bao F, Taylor J, Eisenbarth GS, Haas JE, Sokol RJ, Taki I, Norris JM, Rewers M. Clinical features of children with screening-identified evidence of celiac disease. Pediatrics. 2004;113(5):1254–1259. doi: 10.1542/peds.113.5.1254. [DOI] [PubMed] [Google Scholar]
- Ivarsson A, Myleus A, Norstrom F, van der Pals M, Rosen A, Hogberg L, Danielsson L, Halvarsson B, Hammarroth S, Hernell O, Karlsson E, Stenhammar L, Webb C, Sandström O, Carlsson A. Reduced prevalence of childhood celiac disease: an effect of changes in infant feeding? Pediatrics. 2013;131(3):687–694. doi: 10.1542/peds.2012-1015. [DOI] [PubMed] [Google Scholar]
- Hogen Esch CE, Rosen A, Auricchio R, Romanos J, Chmielewska A, Putter H, Ivarsson A, Szajewska H, Koning F, Wijmenga C, Troncone R, Mearin ML. PreventCD Study Group. The PreventCD Study design: towards new strategies for the prevention of coeliac disease. Eur J Gastroenterol Hepatol. 2010;22(12):1424–1430. doi: 10.1097/MEG.0b013e32833fe9ae. [DOI] [PubMed] [Google Scholar]
- Di Sabatino A, Corazza GR. Coeliac disease. Lancet. 2009;373(9673):1480–1493. doi: 10.1016/S0140-6736(09)60254-3. [DOI] [PubMed] [Google Scholar]
- Webb C, Halvarsson B, Norstrom F, Myleus A, Carlsson A, Danielsson L, Hogberg L, Ivarsson A, Karlsson E, Stenhammar L, Sandstrom O. Accuracy in celiac disease diagnostics by controlling the small-bowel biopsy process. J Pediatr Gastroenterol Nutr. 2011;52(5):549–553. doi: 10.1097/MPG.0b013e3181fa434f. [DOI] [PubMed] [Google Scholar]
- Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320(7244):1240–1243. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole TJ, Flegal KM, Nicholls D, Jackson AA. Body mass index cut offs to define thinness in children and adolescents: international survey. BMJ. 2007;335(7612):194. doi: 10.1136/bmj.39238.399444.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sonti R, Lebwohl B, Lewis SK, Abu Daya H, Klavan H, Aguilar K, Green PH. Men with celiac disease are shorter than their peers in the general population. Eur J Gastroenterol Hepatol. 2013;25(9):1033–1037. doi: 10.1097/MEG.0b013e328362e461. [DOI] [PubMed] [Google Scholar]
- Reilly NR, Aguilar K, Hassid BG, Cheng J, Defelice AR, Kazlow P, Bhagat G, Green PH. Celiac disease in normal-weight and overweight children: clinical features and growth outcomes following a gluten-free diet. J Pediatr Gastroenterol Nutr. 2011;53(5):528–531. doi: 10.1097/MPG.0b013e3182276d5e. [DOI] [PubMed] [Google Scholar]
- Bingley PJ, Williams AJ, Norcross AJ, Unsworth DJ, Lock RJ, Ness AR, Jones RW. Undiagnosed coeliac disease at age seven: population based prospective birth cohort study. BMJ. 2004;328(7435):322–323. doi: 10.1136/bmj.328.7435.322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wierdsma NJ, van der Schueren MA VB-d, Berkenpas M, Mulder CJ, Van Bodegraven AA. Vitamin and mineral deficiencies are highly prevalent in newly diagnosed celiac disease patients. Nutrients. 2013;5(10):3975–3992. doi: 10.3390/nu5103975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nusier MK, Brodtkorb HK, Rein SE, Odeh A, Radaideh AM, Klungland H. Serological screening for celiac disease in schoolchildren in Jordan. Is height and weight affected when seropositive? Ital J Pediatr. 2010;36:16. doi: 10.1186/1824-7288-36-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parnanen A, Kaukinen K, Helakorpi S, Uutela A, Lahdeaho ML, Huhtala H, Collin P, Maki M, Kurppa K. Symptom-detected and screen-detected celiac disease and adult height: a large cohort study. Eur J Gastroenterol Hepatol. 2012;24(9):1066–1070. doi: 10.1097/MEG.0b013e328355a468. [DOI] [PubMed] [Google Scholar]
- Damen GM, Boersma B, Wit JM, Heymans HS. Catch-up growth in 60 children with celiac disease. J Pediatr Gastroenterol Nutr. 1994;19(4):394–400. doi: 10.1097/00005176-199411000-00005. [DOI] [PubMed] [Google Scholar]
- Luciano A, Bolognani M, Di Falco A, Trabucchi C, Bonetti P, Castellarin A. [Catch-up growth and final height in celiac disease] Pediatr Med Chir. 2002;24(1):9–12. [PubMed] [Google Scholar]
- Cosnes J, Cosnes C, Cosnes A, Contou JF, Reijasse D, Carbonnel F, Beaugerie L, Gendre JP. [Undiagnosed celiac disease in childhood] Gastroenterol Clin Biol. 2002;26(6–7):616–623. [PubMed] [Google Scholar]
- Tanner JM, Whitehouse RH, Marshall WA, Carter BS. Prediction of adult height from height, bone age, and occurrence of menarche, at ages 4 to 16 with allowance for midparent height. Arch Dis Child. 1975;50(1):14–26. doi: 10.1136/adc.50.1.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls. Arch Dis Child. 1969;44(235):291–303. doi: 10.1136/adc.44.235.291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Arch Dis Child. 1970;45(239):13–23. doi: 10.1136/adc.45.239.13. [DOI] [PMC free article] [PubMed] [Google Scholar]