

Abstract
Endoscopic submucosal dissection (ESD) has been established as a standard treatment for early stage gastric cancer (EGC) in Japan and has spread worldwide. ESD has been used not only for EGC but also for early esophageal and colonic cancers. However, ESD is associated with several adverse events, such as bleeding and perforation, which requires more skill. Adequate tissue tension and clear visibility of the tissue to be dissected are important for effective and safe dissection. Many ESD methods using traction have been developed, such as clip-with-line method, percutaneous traction method, sinker-assisted method, magnetic anchor method, external forceps method, internal-traction method, double-channel-scope method, outerroute method, double-scope method, endoscopic-surgical-platform, and robot-assisted method. Each method has both advantages and disadvantages. Robotic endoscopy, enabling ESD with a traction method, will become more common due to advances in technology. In the near future, simple, noninvasive, and effective ESD using traction is expected to be developed and become established as a worldwide standard treatment for superficial gastrointestinal neoplasias.
Keywords: Endoscopic submucosal dissection, Traction, Early gastric cancer, Early esophageal cancer, Early colonic cancer
Core tip: Endoscopic submucosal dissection (ESD) is associated with several adverse events, therefore, it requires more skill. Adequate tissue tension and clear visibility of the tissue to be dissected by traction are important for effective and safe ESD like surgery. Many ESD methods with traction have been reported until now. We review these ESD methods not only for early stage gastric cancer but also for early esophageal cancer or colonic cancer. We highlight both advantages and disadvantages of these methods.
INTRODUCTION
The possibility of expanding the use for endoscopic treatment for early stage gastric cancer (EGC) has been proposed[1]. Endoscopic submucosal dissection (ESD) for EGC has improved the rate of successful en bloc resection[2-6] compared to endoscopic mucosal resection (EMR). ESD enables resection en bloc for larger lesions, those with ulceration, and those located in difficult sites. Therefore, ESD has been established as a standard treatment for EGC in Japan and has spread worldwide. This method has been used not only for EGC but also for early esophageal and colonic cancers. However, ESD is associated with several complications, such as bleeding and perforation, which requires more skill. Traction is a standard method for maintaining a clear field of vision and to facilitate in the cutting of lesions during surgery. Likewise, adequate tissue tension and clear visibility of the tissue to be dissected by traction are important for effective and safe ESD[7-9].
The simplest method to achieve traction is position change[8,9]. The weight of the lesions and fluid injected to the submucosal layer enables the lesions to be hung from the wall of the gastrointestinal tract due to gravity. Endoscopic submucosal dissection becomes easier because the submucosal layer becomes wider and the field of vision becomes clearer. However, it is sometimes difficult because of limitation of position change and extension of the GI tract due to inner gas.
Recent reports on ESD with traction are described in this article (Table 1).
Table 1.
Advantages and disadvantages of the traction endoscopic submucosal dissection methods
|
Traction |
Other advantages | Other disadvantages | |||
| Push | Control of direction | Control of tension | |||
| ESD with traction in upper gastrointestinal tract | |||||
| Clip-with-line method[8,11-14] | - | - | + | Simple, easy | |
| Percutaneous-traction method[15-18] | + | + | + | Regrasping | Invasive |
| Magnetic anchor method[19,20] | + | + | + | Large and expensive | |
| External forceps method[21,22] | + | - | + | Regrasping, no need of assistant to hold the forceps | Care of mucosal damage |
| Internal traction method[23-25] | - | - | - | Easy | Roll back of mucosa |
| Spring-assisted ESD[26] | - | - | - | Easy | |
| Double-channel-scope method[28] | + | + | + | Regrasping | Synchronous movement of forceps and scope |
| R-scope[29-31] | + | + | + | Regrasping, swing of knife | Thicker and heavier scope, synchronous movement of forceps and scope |
| Outerroute method[33-38] | + | + | + | Regrasping | Synchronous movement of forceps and scope, small distance between forceps and knife |
| Double-scope method[10] | + | + | + | Regrasping | Interference of scopes, two light sources, double manpower |
| Morita[39] | + | + | + | Regrasping, a little interference of scopes | Thicher overtube, two light sources, double manpower |
| Higuchi[40] | + | + | + | Regrasping, one light source | Interference of scopes, double manpower |
| Robot-assisted method[42-44] | + | + | + | Regrasping | More complicated, no response of hemostasis |
| ESD with traction in colon and rectum | |||||
| Sinker-assisted method[45] | - | - | + | Easy | Retreival of scope |
| External forceps method[46] | + | - | + | Regrasping | Retreival of scope, only rectum |
| Internal traction method[47-50] | - | - | - | Easy | |
| Outerroute method[51] | + | + | + | Regrasping | Synchronous movement of forceps and scope |
| Double-scope method[52,53] | + | + | + | Regrasping | Two light sources and double manpower, interference of t scopes, lesions in only sigmoid colon and rectum |
| Fusaroli[54] | + | + | + | Regrasping, much cheaper, one light source | interference of scopes, lesions in only sigmoid colon and rectum |
| Endoscopic surgical platform[55] | + | + | + | Regrasping, freedom offering surgical triangulation | more complicated configuration with fixed instruments, only rectum |
ESD: Endoscopic submucosal dissection.
ESD WITH TRACTION IN UPPER GASTROINTESTINAL TRACT
Foremost, Hirao et al[10] reported on an EMR procedure using double endoscopes under general anesthesia, which was similar to surgery about 25 years ago. The lesion was grasped and lifted using grasping forceps through the thin endoscope, and submucosal dissection was done using a needle knife through the main scope (Figure 1). This method was revolutionary at that time; however, it was complicated and invasive. It required two endoscopic systems and more than two endoscopists and two assistants. Furthermore, two endoscopes couldnot be moved easily and independently because of their combined diameter. Thereafter, many kinds of less complicated and invasive methods have been developed.
Figure 1.
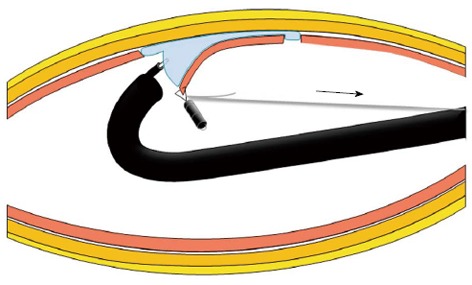
Schema of clip-with-line method.
Clip-with-line method
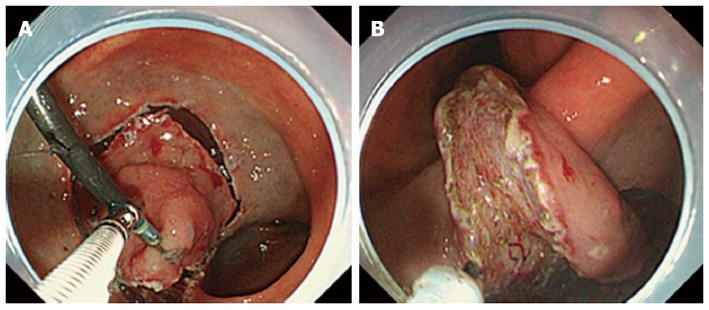
Lee et al[8] and Oyama et al[11] reported on the clip-with-line method, which is a simple, easy and useful method for traction not only for gastric ESD (Figure 1) but also for esophageal (Figure 2), colonic, and duodenal ESD. A long silk line is tied to the arm part of the clip, and the submucosal side of the target lesion is grasped. The line is pulled very gently. This method creates a clear field of vision. Jeon et al[12] and Ota et al[13] reported on similar methods. However, the traction direction by the clip-with-line method is limited. The pulley method is useful for pulling the line to the anal or opposite side (Figure 3). The line is captured by the second clip and fixed at the opposite side of the stomach. The first clip can be pulled to the anal side with the second clip acting like a pulley. Li et al[14] reported on similar method.
Figure 2.
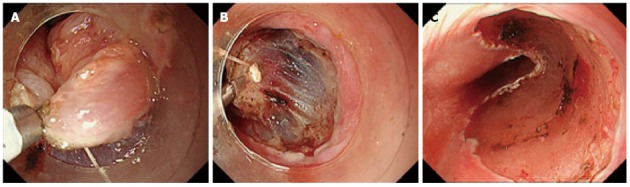
Clip-with-line method. A: Submucosal side of the target lesion in the esophagus was grasped using clip tied to long silk line; B: When the line was pulled very gently, submucosal layer was elevated; C: Lesion was dissected en bloc.
Figure 3.
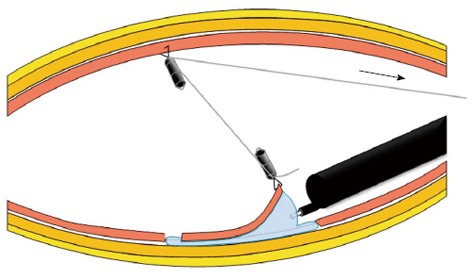
Schema of pulley method. The first clip with the line can be pulled to the anal side with the second clip, which is fixed at the opposite side.
Percutaneous-traction method
Kondo et al[15] reported on percutaneous traction-assisted EMR for gastric neoplasias, which requires a laparoscopic port with a trocar (Figure 4). A small snare is introduced into the gastric lumen through a gastric port to grasp and pull the lesions away from the muscularis propria. Thereafter, von Delius et al[16] reported on similar methods using a PEG-minitrocar for the gastric mucosa, and Chen et al[17] reported on methods using a looped insertion wire for the esophageal lesions. The loop end of the wire inserted through the PEG route was grasped using biopsy forceps and pulled into the esophagus. The wire was fixed on the proximal edge of the resected mucosa with a clip. The wire was gently pulled out through the PEG route, and the edge of the resected mucosa pulled away from the muscle layer. Nishiwaki et al[18] reported on transgastrostomic endoscopy-assisted ESD after percutaneous endoscopic gastrostomy. A small-caliber endoscope was inserted through the mature gastrostomy, and the edge of the resecting specimen was grasped to achieve traction. However, these methods are invasive and cannot be used for lesions on the anterior wall or high fundus of the stomach. They are also sometimes difficult to control the traction direction.
Figure 4.
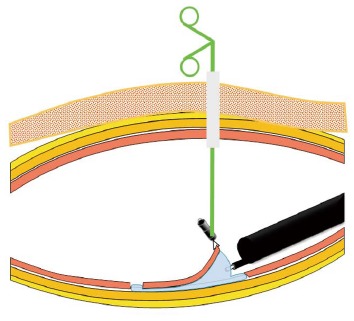
Schema of Percutaneous-traction method. A small snare is introduced into the gastric lumen through a gastric port to grasp and pull the lesions.
Magnetic anchor method
Kobayashi et al[19] and Gotoda et al[20] reported on a magnetic anchor system. The magnetic anchor with magnetic weight and microforceps is placed at the mucosal edge. ESD is done with suitable tension by using a high-power electromagnet placed outside the body. However, this system requires large and expensive instruments.
External forceps method
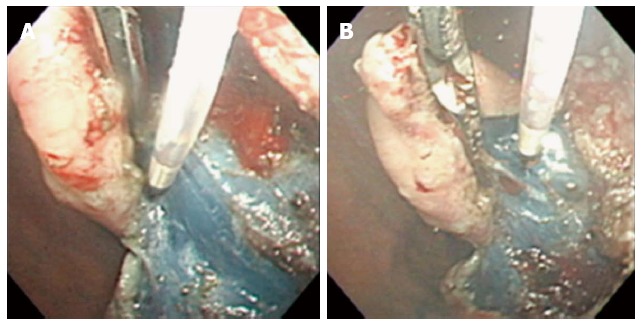
Imaeda et al[21,22] reported on ESD using external grasping forceps. An external pair of grasping forceps is used with a second pair (Figure 5A). This method is useful for creating a clear field of vision due to not only pull but also push and gravity, for lesions in the gastric body but also for those in the antrum (Figure 5B); however, for lesions in the cardia and the lesser curvature or posterior wall of the upper gastric body, this method is sometimes difficult. This procedure does not require any assistant to hold the forceps during ESD because the handle is locked. One endoscopist can easily and independently move the endoscope and forceps. Moreover, this procedure can also enable release and regrasping of the lesion with the forceps if the traction is not sufficient. Great care must be taken to avoid damaging the mucosa, especially at the esophagocardial junction, and the overtube is necessary. Although the traction direction is limited, the forceps can always be used to raise the grasped side of the lesion.
Figure 5.
Endoscopic submucosal dissection using external forceps. A: External grasping was anchored at distal margin of lesion in the lesser curvature of the antrum under control of endoscope and second grasping forceps; B: With gentle oral traction applied with external grasping forceps, submucosal layer was dissected in retroversion from aboral side.
Internal traction method
Several internal traction methods have been reported. A set of two clips connected by a rubber ring or a nylon line is used. The first clip connected by a rubber ring or nylon line is attached at the target part after circumferential incision. Parra-Blanco et al[23] reported the clip-band method. Matsumoto et al[24,25] reported on a new traction device called ‘‘medical ring’’. This device is mounted by connecting it to a hemoclip with 3-0 silk. The second clip is attached at the opposite sides of the lesions (Figure 6A). This method pulls up the lesion and opens the resection margin. Since lesions roll back, the traction direction and elevation of the submucosal layer is not sometimes sufficient. Sakurazawa et al[26] reported on spring-assisted ESD (Figure 6B). One end of the stainless-steel spring device (length 20 mm) is fitted with a polyurethane loop and the other end is fitted with a clip, which was attached to the opposite side. The spring lengthens by more than 10 fold in this range. However, the spring device is made of stainless steel, and its safety within the intestinal tract has not been established. Chen et al[27] reported on the nylon line method using 2 hemoclips. However, this method might not be applicable for neoplasms in the pylorus or cardia, where space is limited, and control of the traction power is sometimes difficult.
Figure 6.

Schema of Internal traction method. A: The second clip is attached at the opposite sides of the lesions; B: The second clip is attached at the opposite sides of the stomach.
Double-channel-scope method
A pair of grasping forceps inserted into a channel of a double-channel scope can create traction during ESD. Ishigooka et al[28] reported on endoscopic resection with injection of hypertonic saline epinephrine using a double-channel scope (S-ERHSE). Yonezawa et al[29] reported on ESD using an R-scope, which has two movable instrument channels: one moves a pair of grasping forceps vertically for lesions with traction and the other swings a cutting knife horizontally for dissection (Figure 7). Neuhaus et al[30] and Lee et al[31] also reported on this method using the R-scope, which facilitated ESD of large gastric areas. Even though the concept was good, the endoscope required a significant learning period to enable proficiency in its use. The forceps moves synchronously with the scope, therefore, it is sometimes difficult to control the traction direction. Hijikata et al[32] reported on ESD using the outer sheath of an injection needle. The bottom of the dissected mucosal layer is pushed and lifted up using the injection sheath through one channel to reveal the submucosal layer and ensure adequate traction, and submucosal dissection was conducted by an IT-knife through the other channel. However, a double-channel scope is thicker, heavier, and more difficult to manipulate than a single-channel endoscope. Moreover, since the grasping forceps or the outer sheath is inserted through the endoscope, it moves synchronously with the endoscope, which sometimes makes it difficult to control the traction direction and to cut the submucosal layer of larger lesions.
Figure 7.
Endoscopic submucosal dissection using double-channel R-scope. A: R-scope has two movable instrument channels: one moves grasping forceps vertically for lesion with traction and other swings cutting knife horizontally for dissection; B Cutting knife was horizontally swung.
Outerroute method
Motohashi et al[33,34] reported on ESD using the Impact Shooter®, which is mounted on the scope (Figure 8). The mucosa was hold with the forceps through the channel which was connected to the Impact Shooter®, and the submucosal tissue was dissected with the hook knife. However, the forceps moves synchronously with the endoscope and the distance between forceps and knife is not sufficient; therefore it is sometimes difficult to control the traction direction. Okamoto et al[35] and Tsao et al[36] reported on ESD using a clip with a nylon suture through a thin tube. The plastic sheath allows the endoscope to be easily maneuvered without interrupting the traction. Ohata et al[37] reported ESD using a biopsy forceps, which is straight when closed and curved when opened. It was inserted a long straw tube which was mounted on an overtube, and the edge of the targeted lesion was grasped and lift up. Teoh et al[38] reported on ESD using the Endolifter®, which consists of a retractable grasping forceps attached to a transparent cap by a hinge that allows simultaneous grasping, retracting, and lifting of the mucosa. However, these methods reduce the sideway movements of the endoscope due to retraction at a fixed point by the forceps, this in turn limits the maneuverability of the endoscope. The visual field is limited due to masking of the dissected part of the mucosa for large lesions.
Figure 8.

Schema of outerroute method.
Double-scope method
Since Hirao et al[10] reported on an EMR procedure using double endoscopes; several methods using a second thin endoscope have also been reported. The traction direction can be controlled easily with the double-scope method (Figure 9). However, the second scope sometimes limits the maneuverability of the main scope because of their combined diameter. Moreover, this method requires two light sources and more than two endoscopists and two assistants. Morita et al[39] described a double-endoscope method, which requires two light sources and a specially designed overtube with two channels to prevent interaction between two endoscopes. However, the overtube is thicker than the usual one. Higuchi et al[40] reported on another method without an overtube, which requires only one light source that can be transferred between two endoscopes, eliminating the problem of optical interference. After circumferential incision, the main scope is left in the stomach, and the light source is removed and attached to the thin endoscope. The thin endoscope is inserted along the main endoscope, and the lesion is grasped along its margin using grasping forceps. Thereafter, the light source is removed from the thin endoscope and reattached to the main endoscope, and submucosal dissection is done. However, the disadvantage is the same as the double scope method except for only requiring one light source. A thin trans-nasal endoscope-assisted ESD has been reported by Ahn et al[41]. This method has disadvantages, including nasal bleeding due to trans-nasal access, invasion due to double endoscopes, need for two endoscopists, and temporary hindrance of movement between endoscopes.
Figure 9.
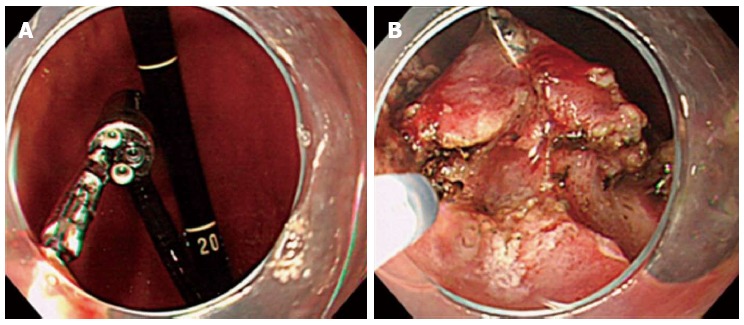
Endoscopic submucosal dissection using double-endoscopes. A: Lesion was grasped and lifted using grasping forceps through thin endoscope; B Submucosal dissection was done using needle knife through main scope.
Robot-assisted method
Ho et al[42], Wang et al[43], and Phee et al[44] reported on ESD using a Master and slave trans-luminal endoscopic robot (MASTER). The MASTER consists of three major components: a master robotic controller, a telesurgical workstation, and a slave manipulator. The system is designed to work with a therapeutic endoscope with two operating channels. The master controller is the human-machine interface that controls the slave manipulator, a unilateral electromechanical device that responds to the operator’s input and drives the end-effectors, grasper, and monopolar electrocautery hook. This method is similar to laparoscopic surgery. However, the disadvantage of the MASTER is its more complicated configuration with fixed instruments. If massive bleeding from a resected site occurs, it is necessary to change the therapeutic endoscope to a conventional endoscope to conduct hemostasis using hemoclips or hemostatic forceps.
ESD WITH TRACTION IN COLON AND RECTUM
ESD using traction for lesions on the colon and rectum is similar to that for lesions on the UGI tract. However, the lumen in the colon and rectum is narrow and bending. Moreover, for lesions in the proximal colon, reinsertion after retrieval of the endoscope is more time-consuming in some methods compared to that for lesions in the UGI tract. Therefore, lesions in only the rectum or sigmoid colon are indicated in some methods.
Sinker-assisted method
Saito et al[45] reported on sinker-assisted ESD for colorectal cancer. The sinker system is composed of a metallic clip attached to a 1-g sinker by a short nylon line. The metallic clip is attached to a target site at the edge of the exfoliated mucosa. The traction direction is controlled using gravity by changing the position of the body. A limitation of this method is the necessity of retrieving the scope to set up the sinker system.
External forceps method
Imaeda et al[46] reported on ESD using external biopsy forceps that are bendable (Figure 10). This procedure is similar to ESD using external grasping forceps for EGC[21,22]. The external bendable forceps was introduced with the help of the grasping forceps. After the external forceps was anchored at the anal margin of the lesion, with bending and gentle anal traction applied with the forceps, the lesion was elevated. However, it is used only for rectal cancers because of the difficulty in inserting and controlling the forceps in the colon.
Figure 10.
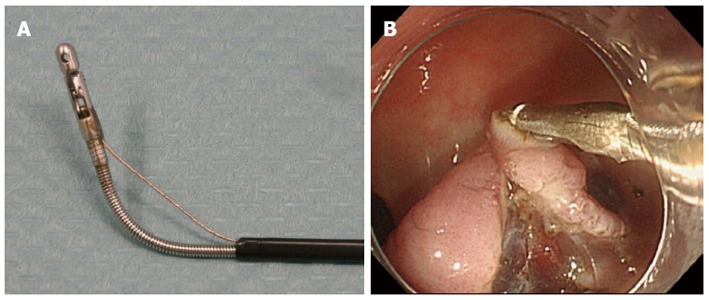
Endoscopic submucosal dissection using external forceps. A: Bendable biopsy forceps; B: Bending forceps and traction applied using forceps elevated lesion and widened submucosal layer.
Internal traction method
Sakamoto et al[47,48] reported on ESD using a S-O clip (Sakamoto and Osada clip). The S-O clip consists of a metal clip attached to the end of a spring or a rubber strip, its other end of which a double nylon loop is connected to. A spring S-O clip is attached to the edge of the exfoliated mucosa and a regular clip is used to grasp the distal nylon loop and applied to the colon wall opposite the lesion. Osada et al[49] also reported on ESD using a loop-attached rubber band, which consists of a circular rubber band connected to many nylon loops. Tomiki et al[50] reported on ESD using latex band traction. These methods are easy, safe, and noninvasive, and the instrument can be used at any location.
Outerroute method
Okamoto et al[51] reported on ESD using a clip with a nylon suture through a thin tube. This procedure is similar to ESD using a clip with a nylon suture through a thin tube for EGC[35]. However, this method needs a single balloon overtube, which enables the endoscope to be retrieved and inserted to set up the devices. The forceps moves synchronously with the endoscope and the distance between forceps and knife is not sufficient, therefore, this method limits the maneuverability of the endoscope. The visual field is limited due to masking of the dissected part of the mucosa for large lesions.
Double-scope method
Uraoka et al[52,53] reported on a double-scope method for large colorectal tumors. An endoclip is attached to the edge at the exfoliated mucosa, a second thin endoscope is then inserted into the lumen followed by removal of the primary endoscope. A snare is used to grasp the positioned endoclip and pull the lesion away from the muscle layer. Once again, the primary endoscope is inserted to the location of the lesion. However, this method is limited to the rectum and rectosigmoid colon because of the difficulty in intubating the second endoscope to the oral side of the distal sigmoid colon. It requires a second endoscopist to operate the traction system. It also may be difficult for treating larger lesions, like the circumferential ones because of insufficient space to maintain the necessary cutting line view provided by the traction system. Fusaroli et al[54] reported on a double-scope method using a prototype blind multi-bending thin probe with a working channel of 2.8 mm. It is much cheaper (when on the market) and more resistant to shear stress than a pediatric scope. However, it is limited to treating lesion on the rectum or sigmoid colon. Two endoscopists and three nurses (one for care of the patient, one for handling accessories for main endoscope and one for handling accessories for the second endoscope) are required.
Endoscopic surgical platform
Diana et al[55] reported on ESD using an endoscopic surgical platform, the Anubiscope®, equipped with two working channels for surgical instruments with four degrees of freedom offering surgical triangulation and ESD using a robotic version of the Anubiscope®. However, it is limited to treating lesion on the rectum, and is a more complicated configuration with fixed instruments.
PERSPECTIVES FOR FUTURE
Although many kinds of ESD methods with traction have been reported, each method has not only some advantages but also the other disadvantages. Some methods require retrieving the scope to set up devices, others are limited to lesions in certain areas, directions and tension of traction, and still others are somewhat complicated and invasive. If each knife or a grasping forceps be moved independently, as in surgery, and the direction and tension of traction can be controlled at will, ESD with traction might become easier and more flexible. A grasping forceps with flexible bending function, which is thinner than an ultrathin endoscope, may make ESD with traction easier.
If robotic endoscopy, which enables ESD with traction, advances in technology in the near future, it may make ESD easier, may approach to the lesions in any area regardless of gastric movement due to respiration, and may also enable endoscopic hemostasis.
CONCLUSION
Simple and flexible methods with traction can make ESD easier and safer. In the near future, simple, noninvasive, and effective ESD with traction is expected to be developed and become established as a standard treatment for superficial gastrointestinal neoplasias worldwide.
Footnotes
P- Reviewers: Jiang CP, Tadic M S- Editor: Wen LL L- Editor: A E- Editor: Zhang DN
References
- 1.Gotoda T, Yanagisawa A, Sasako M, Ono H, Nakanishi Y, Shimoda T, Kato Y. Incidence of lymph node metastasis from early gastric cancer: estimation with a large number of cases at two large centers. Gastric Cancer. 2000;3:219–225. doi: 10.1007/pl00011720. [DOI] [PubMed] [Google Scholar]
- 2.Ono H, Kondo H, Gotoda T, Shirao K, Yamaguchi H, Saito D, Hosokawa K, Shimoda T, Yoshida S. Endoscopic mucosal resection for treatment of early gastric cancer. Gut. 2001;48:225–229. doi: 10.1136/gut.48.2.225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Oyama T, Kikuchi Y. Aggressive endoscopic mucosal resection in the upper GI tract-hook knife EMR method. Minim Invasive Ther Allied Technol. 2002;11:291–295. doi: 10.1080/13645706.2003.11873728. [DOI] [PubMed] [Google Scholar]
- 4.Yahagi N, Fujishiro M, Kakushima N, Kobayashi K, Hashimoto T, Oka M, Iguchi M, Enomoto S, Ichinose M, Niwa H, et al. Endoscopic submucosal dissection for early gastric cancer using tip of an electrosurgical snare (thin type) Dig Endosc. 2004;16:34–38. [Google Scholar]
- 5.Yamamoto H, Kawata H, Sunada K, Sasaki A, Nakazawa K, Miyata T, Sekine Y, Yano T, Satoh K, Ido K, et al. Successful en-bloc resection of large superficial tumors in the stomach and colon using sodium hyaluronate and small-caliber-tip transparent hood. Endoscopy. 2003;35:690–694. doi: 10.1055/s-2003-41516. [DOI] [PubMed] [Google Scholar]
- 6.Kakushima N, Fujishiro M. Endoscopic submucosal dissection for gastrointestinal neoplasms. World J Gastroenterol. 2008;14:2962–2967. doi: 10.3748/wjg.14.2962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Oyama T. Counter traction makes endoscopic submucosal dissection easier. Clin Endosc. 2012;45:375–378. doi: 10.5946/ce.2012.45.4.375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lee BI. Debates on colorectal endoscopic submucosal dissection - traction for effective dissection: gravity is enough. Clin Endosc. 2013;46:467–471. doi: 10.5946/ce.2013.46.5.467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fukami N. What we want for ESD is a second hand! Traction method. Gastrointest Endosc. 2013;78:274–276. doi: 10.1016/j.gie.2013.04.192. [DOI] [PubMed] [Google Scholar]
- 10.Hirao M, Masuda K, Asanuma T, Naka H, Noda K, Matsuura K, Yamaguchi O, Ueda N. Endoscopic resection of early gastric cancer and other tumors with local injection of hypertonic saline-epinephrine. Gastrointest Endosc. 1988;34:264–269. doi: 10.1016/s0016-5107(88)71327-9. [DOI] [PubMed] [Google Scholar]
- 11.Oyama T, Kikuchi Y, Shimaya S, Tomori A, Hotta K, Miyata Y, Yamada S. Endoscopic mucosal resection using a hooking knife (hooking EMR) Stomach Intest. 2002;37:1155–1161. [Google Scholar]
- 12.Jeon WJ, You IY, Chae HB, Park SM, Youn SJ. A new technique for gastric endoscopic submucosal dissection: peroral traction-assisted endoscopic submucosal dissection. Gastrointest Endosc. 2009;69:29–33. doi: 10.1016/j.gie.2008.03.1126. [DOI] [PubMed] [Google Scholar]
- 13.Ota M, Nakamura T, Hayashi K, Ohki T, Narumiya K, Sato T, Shirai Y, Kudo K, Yamamoto M. Usefulness of clip traction in the early phase of esophageal endoscopic submucosal dissection. Dig Endosc. 2012;24:315–318. doi: 10.1111/j.1443-1661.2012.01286.x. [DOI] [PubMed] [Google Scholar]
- 14.Li CH, Chen PJ, Chu HC, Huang TY, Shih YL, Chang WK, Hsieh TY. Endoscopic submucosal dissection with the pulley method for early-stage gastric cancer (with video) Gastrointest Endosc. 2011;73:163–167. doi: 10.1016/j.gie.2010.08.041. [DOI] [PubMed] [Google Scholar]
- 15.Kondo H, Gotoda T, Ono H, Oda I, Kozu T, Fujishiro M, Saito D, Yoshida S. Percutaneous traction-assisted EMR by using an insulation-tipped electrosurgical knife for early stage gastric cancer. Gastrointest Endosc. 2004;59:284–288. doi: 10.1016/s0016-5107(03)02533-1. [DOI] [PubMed] [Google Scholar]
- 16.von Delius S, Karagianni A, von Weyhern CH, Feussner H, Schuster T, Schmid RM, Frimberger E. Percutaneously assisted endoscopic surgery using a new PEG-minitrocar for advanced endoscopic submucosal dissection (with videos) Gastrointest Endosc. 2008;68:365–369. doi: 10.1016/j.gie.2008.02.093. [DOI] [PubMed] [Google Scholar]
- 17.Chen PJ, Huang WC, Wang HP, Chang WK, Hsieh TY, Shih SC, Wang HY, Liu CY. Percutaneous transgastric traction-assisted esophageal endoscopic submucosal dissection: a randomized controlled trial in a porcine model. Scand J Gastroenterol. 2012;47:1386–1393. doi: 10.3109/00365521.2012.725091. [DOI] [PubMed] [Google Scholar]
- 18.Nishiwaki S, Araki H, Shirakami Y, Niwa Y, Iwashita M, Hatakeyama H, Saitoh K. Transgastrostomic endoscopy-assisted endoscopic submucosal dissection. Endoscopy. 2009;41 Suppl 2:E13. doi: 10.1055/s-2008-1077713. [DOI] [PubMed] [Google Scholar]
- 19.Kobayashi T, Gotohda T, Tamakawa K, Ueda H, Kakizoe T. Magnetic anchor for more effective endoscopic mucosal resection. Jpn J Clin Oncol. 2004;34:118–123. doi: 10.1093/jjco/hyh025. [DOI] [PubMed] [Google Scholar]
- 20.Gotoda T, Oda I, Tamakawa K, Ueda H, Kobayashi T, Kakizoe T. Prospective clinical trial of magnetic-anchor-guided endoscopic submucosal dissection for large early gastric cancer (with videos) Gastrointest Endosc. 2009;69:10–15. doi: 10.1016/j.gie.2008.03.1127. [DOI] [PubMed] [Google Scholar]
- 21.Imaeda H, Iwao Y, Ogata H, Ichikawa H, Mori M, Hosoe N, Masaoka T, Nakashita M, Suzuki H, Inoue N, et al. A new technique for endoscopic submucosal dissection for early gastric cancer using an external grasping forceps. Endoscopy. 2006;38:1007–1010. doi: 10.1055/s-2006-925264. [DOI] [PubMed] [Google Scholar]
- 22.Imaeda H, Hosoe N, Ida Y, Kashiwagi K, Morohoshi Y, Suganuma K, Nagakubo S, Komatsu K, Suzuki H, Saito Y, et al. Novel technique of endoscopic submucosal dissection using an external grasping forceps for superficial gastric neoplasia. Dig Endosc. 2009;21:122–127. doi: 10.1111/j.1443-1661.2009.00842.x. [DOI] [PubMed] [Google Scholar]
- 23.Parra-Blanco A, Nicolas D, Arnau MR, Gimeno-Garcia AZ, Rodrigo L, Quintero E. Gastric endoscopic submucosal dissection assisted by a new traction method: the clip-band technique. A feasibility study in a porcine model (with video) Gastrointest Endosc. 2011;74:1137–1141. doi: 10.1016/j.gie.2011.07.037. [DOI] [PubMed] [Google Scholar]
- 24.Matsumoto K, Nagahara A, Sakamoto N, Suyama M, Konuma H, Morimoto T, Sagawa E, Ueyama H, Takahashi T, Beppu K, et al. A new traction device for facilitating endoscopic submucosal dissection (ESD) for early gastric cancer: the “medical ring”. Endoscopy. 2011;43 Suppl 2 UCTN:E67–E68. doi: 10.1055/s-0030-1255923. [DOI] [PubMed] [Google Scholar]
- 25.Matsumoto K, Nagahara A, Ueyama H, Konuma H, Morimoto T, Sasaki H, Hayashi T, Shibuya T, Sakamoto N, Osada T, et al. Development and clinical usability of a new traction device “medical ring” for endoscopic submucosal dissection of early gastric cancer. Surg Endosc. 2013;27:3444–3451. doi: 10.1007/s00464-013-2887-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sakurazawa N, Kato S, Miyashita M, Kiyama T, Fujita I, Yamashita N, Saitou Y, Tajiri T, Uchida E. An innovative technique for endoscopic submucosal dissection of early gastric cancer using a new spring device. Endoscopy. 2009;41:929–933. doi: 10.1055/s-0029-1215191. [DOI] [PubMed] [Google Scholar]
- 27.Chen PJ, Chu HC, Chang WK, Hsieh TY, Chao YC. Endoscopic submucosal dissection with internal traction for early gastric cancer (with video) Gastrointest Endosc. 2008;67:128–132. doi: 10.1016/j.gie.2007.07.021. [DOI] [PubMed] [Google Scholar]
- 28.Ishigooka M, Uchizawa M, Kusama K, Takahashi b, Takagi H, Morizono R, Koyama J. Endoscopic resection with local injection of HSE solution by direct incision of submucosa for early gastric cancer (S-ERHSE). [Japanese with English abstract] Endoscopia Digestiva. 2002;11:1753–1757. [Google Scholar]
- 29.Yonezawa J, Kaise M, Sumiyama K, Goda K, Arakawa H, Tajiri H. A novel double-channel therapeutic endoscope (“R-scope”) facilitates endoscopic submucosal dissection of superficial gastric neoplasms. Endoscopy. 2006;38:1011–1015. doi: 10.1055/s-2006-944779. [DOI] [PubMed] [Google Scholar]
- 30.Neuhaus H, Costamagna G, Devière J, Fockens P, Ponchon T, Rösch T. Endoscopic submucosal dissection (ESD) of early neoplastic gastric lesions using a new double-channel endoscope (the “R-scope”) Endoscopy. 2006;38:1016–1023. doi: 10.1055/s-2006-944830. [DOI] [PubMed] [Google Scholar]
- 31.Lee SH, Gromski MA, Derevianko A, Jones DB, Pleskow DK, Sawhney M, Chuttani R, Matthes K. Efficacy of a prototype endoscope with two deflecting working channels for endoscopic submucosal dissection: a prospective, comparative, ex vivo study. Gastrointest Endosc. 2010;72:155–160. doi: 10.1016/j.gie.2010.01.056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hijikata Y, Ogasawara N, Sasaki M, Mizuno M, Masui R, Tokudome K, Iida A, Miyashita M, Funaki Y, Kasugai K. Endoscopic submucosal dissection with sheath-assisted counter traction for early gastric cancers. Dig Endosc. 2010;22:124–128. doi: 10.1111/j.1443-1661.2010.00948.x. [DOI] [PubMed] [Google Scholar]
- 33.Motohashi O, Nishimura K, Nakayama N, Takagi S, Yanagida N. Endoscopic submucosal dissection (two-point fixed ESD) for early esophageal cancer. Dig Endosc. 2009;21:176–179. doi: 10.1111/j.1443-1661.2009.00881.x. [DOI] [PubMed] [Google Scholar]
- 34.Motohashi O. Two-point fixed endoscopic submucosal dissection in rectal tumor (with video) Gastrointest Endosc. 2011;74:1132–1136. doi: 10.1016/j.gie.2011.07.035. [DOI] [PubMed] [Google Scholar]
- 35.Okamoto K, Okamura S, Muguruma N, Kitamura S, Kimura T, Imoto Y, Miyamoto H, Okahisa T, Takayama T. Endoscopic submucosal dissection for early gastric cancer using a cross-counter technique. Surg Endosc. 2012;26:3676–3681. doi: 10.1007/s00464-012-2364-7. [DOI] [PubMed] [Google Scholar]
- 36.Tsao SK, Toyonaga T, Morita Y, Fujita T, Hayakumo T, Azuma T. Modified fishing-line traction system in endoscopic submucosal dissection of large esophageal tumors. Endoscopy. 2011;43 Suppl 2 UCTN:E119. doi: 10.1055/s-0030-1256148. [DOI] [PubMed] [Google Scholar]
- 37.Ohata K, Fu K, Shouzushima M, Hamanaka J, Ono A, Ito T, Tsuji Y, Chiba H, Matsuhashi N. A novel traction system for esophageal endoscopic submucosal dissection. Endoscopy. 2012;44 Suppl 2 UCTN:E410–E411. doi: 10.1055/s-0032-1325735. [DOI] [PubMed] [Google Scholar]
- 38.Teoh AY, Chiu PW, Hon SF, Mak TW, Ng EK, Lau JY. Ex vivo comparative study using the Endolifter® as a traction device for enhancing submucosal visualization during endoscopic submucosal dissection. Surg Endosc. 2013;27:1422–1427. doi: 10.1007/s00464-012-2583-y. [DOI] [PubMed] [Google Scholar]
- 39.Morita Y, Masuda M, Tanaka S, Fujiwara M, Wakahara C, Toyonaga A new T, Azuma T. approach to treating difficult cases of early gastric cancer: development of a double scope-ESD using transnasal endoscope with a “Split Barrel” [Japanese with English abstract] Endoscopia Digestiva. 2010;22:846–852. [Google Scholar]
- 40.Higuchi K, Tanabe S, Azuma M, Sasaki T, Katada C, Ishido K, Naruke A, Mikami T, Koizumi W. Double-endoscope endoscopic submucosal dissection for the treatment of early gastric cancer accompanied by an ulcer scar (with video) Gastrointest Endosc. 2013;78:266–273. doi: 10.1016/j.gie.2013.01.010. [DOI] [PubMed] [Google Scholar]
- 41.Ahn JY, Choi KD, Choi JY, Kim MY, Lee JH, Choi KS, Kim DH, Song HJ, Lee GH, Jung HY, et al. Transnasal endoscope-assisted endoscopic submucosal dissection for gastric adenoma and early gastric cancer in the pyloric area: a case series. Endoscopy. 2011;43:233–235. doi: 10.1055/s-0030-1256037. [DOI] [PubMed] [Google Scholar]
- 42.Ho KY, Phee SJ, Shabbir A, Low SC, Huynh VA, Kencana AP, Yang K, Lomanto D, So BY, Wong YY, et al. Endoscopic submucosal dissection of gastric lesions by using a Master and Slave Transluminal Endoscopic Robot (MASTER) Gastrointest Endosc. 2010;72:593–599. doi: 10.1016/j.gie.2010.04.009. [DOI] [PubMed] [Google Scholar]
- 43.Wang Z, Phee SJ, Lomanto D, Goel R, Rebala P, Sun ZL, Trasti S, Reddy N, Wong JY, Ho KY. Endoscopic submucosal dissection of gastric lesions by using a master and slave transluminal endoscopic robot: an animal survival study. Endoscopy. 2012;44:690–694. doi: 10.1055/s-0032-1309404. [DOI] [PubMed] [Google Scholar]
- 44.Phee SJ, Reddy N, Chiu PW, Rebala P, Rao GV, Wang Z, Sun Z, Wong JY, Ho KY. Robot-assisted endoscopic submucosal dissection is effective in treating patients with early-stage gastric neoplasia. Clin Gastroenterol Hepatol. 2012;10:1117–1121. doi: 10.1016/j.cgh.2012.05.019. [DOI] [PubMed] [Google Scholar]
- 45.Saito Y, Emura F, Matsuda T, Uraoka T, Nakajima T, Ikematsu H, Gotoda T, Saito D, Fujii T. A new sinker-assisted endoscopic submucosal dissection for colorectal cancer. Gastrointest Endosc. 2005;62:297–301. doi: 10.1016/s0016-5107(05)00546-8. [DOI] [PubMed] [Google Scholar]
- 46.Imaeda H, Hosoe N, Ida Y, Nakamizo H, Kashiwagi K, Kanai T, Iwao Y, Hibi T, Ogata H. Novel technique of endoscopic submucosal dissection by using external forceps for early rectal cancer (with videos) Gastrointest Endosc. 2012;75:1253–1257. doi: 10.1016/j.gie.2012.02.018. [DOI] [PubMed] [Google Scholar]
- 47.Sakamoto N, Osada T, Shibuya T, Beppu K, Matsumoto K, Shimada Y, Konno A, Kurosawa A, Nagahara A, Ohkusa T, et al. The facilitation of a new traction device (S-O clip) assisting endoscopic submucosal dissection for superficial colorectal neoplasms. Endoscopy. 2008;40 Suppl 2:E94–E95. doi: 10.1055/s-2007-995603. [DOI] [PubMed] [Google Scholar]
- 48.Sakamoto N, Osada T, Shibuya T, Beppu K, Matsumoto K, Mori H, Kawabe M, Nagahara A, Otaka M, Ogihara T, et al. Endoscopic submucosal dissection of large colorectal tumors by using a novel spring-action S-O clip for traction (with video) Gastrointest Endosc. 2009;69:1370–1374. doi: 10.1016/j.gie.2008.12.245. [DOI] [PubMed] [Google Scholar]
- 49.Osada T, Sakamoto N, Shibuya T, Beppu K, Matsumoto K, Shimada Y, Mori H, Konno A, Kurosawa A, Nagahara A, et al. "Loops-attached rubber band" facilitation of endoscopic submucosal dissection of superficial colorectal neoplasm. Endoscopy. 2008;40 Suppl 2:E101–E102. doi: 10.1055/s-2007-995605. [DOI] [PubMed] [Google Scholar]
- 50.Tomiki Y, Ishiyama S, Sugimoto K, Takahashi M, Kojima Y, Tanaka M, Sakamoto K. Colorectal endoscopic submucosal dissection by using latex-band traction. Endoscopy. 2011;43 Suppl 2 UCTN:E250–E251. doi: 10.1055/s-0030-1256513. [DOI] [PubMed] [Google Scholar]
- 51.Okamoto K, Muguruma N, Kitamura S, Kimura T, Takayama T. Endoscopic submucosal dissection for large colorectal tumors using a cross-counter technique and a novel large-diameter balloon overtube. Dig Endosc. 2012;24 Suppl 1:96–99. doi: 10.1111/j.1443-1661.2012.01264.x. [DOI] [PubMed] [Google Scholar]
- 52.Uraoka T, Kato J, Ishikawa S, Harada K, Kuriyama M, Takemoto K, Kawahara Y, Saito Y, Okada H. Thin endoscope-assisted endoscopic submucosal dissection for large colorectal tumors (with videos) Gastrointest Endosc. 2007;66:836–839. doi: 10.1016/j.gie.2007.04.028. [DOI] [PubMed] [Google Scholar]
- 53.Uraoka T, Ishikawa S, Kato J, Higashi R, Suzuki H, Kaji E, Kuriyama M, Saito S, Akita M, Hori K, et al. Advantages of using thin endoscope-assisted endoscopic submucosal dissection technique for large colorectal tumors. Dig Endosc. 2010;22:186–191. doi: 10.1111/j.1443-1661.2010.00992.x. [DOI] [PubMed] [Google Scholar]
- 54.Fusaroli P, Grillo A, Zanarini S, Caletti G. Usefulness of a second endoscopic arm to improve therapeutic endoscopy in the lower gastrointestinal tract. Preliminary experience - a case series. Endoscopy. 2009;41:997–1000. doi: 10.1055/s-0029-1215190. [DOI] [PubMed] [Google Scholar]
- 55.Diana M, Chung H, Liu KH, Dallemagne B, Demartines N, Mutter D, Marescaux J. Endoluminal surgical triangulation: overcoming challenges of colonic endoscopic submucosal dissections using a novel flexible endoscopic surgical platform: feasibility study in a porcine model. Surg Endosc. 2013;27:4130–4135. doi: 10.1007/s00464-013-3049-6. [DOI] [PubMed] [Google Scholar]