

Abstract
Aim
To analyze the experience and knowledge of dental practitioners in Saudi Arabia regarding the identification of child abuse and neglect (CAN), to identify barriers that prevent the reporting of suspected cases of child maltreatment by dental practitioners, and to assess the need for training dentists in child protection.
Methods
A self-administered, web-based questionnaire was emailed to all of the members of the Saudi Dental Society (n = 7352) in 2012.
Results
The respondents (n = 122) demonstrated good knowledge of the forms and indicators of CAN. Moreover, a large proportion (59%) had experienced a case of child abuse or neglect in their practice over the previous five years. However, only about 10% of these respondents made a report. Fear of family reprisal, lack of certainty about the diagnosis of child maltreatment, and uncertainty about case management were critical barriers to the reporting of the suspected child maltreatment. In addition, only 20.9% of the respondents reported having knowledge of a child protection policy in their workplace.
Conclusions
Based on the results of this survey, it appears that the level of knowledge among the respondents regarding the forms and indicators of CAN is good. However, a large proportion of respondents did not take action regarding suspected cases of CAN in their practice over the past five years. Therefore, additional resources and training are needed to support the identification and management of cases of child maltreatment by dental practitioners.
Keywords: Child abuse, Child neglect, Child protection, Dental team, Saudi Arabia
1. Introduction
Child abuse and neglect (CAN) are significant problems worldwide. In particular, a substantial increase in the report of cases of CAN has occurred in Saudi Arabia, with 616 CAN cases registered in 2011 (The National Safety Program Annual Report, 2011). This is in comparison with 80 registered cases in 2010, 73 cases registered in 2009, and 65 cases registered in 2008 (The National Safety Program Annual Report, 2010). Although these numbers only represent hospital-based reported cases of CAN, these statistics do reflect an increased awareness among physicians regarding CAN cases. Furthermore, there is a legal obligation for health care providers in Saudi Arabia to report suspected cases of CAN.
CAN has been defined by the World Health Organization as, “Every kind of physical, sexual, emotional abuse, neglect or negligent treatment, commercial or other exploitation resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power” (World Health Organization, 1999). Thus, this definition includes both considerations of action (physical, emotional, or sexual abuse) and omission (neglect). The potential for irreversible damage to a child developmentally, mentally, and/or physically, depends on both the extent of the abuse and the age of the child.
Based on the regular contact that dental practitioners have with children and their families, these health professionals are in a favorable position to observe abnormal child–parent behavior, and to identify and report suspected cases of CAN (Jessee, 1999). It is also possible to diagnose child dental neglect, as well as neglect in general, upon dental examination. In 1992, Da Fonseca et al. reported that “abusive caretakers rarely take the child to the same physician, but they are not cautious about dentists”. This observation further supports the importance of dental evaluations and the awareness of dental practitioners regarding CAN.
It has been reported that the physical abuse of children manifests in the oro-facial region in 50–77% of abuse cases (Hibbard and Sanders, 2004), and this is an area that dentists routinely assess. However, despite the opportunities to detect child maltreatment, dentists are reluctant to report CAN due to lack of certainty about the diagnosis of abuse, lack of knowledge about the referral procedures for cases of CAN, fear of negative effects on the child or the child’s family, and concerns about confidentiality (Al-Habsi et al., 2009; Cairns et al., 2005; Harris et al., 2009a,b; John et al., 1999; Manea et al., 2007; Owais et al., 2009; Welbury et al., 2003; Uldum et al., 2010). Similar results have been published for dentists in Jordan (Sonbol et al., 2011; Owais et al., 2009). However, to our knowledge, there are no published data available regarding dentists’ perception of their role in detecting and reporting suspected cases of CAN in Saudi Arabia, nor are there any studies published on the knowledge of dentists in Saudi Arabia regarding the signs, symptoms, and risk factors of CAN.
Therefore, the purpose of this study was to analyze the experience and knowledge reported by dental practitioners in Saudi Arabia regarding the identification of CAN, to identify dental practitioners’ attitudes toward reporting CAN, to identify the barriers that prevent the reporting of suspected cases of child maltreatment, and to assess the need for additional training in child protection.
2. Materials and methods
This study was conducted at King’s College London. Therefore, ethical approval was obtained for this study from the Biomedical Sciences, Dentistry, Medicine, and Natural & Mathematical Sciences Research Ethics Subcommittee (BDM) of King’s College London Research Ethics Committee.
A web-based questionnaire was distributed via email to all dentists registered with the Saudi Dental Society in February 2012. A cover letter, a link to the survey platform (SurveyMonkey©), and an information sheet were enclosed in the email which stated that responses would be anonymous and confidential. Participants were given six weeks to complete the survey. To maximize response rates, two reminder emails were sent two weeks and four weeks after the initial distribution of the questionnaire. The reminders were sent to all of the members of the Saudi Dental Society and they included a link to the survey as suggested by Dillman (2007) and Edwards et al. (2007). General dentists and dental practitioners from all specialties were included in this study. However, dentists with less than one year of experience were excluded. While the intent was to maximize the representativeness of the sample, the results analyzed are only those from the dentists that responded. Moreover, there are no published data on the demographic characteristics of dental practitioners in Saudi Arabia to compare the current data.
2.1. The questionnaire
The questionnaire was written in the English language based on previous similar studies (Ramos-Gomez et al., 1998; John et al., 1999; Kilpatrick et al., 1999; Cairns et al., 2005; Thomas et al., 2006; Al-Habsi et al., 2009; Chadwick et al., 2009; Harris et al., 2009a,b). The questionnaire was reviewed by two psychologists with knowledge of this field. The content validity of the questionnaire was tested by conducting a pilot survey of postgraduate students studying at the Dental Institute, King’s College London (n = 30). Unfortunately, it was not practically possible to conduct the pilot study with the target population, since the researchers were located in the United Kingdom. However, the pilot sample did include students of Saudi origin that were studying in the United Kingdom. The postgraduate students were asked to comment on the comprehensiveness of the material covered by the questionnaire (e.g., did the measures reflect all aspects of CAN), to indicate which aspects of CAN were not covered, and to address the clarity of the question and response formats. The criterion-related validity of the questionnaire could not be tested since standard measures of the constructs that were measured are not currently available. Some comments and modifications that were received were incorporated into the final version of the questionnaire.
The questionnaire was composed of five sections:
The first section included ten questions that were designed to survey the characteristics and demographics of the respondents, including age, gender, nationality, professional experience, education, specialty, place of work, and the number of children seen per week.
The second section consisted of questions designed to survey the respondents’ ability to recognize different forms of CAN (the seven items surveyed were all considered to represent forms of abuse, except for ‘non-injurious spanking’), risk factors for CAN (13 items), manifestations of physical abuse (6 items), and indicators of CAN (9 items which are likely to be indicators of CAN, except for bruises on a toddler’s forehead).
The third section of the questionnaire consisted of six questions that were designed to address the respondents’ professional experience with CAN, the number of children with neglected dentition that had been evaluated in their practice, the history of suspected child abuse cases for their practice, actions taken for suspected cases, the number of suspected CAN cases observed in the last five years, and whether their practice has a protocol in place for dealing with CAN in the workplace.
The fourth section mainly included questions regarding barriers that potentially interfere with the reporting of suspected cases of CAN (11 items).
Lastly, the fifth section was composed of five questions that addressed the history of training in child protection by the respondents, as well as the opinion of the respondents regarding the need for continuing education in recognizing and reporting CAN.
The response formats for these sections included yes/no answers, multiple choice answers, or the selection of a response according to a five-point Likert scale. The latter was scored from 1 to 5 to represent answers of “strongly disagree”, “disagree”, “neutral”, “agree”, and “strongly agree”, respectively. The Likert scale is considered reliable in providing an approximate ordering of respondents’ concerns regarding a specific attitude (Oppenheim, 1992).
Data received were coded and analyzed using the Statistical Package for Social Sciences (IBM SPSS) version 20 software.
3. Results
3.1. Demographic characteristics of the respondents
A total of 163 Saudi dentists responded to the web-based survey that was distributed to all dentists registered with the Saudi Dental Society. However, 41 dentists only completed the demographic section of the questionnaire, and therefore, their incomplete questionnaires were excluded from the study. For the remaining 122 participants, the male-to-female ratio was 1:1, consisting of 61 dentists of each gender. A total of 90/122 (73.8%) dentists were ⩽40 years of age, while 32/122 (26.2%) were >40 years of age. Regarding experience, 108/122 (88.5%) respondents reported practicing dentistry for less than 20 years, while 14/122 (11.5%) had more than 20 years of experience. Most of the respondents worked in a university setting (41%), while the remainder were employed in private or public hospitals and clinics. The academic degrees and specialties of the respondents are summarized in Table 1.
Table 1.
Academic degrees and specialties of the respondents.
| Topic surveyed | Answer | Responses N (%) |
|---|---|---|
| Last degree obtained | Bachelor’s degree | 57 (46.7) |
| Master’s degree | 36 (29.5) | |
| PhD degree | 11 (9.0) | |
| Fellowship | 1 (0.8) | |
| Board member | 16 (13.1) | |
| Other | 1 (0.8) | |
| Specialty | General dentistry | 49 (40.2) |
| AGD⁎ | 2 (1.2) | |
| Restorative dentistry | 11 (9.0) | |
| Pediatric dentistry | 16 (13.1) | |
| Orthodontics | 8 (6.6) | |
| Periodontics | 7 (5.7) | |
| Maxillofacial surgery | 3 (2.5) | |
| Prosthodontics | 9 (7.4) | |
| Endodontics | 14 (11.5) | |
| Oral medicine | – | |
| Dental Public Health | 3 (2.5) | |
Advanced general dentistry.
3.2. Knowledge of CAN
Dentists were asked to identify different forms of CAN by agreeing or disagreeing with statements that represented different forms of abuse. Nine out of ten items represented abuse, with the exception being ‘non-injurious spanking’. The average total score for the respondents when the latter was excluded was 84.2%. Fig. 1 shows the distribution of responses according to each item.
Figure 1.
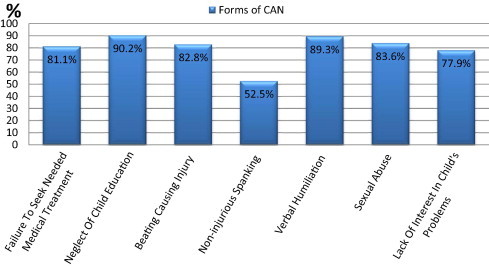
Proportion of agreement among respondents regarding proposed forms of CAN.
When asked about risk factors of CAN, the responses varied among the respondents. Fig. 2 presents the proportion of dentists who correctly identified risk factors associated with CAN.
Figure 2.
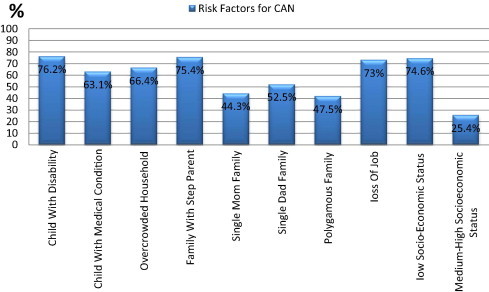
Proportion of respondents who correctly identified risk factors for CAN.
3.3. Observed indicators of CAN
When asked about the most common manifestations of physical abuse, the total average score of the respondents was 73.3%. The highest percentage of respondents (86.1%) indicated that skin and mucosal burns were the most common manifestations, followed by oro-facial injuries (84.4%). In addition, 69.7% of respondents indicated that bruises on the neck were manifestations of physical abuse, while 63.1% agreed ‘injuries to soles of feet’ and ‘bone fracture’ represented manifestations of physical abuse.
For a high percentage of respondents (81.1%), bruises on the soft tissue of the cheeks represented an indicator of CAN, while only 52.5% of respondents indicated that intra oral injuries were a common indicator of CAN. Furthermore, regarding ‘bruises on a toddler’s forehead’, 67.2% agreed this represented an indicator of CAN. Fig. 3 shows the proportion of dentists who identified various indicators as those of CAN.
Figure 3.
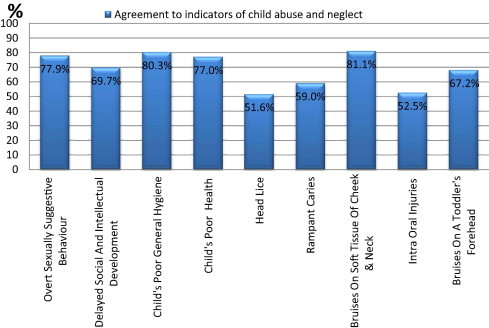
Proportion of respondents who correctly identified indicators of CAN.
3.4. Experience with suspected cases of CAN
Of the respondents, 16.4% did not treat children. Therefore, of those who routinely treated children, 27.0% reported observing at least one case a day of neglected dentition in their practice. The experience of respondents with children exhibiting neglected dentition is summarized in Table 2.
Table 2.
Experience of respondents with children exhibiting neglected dentition.
| Topic surveyed | Answer | Responses total = 122) N (%) |
|---|---|---|
| Approximately how often do you see children with neglected dentition? | Children are not evaluated | 20 (16.4) |
| No cases observed | 32 (26.2) | |
| One case a day | 11 (9.0) | |
| More than one case a day | 22 (18.0) | |
| One case a week | 10 (8.2) | |
| One case a month | 14 (11.5) | |
| One case every 6 months | 12 (9.8) | |
| One case a year | – |
A total of 72/122 (59%) respondents reported evaluating a child suspected of being subjected to CAN in the last five years. Table 3 describes the types of child abuse suspected by dentists in these cases. However, while 84.3% of all respondents reported their willingness to report a suspected case of child abuse, 19.7% of the dentists with CAN cases in their practice did not take any action. Moreover, 39.4% only documented the signs of abuse in the patient’s medical record. A very small percentage of dentists (7.0%) contacted social services, and contact of police was least popular among the respondents, with only 2.82% reporting this action (Table 4). In addition, only 20.9% of the respondents reported knowledge of a child protection policy in their workplace.
Table 3.
Frequencies of the type of CAN cases suspected by respondents in the last five years.
| Type of abuse | Answer | KSA Sample (n = 122) N (%) |
|---|---|---|
| (1) Physical abuse | Up to 5 | 47 (38.5) |
| >5 | 14 (8.3) | |
| (2) Emotional abuse | Up to 5 | 39 (32) |
| >5 | 24 (19.7) | |
| (3) Sexual abuse | Up to 5 | 30 (24.6) |
| >5 | 0 | |
| (4) Neglect | Up to 5 | 19 (15.6) |
| >5 | 44 (36.1) |
Table 4.
Actions taken by respondents with suspected cases of CAN in their practice (n = 71).
| Actions taken regarding CAN cases | Answers reported |
|
|---|---|---|
| N | % | |
| (1) Dismissed/no action taken | 14 | 19.72 |
| (2) Documented signs of abuse in patient’s records | 28 | 39.40 |
| (3) Discussed the case with the child’s caregiver | 32 | 45.07 |
| (4) Discussed the case with a senior staff member | 29 | 40.85 |
| (5) Discussed the case with a colleague | 32 | 45.07 |
| (6) Contacted social services | 5 | 7.04 |
| (7) Contacted police | 2 | 2.82 |
Percentages add up to more than 100 because participants could indicate more than one response.
Dentists were able to give more than one response to the question inquiring about whom to discuss or refer concern in cases of suspicion of CAN. The majority of dentists (62.6%) reported that they preferred to discuss suspected cases of CAN with a social worker. In addition, 31.3% preferred to discuss suspected cases with the caregiver, 55.7% preferred to discuss the case with a senior staff member, 38.3% preferred to consult a colleague, and 22.6% preferred to discuss suspected cases with the police.
3.5. Barriers to reporting suspected cases of CAN
In general, fear of family violence toward the child was reported as the main barrier (88%) preventing the respondents from reporting suspected cases of CAN. In addition, respondents reported lack of certainty about the diagnosis of CAN (80%) and lack of knowledge in referral procedures of CAN (79%) as barriers to reporting suspected abuse cases (Fig. 4).
Figure 4.
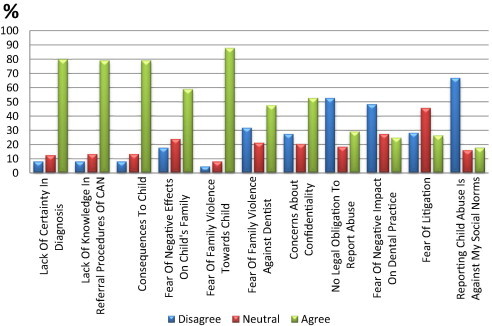
Barriers to reporting suspected cases of CAN perceived by respondents.
3.6. Present knowledge and attitudes toward training programs for child protection
Only four dentists reported attending a training program in child protection (3.3%), although the majority of respondents (94.7%) agreed that dentists’ knowledge of child protection protocols is important. Similarly, 93% of respondents agreed that additional training is required in this field. However, 47.8% of respondents reported being confident in recognizing signs of CAN’. Further details regarding their responses are provided in Table 5.
Table 5.
Knowledge of and attitudes toward training programs of child protection by respondents.
| Statement for consideration | Answer | Responses (total n = 113) |
|---|---|---|
| N (%) | ||
| (1) Knowledge about child protection protocols is important | D | 1 (0.9) |
| N | 5 (4.4) | |
| A | 107 (94.7) | |
| (2) More training regarding child protection is needed for dentists in this field | D | 1 (0.9) |
| N | 7 (6.2) | |
| A | 105 (92.9) | |
| (3) I can confidently recognize signs of child abuse | D | 25 (22.1) |
| N | 34 (30.1) | |
| A | 54 (47.8) | |
| Number of missing data | 9 | |
D: Disagree, N: Neutral, A: Agree.
4. Discussion
While the limitations of this study include the low response rate and a sample consisting mainly of academics rather than practitioners, the results provide valuable insights into a very important issue and significantly contribute to our knowledge of the attitudes and experience regarding CAN by health professionals in the dental field in Saudi Arabia.
4.1. Knowledge of the different forms of CAN
To our knowledge, this cross-sectional study to identify the knowledge and attitudes of dental practitioners in Saudi Arabia toward CAN is the first to be conducted in Saudi Arabia. However, comparable studies have previously been published for dentists in the United Arab Emirates (Hashim and Al-Ani, 2013) and Jordan (Owais et al., 2009; Sonbol et al., 2011).
In the present study, a score of 80% was set as the cut-off between adequate knowledge and deficient knowledge (Habib, 2012). Most of the respondents for this survey were found to have adequate knowledge of different forms of CAN, which included physical, emotional, and sexual abuse, as well as neglect, in the questionnaire distributed. The average score was 84.2%, when ‘non-injurious spanking’ was excluded, and similar results were published by Habib (2012) in a study involving the knowledge of pediatricians in Saudi Arabia regarding CAN. In a study of dentists in Jordan, 97% of both general dental practitioners (GDPs) and specialists were able to identify physical abuse, 92% identified sexual abuse, and 84% identified emotional abuse and neglect as forms of child maltreatment (Owais et al., 2009).
Interestingly, 52.5% of the current respondents reported that non-injurious spanking (corporal punishment) was also a form of CAN. This result is surprisingly high given that a 2012 report of the Global Initiative to End All Corporal Punishment of Children in Saudi Arabia revealed that corporal punishment was still lawful in the home. Furthermore, Basic Laws (1992) that prevent abuse are not interpreted as prohibiting corporal punishment as part of childcare. The present finding may be explained by the high percentage of respondents who held faculty positions at a university (41%), and thus may have greater exposure to the literature on child protection. In addition, 13% of the respondents were pediatric dentists, and this subset of respondents might also have increased exposure to the literature on child abuse.
4.2. Knowledge of CAN risk factors
Knowledge of the factors that increase the risk of CAN was found to be deficient based on the questionnaires returned. This result emphasizes the need for a better understanding of the causative factors that can increase the risk of CAN. These topics could be incorporated into a training program for dentists in Saudi Arabia. Moreover, such information is vital for dentists to have a comprehensive understanding of the various aspects of child protection and to be better able to detect suspected cases of CAN. In a study conducted in Jordan, more than half of the dentists surveyed (57%) reported that CAN occurred mostly in low socio-economic households, rather than in middle or high socio-economic classes (Sonbol et al., 2011). Correspondingly, 74.6% of the current respondents conveyed that CAN was more common in low socio-economic classes, and 28% disagreed with the statement that CAN occurs in medium to high socio-economic classes. In addition, Hobbs and Wynne (2001) previously reported that low socio-economic status, poverty, and temporary housing are highly and consistently linked to the incidence of CAN. In another study (Gillham et al., 1998), a link between parent unemployment and the risk of child maltreatment was identified. Despite these findings, however, it is important for healthcare providers to recognize that child maltreatment is not confined to poverty and low socio-economic classes.
4.3. Common manifestations of physical abuse
The respondents for the present study exhibited deficient knowledge regarding common manifestations of physical abuse. Moreover, similar results have been reported in previous studies (Owais et al., 2009; Sonbol et al., 2011; Hashim and Al-Ani 2013). Taken together, these results indicate that a need still exists for training of health professionals in child protection.
4.4. Observed indicators of CAN
Regarding observed indicators of child abuse, most of the respondents (81%) indicated that bruises on the soft tissue of the cheek and neck were indicators of child abuse. Similar findings were reported by Owais et al. (2009) for dentists in Jordan. For bruises on a toddler’s forehead, 68% of respondents considered this an indicator of abuse. Similarly, a study of United Arab Emirates dental students by Hashim and Al-Ani (2013) reported that 79.2% of the students agreed that physical abuse usually occurs in areas overlying bony prominences. Although, it is important to consider that toddlers are known to be more prone to accidental falls in their first years of walking that are likely to lead to injuries over bony prominences. Distinguishing between these two possibilities is likely to be part of a child protection training program.
4.5. Experience with suspected CAN
The proportion of respondents who had suspected their patients represented cases of abuse in the last five years is higher (59%) than previously reported (Ramos-Gomez et al., 1998; Cairns et al., 2005; Manea et al., 2007). This may be due to the large percentage of respondents in the present study that possessed advanced degrees, in combination with the large number of pediatric dentistry specialists who responded and would be predicted to evaluate a greater number of children. Owais et al. (2009) reported a high percentage (42%) of dentists in Jordan who suspected CAN cases, and Sonbol et al. (2011) reported a percentage of 50%. In contrast, Al-Buhairan et al. (2011) reported that only 20% of school professionals in Saudi Arabia had encountered at least one case of child maltreatment throughout their career. Al-Buhairan et al. (2011) also reported that only 22% of the dentists evaluated were aware of the United Nations Convention of the Rights of the Child (UNCRC) Article 19, or national policies addressing child maltreatment (United Nations Human Rights. Convention on the Rights of the Child, 1989). Thus, the lower percentage of encountered CAN cases may not represent the actual incidence of CAN but rather undiagnosed cases of child maltreatment.
Child dental neglect is perceived to be within the scope of child neglect and thus should be addressed seriously. In the present study, around one quarter of respondents reported seeing at least one case of dental neglect per day. This may be due to inadequate dental care and diet by the caregiver, or inaccessibility of dental care to these families. Since many families face difficulties in accessing dental care, clinicians need to determine whether dental services are available to the family when considering dental neglect. Dental neglect is considered a form of CAN when a caregiver is aware of a child’s need for dental care but willfully denies the child from dental care (American Academy of Pediatrics Committee on Child Abuse and Neglect and the American Academy of Pediatric Dentistry, 2010).
4.6. Action taken regarding incidences of suspected CAN
The results of the present study indicate that a gap exists between suspected cases of CAN (59%) and the reporting of suspected incidences. For example, almost one in every five respondents did not take action after suspecting a CAN case. Moreover, only 39.4% of the respondents indicated that they had recorded suspected findings in the affected child’s medical record. Good record keeping is essential in dentistry for legal purposes, and especially if CAN is suspected. Correspondingly, a comprehensive record should include injuries observed by the dentist along with any other significant findings, including any abnormal child-caregiver interactions (Cairns et al., 2005). To obtain evidence for child protection procedures, X-rays and photographic evidence should be obtained with consent from the caregiver. A special form for recording findings related to suspected cases of CAN should also be available in dental clinics. Accordingly, dental practitioners should be trained in the handling of such cases and in the completing of these forms.
It was not surprising to find that almost half of the dentists who indicated they had experience with suspected CAN cases discussed these situations with a colleague. Colleagues are generally readily accessible, and it is understandable that a dentist would feel more comfortable discussing such a sensitive matter within his professional circle. Alternatively, 62.6% of respondents preferred to discuss CAN cases with a social worker. However, only 7% of these reported actually contacting a social worker. This may be due to a lack of communication that typically exists between dental practitioners and social workers. Moreover, contact of the police was the least often reported action taken. Similar findings have also been reported in other studies. For example, Owais et al. (2009) reported that only 20% of the dentists they surveyed reported suspected cases of CAN, while Sonbol et al. (2011) reported that only 12% of their cohort reported cases of CAN.
4.7. Barriers to reporting suspected cases of CAN
Under-reporting of CAN cases by dentists and healthcare providers is a problem that challenges many societies. The main barrier to reporting suspected CAN cases in the present study was fear of violence toward the child (87.7%). Similarly, 66% of GDPs in a study by Al-Habsi et al. (2009) reported fear of an unknown consequence to the child as a barrier (79%). Since corporal punishment is still acceptable culturally and under the law in Saudi Arabia, this supports the reported fear of dentists regarding a child’s well-being. Lack of confidence in child protection services and their ability to handle such sensitive cases has also been identified as a potential barrier for the reporting of CAN cases (John et al., 1999).
‘Lack of certainty about the diagnosis’ was the second most common barrier reported by respondents of the present study (79.8%). Similarly, this was the most cited barrier to referral in studies by Harris et al. (2009a,b) and Cairns et al. (2005). Interestingly, dental practitioners are not required to diagnose a case before making a referral; diagnosis is the shared responsibility of the child protection team Harris et al. (2009a,b). In Saudi Arabia, child protection teams consist of a pediatric physician, a psychologist, and a social worker (Almuneef and Al-Eissa, 2011). In the present study, lack of knowledge of referral procedures was also reported as a barrier to reporting suspected CAN cases (78.9%), and only 21% of respondents reported knowledge of an existing child protection protocol in their workplace. Uncertainty about referral procedures was also reported by Sonbol et al. (2011) as a major concern that prevented dentists from reporting suspected cases of CAN in Jordan. However, health care professionals are responsible for reporting and preventing child maltreatment, and they must seek the necessary knowledge in reporting procedures if needed. In Saudi Arabia and Jordan, a lack of child protection training programs contributes to this situation.
Fear of negative effects on the child’s family was reported by 58.8% of respondents as a barrier to the reporting of suspected CAN cases. Similarly, almost half of the dentists surveyed in this study reported ‘family violence against dentists’ as a barrier. In contrast, Sonbol et al. (2011) reported that only a quarter of the dentists they surveyed expressed fear from the affected family or anger of the parents. Another concern expressed in the current study was regarding confidentiality associated with reporting CAN cases. A similar concern was reported in a study by Owais et al. (2009). Unfortunately, approximately half of the current respondents disagreed with the statement that ‘dentists have no legal obligation to report abuse’. This percentage is surprisingly high, considering that a large percentage of the respondents reported holding university faculty positions, postgraduate degrees, and pediatric dentistry as a specialty. Therefore, it is possible that the dental practitioners in Saudi Arabia may include an even larger percentage of dentists who feel they have no obligation toward child protection. Conversely, the least reported barriers to the reporting of CAN cases included: fears of a negative impact on dental practice, fear of litigation, and reporting child abuse is against social norms.
4.8. Child protection training
The majority of respondents had not attended any type of formal training in child protection, and 92.9% agreed that such training is required for dentists. Similar findings were reported by Al-Buhairan et al. (2011) with only 1.9% of school professionals surveyed having attended any sort of training in child protection. However, in the latter study, 69.3% of those surveyed were willing to attend training.
Unfortunately, inadequate training in child protection is evident in this study, and was evident from pediatricians in Saudi Arabia surveyed by Habib (2012) as well. By publishing these results, it is hoped that child protection will be better recognized and appreciated by health care providers. Furthermore, these results indicate that there is a need for clear guidelines, regulations, and training related to child protection. Good communication is also needed between health care providers and local authorities, child protection teams, and pediatricians in order to establish protocols to deal with CAN cases.
5. Limitations
This study was associated with several limitations. First, the questionnaire was initially completed by postgraduate dental students studying at King’s College London, rather than a Saudi population. However, the goal of the pilot testing was to focus on the comprehensiveness and comprehensibility of the material covered by the questionnaire.
Secondly, the total number of participants in this study was 122, despite distribution of the questionnaire and reminders to all dentists registered with the Saudi Dental Society. It is possible that this email-based contact may have been labeled as “SPAM” or “junk email”, thus lowering the possibility that the recipients actually received the intended emails. In addition, the low rate of return could also be attributed to changes in the e-mail addresses of dentists registered with the Saudi Dental Society, as well as the lack of interest or knowledge in the subject. The questionnaire was also long and this may have discouraged dental practitioners from completing it (Edwards et al., 2007). However, the survey was designed to be comprehensive, and similar studies included comparable sample sizes (Kilpatrick et al., 1999; Manea et al., 2007; Al-Habsi et al., 2009; Habib, 2012).
Thirdly, a large percentage of respondents in this study were academics. Therefore, the results obtained are not necessarily representative of the total population of dentists working in Saudi Arabia. However, to our knowledge, there are also no published data regarding the demographic characteristics of dentists living in Saudi Arabia, thereby preventing an analysis of the demographics that characterized the present study. Moreover, knowledge of child protection that is reported in the present study may not represent the actual knowledge of dental practitioners working in Saudi Arabia, and thus, knowledge of CAN may be even lower than what has been reported.
Conflict of interest
The authors have no conflicts of interest to declare.
Footnotes
Peer review under responsibility of King Saud University.

Contributor Information
R. Al-Dabaan, Email: rasha.al-dabaan@kcl.ac.uk.
J.T. Newton, Email: tim.newton@kcl.ac.uk.
K. Asimakopoulou, Email: koula.asimakopoulou@kcl.ac.uk.
References
- Al-Buhairan F.S., Inam S.S., AlEissa M.A., Noor I.K., Almuneef M.A. Self- reported awareness of child maltreatment among school professionals in Saudi Arabia: Impact of CRC ratification. Child Abuse Negl. 2011;35(1):1032–1036. doi: 10.1016/j.chiabu.2011.10.002. [DOI] [PubMed] [Google Scholar]
- Al-Habsi S.A., Roberts G.J., Attari N., Parekh S. A survey of attitudes, knowledge and practice of dentists in London towards child protection. Are children receiving dental treatment at the Eastman Dental Hospital likely to be on the child protection register? Br. Dent. J. 2009;206(4):E7. doi: 10.1038/sj.bdj.2009.113. [DOI] [PubMed] [Google Scholar]
- Almuneef M., Al-Eissa M. Preventing child abuse and neglect in Saudi Arabia: are we ready? Ann. Saudi Med. 2011;31(6):635–640. doi: 10.4103/0256-4947.87102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Academy of Pediatrics Committee on Child Abuse and Neglect and the American Academy of Pediatric Dentistry, 2010. Guideline on Oral and Dental Aspects of Child Abuse and Neglect. Available at: <http://www.aapd.org/media/Policies_Guidelines/G_Childabuse.pdf> (accessed 25.03.13). [PubMed]
- Cairns A.M., Mok J.Y.Q., Welbury R.R. The dental practitioner and child protection in Scotland. Br. Dent. J. 2005;199(8):517–520. doi: 10.1038/sj.bdj.4812809. [DOI] [PubMed] [Google Scholar]
- Chadwick B.L., Davies J., Bhatia S.K., Rooney C., McCusker N. Child protection: training and experiences of dental therapists. Br. Dent. J. 2009;6(3):18–21. doi: 10.1038/sj.bdj.2009.666. [DOI] [PubMed] [Google Scholar]
- Da Fonseca M.A., Feigal R.J., Ten Bensel R.W. Dental aspects of 1248 cases of child maltreatment on file at a major county hospital. Pediatr. Dent. 1992;14(3):152–157. [PubMed] [Google Scholar]
- Dillman D.A. second ed. John Wiley & Sons Inc; Hoboken, NJ: 2007. Mail and Internet Surveys: The Tailored Design Method. [Google Scholar]
- Edwards P., Roberts I., Clarke M., DiGuiseppi C., Pratap S., Wentz R., Kwan I. The Cochrane Library; 2007. (Methods to influence response to postal questionnaires). [DOI] [PubMed] [Google Scholar]
- Gillham B., Tanner G., Cheyne B., Freeman I., Rooney M., Lambie A. Unemployment rates, single parent density, and indices of child poverty: their relationship to different categories of child abuse and neglect. Child Abuse Negl. 1998;22(2):79–90. doi: 10.1016/s0145-2134(97)00134-8. [DOI] [PubMed] [Google Scholar]
- Global Initiative to End All Corporal Punishment of Children, report on Saudi Arabia, 2012. Available at: <http://www.endcorporalpunishment.org/pages/pdfs/states-reports/Saudi%20Arabia.pdf> (accessed 15.02.13).
- Habib H.S. Pediatrician knowledge, perception, and experience on child abuse and neglect in Saudi Arabia. Ann. Saudi Med. J. 2012;32(3):236–242. doi: 10.5144/0256-4947.2012.236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris J.C., Elcock C., Sidebotham P.D., Welbury R.R. Safeguarding children in dentistry: 1. Child protection training, experience and practice of dental professionals with an interest in paediatric dentistry. Br. Dent. J. 2009;206(8):409–414. doi: 10.1038/sj.bdj.2009.307. [DOI] [PubMed] [Google Scholar]
- Harris J.C., Elcock C., Sidebotham P.D., Welbury R.R. Safeguarding children in dentistry: 2. Do paediatric dentists neglect child dental neglect? Br. Dent. J. 2009;206(9):465–470. doi: 10.1038/sj.bdj.2009.356. [DOI] [PubMed] [Google Scholar]
- Hashim R., Al-Ani A. Child physical abuse: assessment of dental students’ attitudes and knowledge in United Arab Emirates. Eur. Arch. Paediatr. Dent. 2013;14:301–305. doi: 10.1007/s40368-013-0063-2. [DOI] [PubMed] [Google Scholar]
- Hibbard R.A., Sanders B.J. Child abuse and neglect. In: McDonalds R.E., Avery D.R., Dean J.A., editors. Dentistry for the Child and Adolescent. eigth ed. Mosby Inc; St Louis, Missouri: 2004. pp. 23–32. [Google Scholar]
- Hobbs C.J., Wynne J.M. second ed. Harcourt Publishers Ltd; London: 2001. Physical Signs of Child Abuse: A Colour Atlas. [Google Scholar]
- Jessee S.A. Child abuse and neglect: implications for the dental profession. Tex. Dent. J. 1999;116(1):40–46. [PubMed] [Google Scholar]
- John V., Messer L.B., Arora R., Fung S., Hatzis E., Nguyen T. Child abuse and dentistry: A study of knowledge and attitudes among dentists in Victoria, Australia. Aust. Dent. J. 1999;44(4):259–267. doi: 10.1111/j.1834-7819.1999.tb00230.x. [DOI] [PubMed] [Google Scholar]
- Kilpatrick N.M., Scott J., Robinson S. Child protection: a survey of experience and knowledge within the dental profession of New South Wales, Australia. Int. J. Paediatr. Dent. 1999;9(3):153–159. doi: 10.1046/j.1365-263x.1999.00130.x. [DOI] [PubMed] [Google Scholar]
- Manea S., Favero G.A., Stellini E., Romoli L., Mazzucato M., Facchin P. Dentists’ perceptions, attitudes, knowledge, and experience about child abuse and neglect in Northeast Italy. J. Clin. Pediatr. Dent. 2007;32(1):19–26. doi: 10.17796/jcpd.32.1.f920721252jx3614. [DOI] [PubMed] [Google Scholar]
- Oppenheim A.N. Continuum; New York: 1992. Questionnaire Design, Interviewing and Attitude Measurement. [Google Scholar]
- Owais A.I.N., Qudeimat M.A., Qodceih S. Dentists’ involvement in identification and reporting of child physical abuse: Jordan as a case study. Int. J. Pediatr. Dent. 2009;19(4):291–296. doi: 10.1111/j.1365-263X.2009.00971.x. [DOI] [PubMed] [Google Scholar]
- Ramos-Gomez F., Rothman D., Blain S. Knowledge and attitudes among California dental care providers regarding child abuse and neglect. J. Am. Dent. Assoc. 1998;129(3):340–348. doi: 10.14219/jada.archive.1998.0208. [DOI] [PubMed] [Google Scholar]
- Sonbol H.N., Abu-Ghazaleh S., Rajab L.D., Baqain Z.H., Saman R., Al-Bitar Z.B. Knowledge, educational experiences and attitudes towards child abuse amongst Jordanian dentists. Eur. J. Dent. Educ. 2011;16(1):158–165. doi: 10.1111/j.1600-0579.2011.00691.x. [DOI] [PubMed] [Google Scholar]
- The Saudi National Safety Program Annual Report, 2010.
- The Saudi National Safety Program Annual Report, 2011.
- Thomas J.E., Straffon L., Inglehart M.R. Child abuse and neglect: dental and dental hygiene students’ educational experiences and knowledge. J. Dent. Educ. 2006;70(5):558–565. [PubMed] [Google Scholar]
- Uldum B., Christensen H.N., Welbury R., Poulsen S. Danish dentists’ and dental hygienists’ knowledge of and experience with suspicion of child abuse or neglect. Int. J. Pediatr. Dent. 2010;20(5):361–365. doi: 10.1111/j.1365-263X.2010.01070.x. [DOI] [PubMed] [Google Scholar]
- United Nations Human Rights. Convention on the Rights of the Child, 1989. <http://www.ohchr.org/en/professionalinterest/pages/crc.aspx>.
- Welbury R.R., MacCaskill S.G., Murphy J.M., Evans D.J., Weightman K.E., Jackson M.C. General dental practitioners’ perception of their role within child protection: a qualitative study. Eur. J. Paediatr. Dent. 2003;4(1):89–95. [PubMed] [Google Scholar]
- World Health Organization . WHO; Geneva: 1999. Report of the Consultation on Child Abuse Prevention. [Google Scholar]