

Abstract
Background:
Halitosis or oral malodor is characterized by unpleasant odor arising from the oral cavity. The prevalence of halitosis however is not studied extensively. The aim of this study was to evaluate the self perception of oral malodor and oral hygiene habits amongst dental students.
Materials and Methods:
A structured questionnaire consisting of ten questions was administered to 285 undergraduate students of Madha Dental College and Hospital. The questionnaire was designed to evaluate the self perception of halitosis, oral hygiene aids used, presence of dental caries, gingival bleeding, and dryness of mouth.
Results:
Of the 285 students, 259 students completed the questionnaire. The response rate was 90%, with male response rate being 85.7% and female 95.8%. Self-perceived halitosis was reported by 44.1% males and 45.32% females. The difference in reporting self-perception of halitosis between females and males was found to be statistically significant (P < 0.05). Significant difference was found for use of mouth wash, presence of carious teeth, bleeding gums, and use of tongue cleaners between females and males (P < 0.05).
Conclusion:
The results of this study indicate higher prevalence of halitosis among this population consisting of dental students. The awareness of halitosis was also higher among this population. The awareness of halitosis as an individual entity should be promoted to the general population and the therapeutic measures should be made available to all.
Keywords: Dental students, halitosis, oral hygiene, oral malodor
INTRODUCTION
Unpleasant odor emitted from a person's oral cavity is referred to as halitosis. The other common terminologies that are used to denote halitosis are fetor oris, oral malodor, or bad breath. Halitosis is an oral health condition characterized by consistently emanating odorous breath and may be caused by several agents including poor oral hygiene, improper cleaning of dentures, decreased salivary flow rate, use of tobacco in any form, or certain systemic conditions.[1] Its etiology could be attributed to both intraoral or extraoral factors. However, in about 90% of the cases, the cause is intra oral, with the reason being deep carious lesions, periodontal disease, peri-implant disease, mucosal ulcers, food debris, reduced salivary flow rates, or tongue coating.[2] Among the listed intra oral causes for halitosis, tongue coating is the most common reason in otherwise healthy individuals with the odor arising from the dorsoposterior aspect of the tongue.[3] The main compounds that lead to bad breath emanating from the oral cavity are the volatile sulfide compounds (VSC), especially hydrogen sulfide (H2S), methyl mercaptan (CH3SH), and dimethylsulfide [(CH3)2S].[4] These compounds are produced by the anaerobic Gram-negative microorganisms such as Treponema denticola, Porphyromonas gingivalis, Porphyromonas endodontalis, Prevotella intermedia, Bacteroides loescheii, Enterobacteriaceae, Tannerella forsythensis, Centipeda periodontii, Eikenella corrodens, and Fusobacterium nucleatum that inhabit the oral cavity.[5] The microorganisms interact with the sulfur-containing substances that are present in saliva, gingival crevicular fluid, blood, and cells leading to the production of odiferous products.[6]
Halitosis, a common condition, could be a serious social stigma. There are several agents that can temporarily mask the malodor like mouthrinses, chewing gum, etc., which in turn prevents the individual from reporting to the dentist for the conclusive treatment. Very rarely, this can have serious medical implications because there are numerous medical conditions that predispose to oral malodor.[7,8,9] There lies a necessity to enhance the knowledge of self-perception of oral and general health among dental students.[10] Therefore, it is essential both from a social and a medical point of view that halitosis is reported and a definitive remedy is given to treat the underlying cause.
The objectives of this present study were to evaluate self-perception of oral malodor by male and female dental students studying in Madha Dental College and Hospital, Chennai. The prevalence of oral hygiene habits and awareness of common dental problems such as dental caries, gingival bleeding, and dryness of mouth were also evaluated.
MATERIALS AND METHODS
Study population and recruitment
This study involved 285 dental undergraduate students of Madha Dental College and Hospital Chennai. This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Ethical Committee, Madha Dental College and Hospital. All the participants signed a written informed consent prior to the initiation of this study.
Structured questionnaire
A structured questionnaire was developed and tested on a pilot population prior to its administration in this study. The responses were evaluated and modifications were made as required. The final questionnaire included ten questions [Figure 1] which evaluated the presence, self-perception of halitosis, and treatment (self or professional) for halitosis. The oral hygiene habits of the subjects including toothbrushing frequency, use of interdental aids, and mouth rinses were also evaluated. The questionnaire was anonymous with no column for identification of the individual. The participants were explained about the questions, and clarifications were made. The questionnaire was administered in English language after confirming that all the participants were comfortable in the language.
Figure 1.
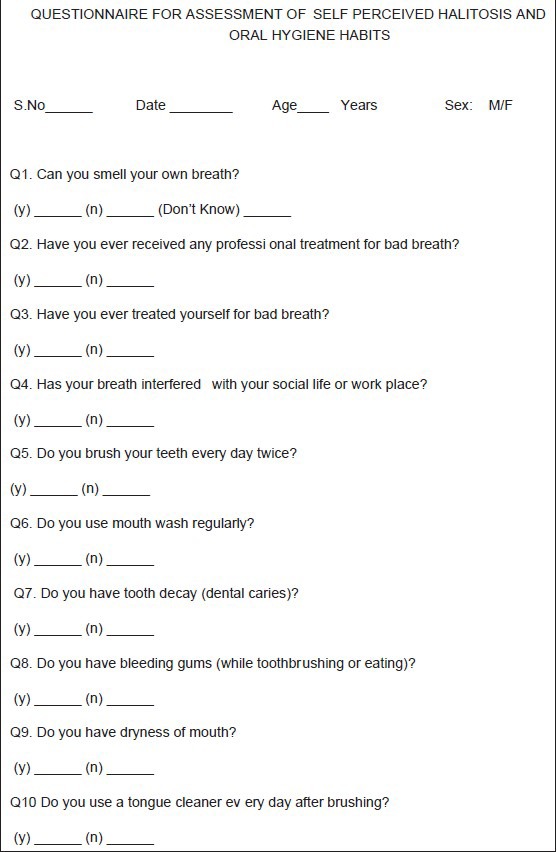
Questionnaire used in this study
Data analysis
Statistical package for social science version 15 was utilized for statistical analysis (SPSS, Inc., Chicago Illinois USA). The Chi square test was performed for comparison of responses obtained from males and females. The level of statistical significance was set at a P value less than 0.05.
RESULTS
The study population included 285 participants in the age range of 18 to 22 years. A total of 259 participants answered all the questions provided and were included for statistical analysis. Questionnaires that were incompletely filled were excluded from the final analysis. The overall response rate was 90%; of the 259, 120 (46.3%) were males and 139 (53.7%) were females.
Figure 2 shows the comparison for self-perception of halitosis. Among males, 26 (21.7%) reported perceiving halitosis, 77 (64.2%) gave a negative answer, and 17 (14.2%) were not aware of its presence or absence; where in females, 49 (35.3%) reported self-perception, 51 (36.7%) gave a negative response, and 39 (28.1%) were not aware of its presence or absence. The difference was found to be significant (P < 0.05).
Figure 2.
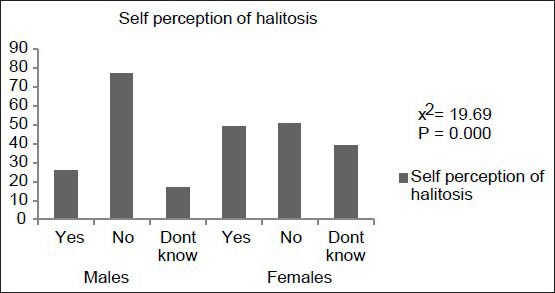
Frequency of self-perception of oral malodor
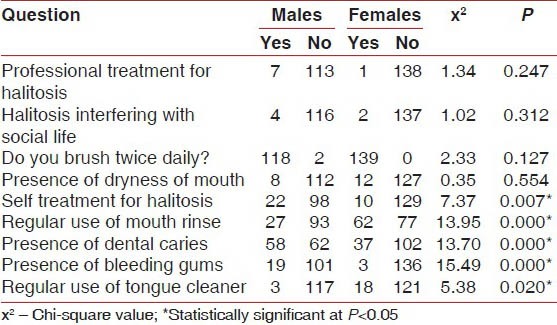
The answers to all the questions provided in the questionnaire were segregated according to gender and analyzed using the Chi-square test [Table 1]. Significant difference was observed for self-perception of halitosis, use of mouth wash, presence of carious teeth, bleeding gums, and use of tongue cleaners (P < 0.05).
Table 1.
Responses for the questions based on gender
DISCUSSION
To the best of our knowledge, this is the first study on the prevalence of halitosis among dental students in India. Since halitosis is a relatively common problem with many ramifications - personal, professional, and social effects - the data on its prevalence can be of importance. Literature reveals that the prevalence of halitosis ranges to around 50% in USA,[11] 27.5% in China,[12] and 22% in France.[13] This highlights the significance of halitosis as a widespread global problem. It has been estimated that in the developed world, 8 to 50% of people perceive oral malodor.[14] As dental professionals are most likely to diagnose halitosis, the percentage of individuals getting professional treatment for halitosis remains minimal.
The presence or absence of halitosis is often discerned by individuals on their own. The etiology could be either intraoral or extraoral causes. The diagnosis is usually subjective as there are no standard criteria that define a patient with halitosis.[1] The results of our study showed greater self-perception of halitosis among females (P > 0.05). This was similar to results obtained in previous studies.[10,15,16] Self-perception of halitosis is a psycho-physiological issue with multi-factorial etiology closely related to each individual's psychopathological profile.[17]
In younger individuals, the presence of oral malodor has been attributed to tongue coating in the absence of periodontal disease.[18] If oral hygiene is already good, or improves and yet oral malodor persists, the tongue may be the likely source of odor. The use of tongue cleaner was very minimal, which could be a reason for self-perception of halitosis in our study population. There is a positive correlation between the oral malodor and the levels of VSCs on the dorsum surface of the tongue and the propensity of microorganisms colonized on the surface of the tongue itself.[19,20] A recent systematic review concluded that tongue scraping may have a limited benefit in reducing oral malodor in the long term.[21]
The oral hygiene habits were excellent among the study population with most of the subject population reporting brushing twice daily. This was however anticipated as the subject population comprised of students. Effective toothbrushing and flossing can significantly reduce oral malodor, especially in people with poor oral hygiene and related gingival and periodontal disease.[22] The usage of mouthrinses was two-fold higher among females (44.6%) when compared with males (22.5%). This could imply a more conscious attitude among females than among males.
The prevalence of dental caries among the subject population was higher than that of gingival bleeding or dryness of mouth. Dental caries was reported higher in males than females as was gingival bleeding. The intraoral factors that are implicated in contributing to halitosis are tongue coating, gingival bleeding, and dental calculus.[13] The extraoral factors that are associated with halitosis include gastrointestinal tract disorders, chronic sinusitis, upper respiratory tract infections, and lower socioeconomic status.[1]
One drawback of this present study was the lack of correlation of self-perceived oral malodor with clinical- or laboratory-based evaluation.
CONCLUSION
Our results indicate that the prevalence of self-perceived malodor among dental students is in the similar range reported by other studies. However, these findings need to be corroborated by objective examination to ascertain the prevalence. The role of dental professionals in maintaining good oral health should be emphasized in the community.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Cortelli JR, Barbosa MD, Westphal MA. Halitosis: A review of associated factors and therapeutic approach. Braz Oral Res. 2008;22(Suppl 1):44–54. doi: 10.1590/s1806-83242008000500007. [DOI] [PubMed] [Google Scholar]
- 2.van den Broek AM, Feenstra L, de Baat C. A review of the current literature on management of halitosis. Oral Dis. 2008;14:30–9. doi: 10.1111/j.1601-0825.2006.01350.x. [DOI] [PubMed] [Google Scholar]
- 3.Yaegaki K, Sanada K. Volatile sulfur compounds in mouth air from clinically healthy subjects and patients with periodontal disease. J Periodontal Res. 1992;27:233–8. doi: 10.1111/j.1600-0765.1992.tb01673.x. [DOI] [PubMed] [Google Scholar]
- 4.Tonzetich J. Production and origin of oral malodor: A review of mechanisms and methods of analysis. J Periodontol. 1977;48:13–20. doi: 10.1902/jop.1977.48.1.13. [DOI] [PubMed] [Google Scholar]
- 5.Awano S, Gohara K, Kurihara E, Ansai T, Takehara T. The relationship between the presence of periodontopathogenic bacteria in saliva and halitosis. Int Dent J. 2002;52:212–6. doi: 10.1002/j.1875-595x.2002.tb00927.x. [DOI] [PubMed] [Google Scholar]
- 6.Quirynen M, Zhao H, Soers C, Dekeyser C, Pauwels M, Coucke W, et al. The impact of periodontal therapy and the adjunctive effect of antiseptics on breath odor-related outcome variables: A double-blind randomized study. J Periodontol. 2005;76:705–12. doi: 10.1902/jop.2005.76.5.705. [DOI] [PubMed] [Google Scholar]
- 7.Suarez F, Springfield J, Furne J, Levitt M. Differentiation of mouth versus gut as site of origin of odoriferous breath gases after garlic ingestion. Am J Physiol. 1999;276:G425–30. doi: 10.1152/ajpgi.1999.276.2.G425. [DOI] [PubMed] [Google Scholar]
- 8.Tangerman A, Winkel EG. Intra- and extra-oral halitosis: Finding of a new form of extra-oral blood-borne halitosis caused by dimethyl sulphide. J Clin Periodontol. 2007;34:748–55. doi: 10.1111/j.1600-051X.2007.01116.x. [DOI] [PubMed] [Google Scholar]
- 9.Moshkowitz M, Horowitz N, Leshno M, Halpern Z. Halitosis and gastroesophageal reflux disease: A possible association. Oral Dis. 2007;13:581–5. doi: 10.1111/j.1601-0825.2006.01341.x. [DOI] [PubMed] [Google Scholar]
- 10.Almas K, Al-Hawish A, Al-Khamis W. Oral hygiene practices, smoking habit, and self-perceived oral malodor among dental students. J Contemp Dent Pract 2003. 15;4:77–90. [PubMed] [Google Scholar]
- 11.Lee SS, Zhang W, Li Y. Halitosis update: A review of causes, diagnoses, and treatments. J Calif Dent Assoc. 2007;35:258–60. 262, 264-8. [PubMed] [Google Scholar]
- 12.Liu XN, Shinada K, Chen XC, Zhang BX, Yaegaki K, Kawaguchi Y. Oral malodor-related parameters in the Chinese general population. J Clin Periodontol. 2006;33:31–6. doi: 10.1111/j.1600-051X.2005.00862.x. [DOI] [PubMed] [Google Scholar]
- 13.Frexinos J, Denis P, Allemand H, Allouche S, Los F, Bonnelye G. Descriptive study of digestive functional symptoms in the French general population. Gastroenterol Clin Biol. 1998;22:785–91. [PubMed] [Google Scholar]
- 14.Porter SR, Scully C. Oral malodor (halitosis) BMJ. 2006;333:632–5. doi: 10.1136/bmj.38954.631968.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Al-Ansari JM, Boodai H, Al-Sumait N, Al-Khabbaz AK, Al-Shammari KF, Salako N. Factors associated with self-reported halitosis in Kuwaiti patients. J Dent. 2006;34:444–9. doi: 10.1016/j.jdent.2005.10.002. [DOI] [PubMed] [Google Scholar]
- 16.Bosy A. Oral malodor: Philosophical and practical aspects. J Can Dent Assoc. 1997;63:196–201. [PubMed] [Google Scholar]
- 17.Eli I, Baht R, Koriat H, Rosenberg M. Self-perception of breath odor. J Am Dent Assoc. 2001;132:621–6. doi: 10.14219/jada.archive.2001.0239. [DOI] [PubMed] [Google Scholar]
- 18.Miyazaki H, Sakao S, Katoh Y, Takehara T. Correlation between volatile sulphur compounds and certain oral health measurements in the general population. J Periodontol. 1995;66:679–84. doi: 10.1902/jop.1995.66.8.679. [DOI] [PubMed] [Google Scholar]
- 19.Morita M, Wang HL. Relationship between sulcular sulfide level and oral malodor in subjects with periodontal disease. J Periodontol. 2001;72:79–84. doi: 10.1902/jop.2001.72.1.79. [DOI] [PubMed] [Google Scholar]
- 20.Hinode D, Fukui M, Yokoyama N, Yokoyama M, Yoshioka M, Nakamura R. Relationship between tongue coating and secretory-immunoglobulin A level in saliva obtained from patients complaining of oral malodor. J Clin Periodontol. 2003;30:1017–23. doi: 10.1046/j.0303-6979.2003.00407.x. [DOI] [PubMed] [Google Scholar]
- 21.Outhouse TL, Al-Alawi R, Fedorowicz Z, Keenan JV. Tongue scrapping for treating halitosis. Cochrane Database Sys Rev. 2006;2:CD005519. doi: 10.1002/14651858.CD005519.pub2. [DOI] [PubMed] [Google Scholar]
- 22.Morita M, Wang HL. Association between oral malodor and adult periodontitis: A Review. J Clin Periodontol. 2001;28:813–9. doi: 10.1034/j.1600-051x.2001.028009813.x. [DOI] [PubMed] [Google Scholar]