

Abstract
Graves’ disease in adolescents and adults usually presents with classic symptoms including weight loss, frequent stools, irritability, and heat intolerance. However, the clinical manifestations of hyperthyroidism in young children are often subtle, unrecognized, and atypical. Here, we report a 6 year-old girl who presented for evaluation of increased thirst. Review of systems was negative with respect to weight loss, irritability, palpitations, diarrhea, and school performance problems. Physical exam was unremarkable except for an enlarged thyroid gland. Her identical twin sister, who incidentally accompanied her to clinic, also had a previously unidentified goiter. Testing for diabetes was negative. Further laboratory investigation was consistent with Graves’ disease in both girls. Polydipsia is a rare and unusual presenting feature of hyperthyroidism in children. The evolution of this case highlights the importance of maintaining a high index of suspicion for thyroid disease during childhood.
Keywords: polydipsia, polyuria, identical twins, Graves’ disease, hyperthyroidism
PATIENT REPORT
A previously healthy 6 year-old girl presented for evaluation of possible diabetes because of increased thirst and urinary frequency over the past six months. The patient’s mother had been intermittently testing her daughter’s blood sugar at home with a glucometer. Blood sugar readings ranged between 4.4 mmol/L (80 mg/dL) to 10.0 mmol/L (180 mg/dL). The patient often carried a water bottle with her at home and at school. Although her symptoms were most prominent during the day, she had recently experienced multiple episodes of secondary nocturnal enuresis. Review of systems was otherwise negative with respect to vomiting, abdominal pain, weight loss, irritability, hyperactivity, palpitations, diarrhea, diaphoresis, and school performance problems. Family history was positive for several relatives with auto-immune thyroid disease.
Growth parameters were between the 75th and 90th percentiles for height and between the 25th and 50th percentiles for weight. Blood pressure was 112/56 and heart rate was 91 beats per minute. Physical exam was unremarkable except for a symmetrically enlarged, smooth thyroid gland without tenderness, nodules, or cervical lymphadenopathy. No tremor or ophthalmologic findings were appreciated. Her identical twin sister, who incidentally accompanied the patient to clinic, was also found to have a previously unidentified enlarged thyroid gland (Figure). Upon further questioning, the patient’s twin also reported increased thirst and urination over the last few months, but to a lesser degree than her sister.
Figure.
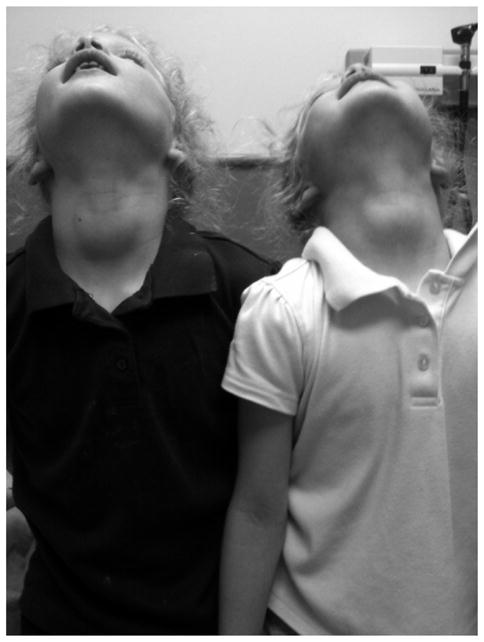
Identical twin girls with goiters.
Laboratory testing for diabetes was negative, including a hemoglobin A1C of 5.4% (reference range 4.0–5.9%) and a random non-fasting blood sugar of 5.9 mmol/L (107 mg/dL). Due to the patient’s enlarged thyroid gland, additional laboratory tests were obtained. Thyroid testing revealed a suppressed TSH, elevated T4 and T3, positive TSH receptor antibody (TRAb), positive thyroid peroxidase (TPO) antibody, and negative thyroglobulin (Tg) antibody. Her twin sister also had thyroid testing with similar laboratory values (Table).
TABLE.
Thyroid laboratory results.
| Laboratory Test (metric units) | Twin A | Twin B | Reference Range |
|---|---|---|---|
| TSH: mIU/L (mcU/ml) | 0.013 (0.013) | 0.045 (0.045) | 0.4–4.2 (0.4–4.2) |
| Total T4: nmol/L (μg/dL) | 208.5 (16.2) | 202 (15.7) | 72–166 (5.6–12.9) |
| Total T3: nmol/L (ng/dL) | 6.47 (420) | 5.27 (342) | 1.26–2.77 (82–179) |
| TRAb: IU/L | 11 | 24 | ≤1.75 |
| TPO antibody: IU/mL | 353.3 | >1000.0 | 0.0–3.9 |
| Tg antibody: IU/mL | 2.4 | <1.8 | <4.0 |
Based on these results, the twins were diagnosed with Graves’ disease. Treatment options, including anti-thyroid drug therapy, radioactive iodine, and thyroidectomy, were discussed with the family. Due to the patients’ young age, anti-thyroid drug therapy with methimazole was initiated. After a few weeks, the polydipsia and polyuria gradually resolved corresponding to the biochemical resolution of hyperthyroidism in both girls.
DISCUSSION
Graves’ disease is the most common cause of hyperthyroidism in children, adolescents, and adults. Prevalence rates are six to eight times greater in females compared to males. Older children and adults often present with typical symptoms, including weight loss, frequent stools, irritability, heat intolerance, or neck swelling1. However, the clinical manifestations of hyperthyroidism in young children are often subtle or atypical, which can delay the diagnosis and treatment by several months2,3. This delay in treatment not only negatively impacts quality of life, but it also decreases the likelihood of achieving long-term remission from hyper-thyroidism2. Subtle manifestations of Graves’ disease in young, prepubertal children include growth acceleration and tachycardia, which can easily be overlooked or misinterpreted by parents and healthcare providers3.
Polydipsia has been described as a presenting feature of hyperthyroidism in adults4. Studies have shown that hyperthyroid patients have increased micturition frequency as well as nocturia when compared to patients who are not hyperthyroid5. However, symptoms of polydipsia and polyuria are rarely described or appreciated in children presenting with hyperthyroidism. After reviewing the medical literature, we are aware of only one other report of a 9-year-old boy from Germany with Graves’ disease in which polyuria was part of the initial clinical presentation6.
The development of Graves’ disease involves a complex interplay between various immune responses and potential environmental factors in genetically predisposed individuals. Susceptibility genes encoding for proteins involved in immunologic regulation as well as those specific to the thyroid gland have been implicated to increase the risk of developing Graves’ disease7. Genetic studies have found a higher concordance of autoimmune thyroid disease, including Graves’ disease, in monozygotic twins as compared to dizygotic twins8. While autoimmune thyroid disease has previously been noted in identical and non-identical twins9,10, the simultaneous diagnosis of Graves’ disease in young identical twins has not been previously reported.
In summary, this case represents the unique constellation of an atypical presentation of hyperthyroidism along with its unexpected coexistence in the patient’s identical twin sister. The evolution of this case highlights the importance of maintaining a high index of suspicion for thyroid disease during childhood, and of being alert to the possibility of serendipitously uncovering related pathology among siblings that come to medical visits.
Footnotes
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare related to this report.
References
- 1.Birrell G, Cheetham Juvenile thyrotoxicosis; can we do better? Arch Dis Child. 2004;89:745–750. doi: 10.1136/adc.2003.035980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shulman DI, Muhar I, Jorgensen EV, Diamond FB, Bercu BB, Root AW. Autoimmune hyperthyroidism in prepubertal children and adolescents: comparison of clinical and biochemical features at diagnosis and responses to medical therapy. Thyroid. 1997;7:755–760. doi: 10.1089/thy.1997.7.755. [DOI] [PubMed] [Google Scholar]
- 3.Lazar L, Kalter-Leibovici O, Pertzelan A, Weintrob N, Josefsberg Z, Phillip M. Thyrotoxicosis in prepubertal children compared with pubertal and postpubertal patients. J Clin Endocrinol Metab. 2000;85:3678–3682. doi: 10.1210/jcem.85.10.6922. [DOI] [PubMed] [Google Scholar]
- 4.Evered DC, Hayter CJ, Surveyor I. Primary polydipsia in thyrotoxicosis. Metabolism. 1972;21:393–404. doi: 10.1016/0026-0495(72)90052-2. [DOI] [PubMed] [Google Scholar]
- 5.Andersen LF, Agner T, Walter S, Hansen JM. Micturition pattern in hyperthyroidism and hypothyroidism. Urology. 1987;29:223–224. doi: 10.1016/0090-4295(87)90161-0. [DOI] [PubMed] [Google Scholar]
- 6.Meir J, Roessner D, Eggert P. Enuresis in hyperthyroidism: a temporary lack of central control mechanism leads to nocturnal enuresis. Acta Paediatr. 2009;99:145–146. doi: 10.1111/j.1651-2227.2009.01511.x. [DOI] [PubMed] [Google Scholar]
- 7.Brown RS. Autoimmune thyroid disease: unlocking a complex puzzle. Curr Opin Pediatr. 2009;21:523–528. doi: 10.1097/MOP.0b013e32832cf824. [DOI] [PubMed] [Google Scholar]
- 8.Jacobson EM, Tomer Y. The genetic basis of thyroid autoimmunity. Thyroid. 2007;17:949–961. doi: 10.1089/thy.2007.0153. [DOI] [PubMed] [Google Scholar]
- 9.Brix TH, Kyvik KO, Christensen K, Hegedus L. Evidence for a major role of heredity in Graves’ disease: a population-based study of two Danish twin cohorts. J Clin Endocrinol Metab. 2001;86:930–934. doi: 10.1210/jcem.86.2.7242. [DOI] [PubMed] [Google Scholar]
- 10.Ringold DA, Nicoloff JT, Kesler M, Davis H, Hamilton A, Mack T. Further evidence for a strong genetic influence on the development of autoimmune thyroid disease: the California twin study. Thyroid. 2002;12:647–53. doi: 10.1089/105072502760258613. [DOI] [PubMed] [Google Scholar]