

Abstract
Single coronary arteries are rare congenital anomalies in which the whole heart circulation is supplied by a coronary artery arising from a single ostium. Single left coronary artery with right coronary artery (RCA) originating from distal left circumflex artery (LCX) is a very rare anomaly with only few cases reported in the literature. We report a 44 years old male presenting with anterior myocardial infarction who was found to have a single left coronary artery during angiography. RCA had an abnormal origin arising from distal of a dominant LCX that retrogradely followed the course of a normal RCA to the base of the heart. A brief review of the reported cases with emphasis on the clinical significance of this unusual anomaly is presented.
Keywords: Coronary Anomaly, Myocardial Infarction, Coronary Angiography
Case History
A 44 years old man was referred to our hospital for coronary angiography. He had a history of anterior myocardial infarction four days earlier for which he had received streptokinase in another hospital and had been referred to our center for coronary angiography for recurrent ischemic symptoms. His past medical history was otherwise unremarkable. He didn’t report a history of smoking. He had developed recurrent chest pain on the third day of his admission that had been refractory to intensification of anti-ischemic therapy. Transthoracic echocardiography showed a left ventricular ejection fraction of 45%, hypokinetic anterior and apical segments and trivial mitral regurgitation. Right ventricular (RV) size and function were normal. He was scheduled for coronary angiography. During catheterization only one coronary ostium originating from left coronary cusp could be cannulated and several attempts with different catheters to identify the right coronary artery (RCA) ostium failed. Injection of contrast medium didn’t show any coronary artery originating from right coronary cusp. The patient had a single coronary artery arising from left coronary cusp. RCA had an abnormal origin arising from distal of a dominant left circumflex artery (LCX) that retrogradly followed the course of a normal RCA to the base of the heart (Figure 1). Left anterior descending artery (LAD) was cut off just after first septal branch with no angiographically visible antegrade or retrograde distal flow. A bare metal stent was deployed. The patient’s symptoms resolved completely following the procedure and he was discharged 2 days after percutaneous coronary intervention (PCI) without any complication. A myocardial perfusion scan performed six months after the index event showed scar tissue in anterior myocardial wall. Other segments did not show any abnormality. The patient was asymptomatic in 3 years follow up.
Figure 1 .
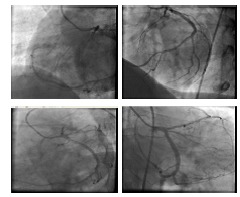
Retrograde filling of RCA from distal LCX shown in LAO (A), LAO cranial (B), LAO caudal (C) and shallow RAO with deep caudal (D) projections . A-C are before and D is after PCI.
Discussion
Single left coronary artery with anomalous origin of right coronary artery arising as a continuation of distal left circumflex artery is a very rare congenital coronary anomaly with few reported cases in the literature.1-22 Table 1 summarizes the demographics, angiography data, associated conditions, treatment options and follow-up data for the reported cases. Nine female and 15 male patients (age range: 30-77 years) have been reported (Table 1 ).1-22 This anomaly is compatible with L1 type of extensively used Lipton classification of coronary anomalies in which a single coronary artery from left sinus of valsalva divides to LAD and LCX, and distal LCX continues its course beyond the crux in to the atrioventricular groove and follows the course of a normal RCA to the base of the heart.6,12 Right coronary ostium is congenitally absent. Though single coronary arteries are often associated with other congenital anomalies12 and could be associated with the development of cardiac ischemia, cardiomyopathy, sudden cardiac death and congestive heart failure14, this particular anomaly has been reported to have a clinically benign course unless there are significant atherosclerotic lesions compromising the coronary flow.10,12,14,20 Majority of reported cases had a benign course and negative ischemic work up in the absence of coronary lesions.2,4,6,11-14,21 Choi et al. report a similar patient who presented with atypical chest pain. They attributed her chest discomfort to possible myocardial ischemia from abnormally slow coronary flow to the RCA and successfully treated the patient with calcium channel blocker and nitrates.13 On the other hand a 30 years old male with chest discomfort had mild posterolateral ischemia on perfusion imaging in the absence of any atherosclerotic lesion.4 Association with atrial fibrillation (AF) and severe mitral regurgitation (MR) have also been reported.7,18 Ma et al. report a similar patient who presented with right ventricular infarction and was treated with coronary stenting in distal LCX.19 Incidental finding during coronary CT angiography for the evaluation of atypical chest pain has been described.20 Ghaffari et al. described a patient with prolonged hemodynamic instability following a massive pulmonary embolism who was found to have a single left coronary artery. They attributed the prolonged and disproportionate RV dysfunction to its insufficient perfusion in the setting of acute pulmonary hypertension and absence of proximal RCA.15
Table 1. Summary of characteristics of reported cases with this unusual anomaly .
| Case | Author/Year | Age/Sex | Presenting Symptom | Angiography | Associated Conditions | Further imaging | Treatment | Outcome |
| 1 | Tavernarakis 1986 | 57/M | TCP | LAD lesion | None | None | NA | NA |
| 2 | Sheth 1988 | 60/M | ATCP | No lesion | None | None | None | NA |
| 3 | Vrolix 1991 | 51/M | TCP | LCX lesion | None | None | CABG | |
| 4 | Shammas 2001 | 44/F | Chest pain | No lesion | None | None | None | NA |
| 5 | Shammas 2001 | 30/M | Dyspnea/chest discomfort | No lesion | None | Mild posterolateral ischemia in MPI | None | NA |
| 6 | Turhan 2003 | 52/M | ATCP | No lesion | None | None | None | NA |
| 7 | Asha 2003 | 62/M | UA | LCX & LAD lesion | None | None | CABG | Uneventful recovery |
| 8 | Yoshimoto 2004 | 63/M | ATCP | No lesion | Atrial fibrillation | None | Oral anticoagulation for AF | NA |
| 9 | Chou 2004 | 42/M | TCP | 40% lesion in LCX | None | Anteroapical ischemia in MPI | Medical | Asymotimatic at 1.5 yrs f/u |
| 10 | Kunimasa 2007 | 61/M | MI | LAD lesion | None | MSCT | NA | NA |
| 11 | Celik 2008 | 57/M | TCP | No lesion | None | Normal MPI | Medical | Asymptomatic at 1 yr f/u |
| 12 | Tanawuttiwat 2009 | 44/F | ATCP | No lesion | None | Normal DSE | Medical | NA |
| 13 | Datta 2010 | 69/F | TCP | No lesion | None | None | None | Asymptomatic at 1 yr f/u |
| 14 | Choi 2010 | 68/F | ATCP | No lesion | None | Normal MPI | NA | Symptoms resolved with CCB and nitrate |
| 15 | Chung 2010 | 77/F | TCP | LAD lesion | None | Normal MPI | PCI on LAD | NA |
| 16 | Ghaffari 2010 | 65/F | Dyspnea | No lesion | Massive pulmonary embolism | None | Medical | Dyspnea at 3 months f/u |
| 17 | Voyce 2010 | 76/F | RVMI | LAD and LCX lesion | None | None | PCI on LCX | Asymotimatic at 3 yrs f/u |
| 18 | Sonmez 2011 | 63/F | Subacute MI | LAD lesion | None | None | PCI on LAD | NA |
| 19 | Turfan 2012 | 58/M |
exertional dyspnea and chest pain |
Mid LAD lesion |
Severe mitral regurgitation | None | Mitral valve surgery | NA |
| 20 | Ma 2012 | 39/M | RV MI | Distal LCX occlusion | None | None | PCI on LCX | NA |
| 21 | Blaschke 2013 | 59/F | TCP | No lesion | None | Negative DSE and Stress-perfusion cardiac MRI | None | NA |
| 22 | De Augustin 2014 | 40/M | ATCP | No lesion | None | Inconclusive EST,MSCT | Conservative | NA |
| 23 | Pourbehi 2014 | 47/M | MI | LCX & LAD lesion | None | None | PCI | Asymptomatic at 8 months f/u |
| 24 | Present case | 44/M | MI | LAD lesion | None | None | PCI | Asymptomatic at 3 years f/u |
ATCP=atypical chest pain, TCP= typical chest pain, PCI= percutaneous coronary intervention, MI= myocardial infarction, M=male, F= female, DSE= dobutamine stress echocardiography, MPI= myocardial perfusion imaging, UA= unstable angina, AF=atrial fibrillation, CABG= coronary artery bypass grafting, f/u=follow-up, RV=right ventricle, CCB= calcium channel blocker, NA= not available
Our patient similar to most of the reported cases didn’t have objective evidence of ischemia in the territory of RCA. Anomalous origin of RCA from distal continuation of LCX though extremely rare, seems to be an isolated and benign congenital anomaly in the absence of atherosclerotic lesions and it is unlikely that the anomaly causes myocardial ischemia. Actually left ventricular perfusion in these patients is very similar to that of normal subjects with LCX dominant coronary system. The main difference could be RV perfusion through RV branches. We postulated that the most vulnerable segments to ischemia in these patients could be in RV as described in few case reports of acute RV strain in the setting of pulmonary embolism15 or RV infarction since collateral circulation from proximal to distal RCA are not developed.16,19 Associated conditions are extremely uncommon and only one case of AF and one patient with severe MR are described in the literature. However coronary lesions could be of more critical significance because of the dependence of the heart’s circulation on a single coronary. Coronary artery bypass grafting and PCI have been described in a few cases with associated coronary atherosclerosis.
Ethical issues
The study was approved by the Ethics Committee of the University.
Competing interests
Authors declare no conflict of interest in this study.
References
- 1.Tavernarakis A, Voudris V, Ifantis G, Tsaganos N. Anomalous origin of the right coronary artery arising from the circumflex artery. Clin Cardiol. 1986;9:230–232. doi: 10.1002/clc.4960090514. [DOI] [PubMed] [Google Scholar]
- 2.Sheth M, Dovnarsky M, Cha SD, Kini P, Maranhao V. Single coronary artery: right coronary artery originating from distal left circumflex. Cathet Cardiovasc Diagn. 1988;14:180. doi: 10.1002/ccd.1810140310. [DOI] [PubMed] [Google Scholar]
- 3.Vrolix MC, Geboers M, Sionis D, De Geest H, Van de Werf F. Right coronary artery originating from distal circumflex: an unusual feature of single coronary artery. Eur Heart J. 1991;12:746. doi: 10.1093/eurheartj/12.6.746. [DOI] [PubMed] [Google Scholar]
- 4.Shammas RL, Miller MJ, Babb JD. Single left coronary artery with origin of the right coronary artery from distal circumflex. Clin Cardiol. 2001;24:9–2. doi: 10.1002/clc.4960240115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Turhan H, Duru E, Yetkin E, Atak R, Senen K. Right coronary artery originating from distal left circumflex: an extremely rare variety of single coronary artery. Int J Cardiol. 2003;88:309–11. doi: 10.1016/s0167-5273(02)00324-8. [DOI] [PubMed] [Google Scholar]
- 6.Asha M, Sriram R, Mukundan S, Abraham K. Single Coronary Artery from the Left Sinus With Atherosclerosis. Asian Cardiovasc Thorac Ann. 2003;11:163. doi: 10.1177/021849230301100217. [DOI] [PubMed] [Google Scholar]
- 7.Yoshimoto S, Hirooka K, Irino H, Abe H, Yasuoka Y, Yamamoto H. et al. Anomalous right coronary artery originating from the distal left circumflex artery: single coronary artery with choronic atrial fibrillation. Jpn Heart J. 2004;45:679–83. doi: 10.1536/jhj.45.679. [DOI] [PubMed] [Google Scholar]
- 8.Chou LP, Kao C, Lin SL. Right coronary artery originating from distal left circumflex artery in a patient with an unusual type of isolated single coronary artery. Jpn Heart J. 2004;45:337–42. doi: 10.1536/jhj.45.337. [DOI] [PubMed] [Google Scholar]
- 9.Kunimasa T, Sato Y, Ito S, Takagi T, Lee T, Saeki F. et al. Absence of the right coronary artery detected by 64-detector-row multislice computed tomography. Int J Cardiol. 2007;115:249–50. doi: 10.1016/j.ijcard.2006.01.039. [DOI] [PubMed] [Google Scholar]
- 10.Celik T, Iyisoy A, Yüksel C, Işik E. Anomalous right coronary artery arising from the distal left circumflex coronary artery. Anadolu Kardiyol Derg. 2008;8:459–60. [PubMed] [Google Scholar]
- 11.Tanawuttiwat T, Harindhanavudhi T, Trivedi D. Anomalous Single Coronary Artery with Absent Right Coronary Artery Diagnosed with the Aid of 64-Slice Multidetector Computed Tomographic Angiography. Tex Heart Inst J. 2009;36:362–3. [PMC free article] [PubMed] [Google Scholar]
- 12.Datta S, Moussa T, Hussain F. Anomalous right coronary artery originating from the distal left circumflex artery: a novel coronary artery anomaly viewed by computed tomography and invasive angiography. Can J Cardiol. 2010;26:213. doi: 10.1016/s0828-282x(10)70404-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Choi HY, Kim JW, Moon JM, Kim YJ, Choi CU, Lim HE. et al. Unusual dominant course of left circumflex coronary artery to right coronary artery territory with absent right coronary artery. J Cardiol. 2010;55:117–9. doi: 10.1016/j.jjcc.2009.03.014. [DOI] [PubMed] [Google Scholar]
- 14.Chung SK, Lee SJ, Park SH, Lee SW, Shin WY, Jin DK. An extremely rare variety of anomalous coronary artery: right coronary artery originating from the distal left circumflex artery. Korean Circ J. 2010;40:465–7. doi: 10.4070/kcj.2010.40.9.465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ghaffari S, Pourafkari L. Pulmonary embolism in a patient with a rare coronary anomaly — a clue to the importance of proximal right coronary artery branches. Kardiol Pol. 2010;68(7):844–6. [PubMed] [Google Scholar]
- 16.Voyce SJ, Abughnia H. An unusual cause of right ventricular myocardial infarction. J Invasive Cardiol. 2010;22:E172–5. [PubMed] [Google Scholar]
- 17.Sönmez O, Gül EE, Altunbaş G, Ozdemir K. Right coronary artery arising from the distal left circumflex artery. Turk Kardiyol Dern Ars. 2011;39:325–7. doi: 10.5543/tkda.2011.00769. [DOI] [PubMed] [Google Scholar]
- 18.Turfan M, Aydin C, Elbey MA, Erdogan E, Asoglu E, Basel H. et al. Right coronary artery originating from the distal left circumflex artery, evaluation using three imaging techniques. CLINICS. 2012;67:1517–8. doi: 10.6061/clinics/2012(12)28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ma SH, Kim DH, Hur JY, Kim KS, Byun SJ, Park KH. et al. Right Ventricular Myocardial Infarction due to Right Coronary Artery Total Occlusion Originating From the Distal Left Circumflex Artery. Korean Circ J. 2012;42:565–7. doi: 10.4070/kcj.2012.42.8.565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Blaschke F, Zimmermann E, Greupner J, Zohlnhoefer D, Krackhard T, Haverkamp W. et al. A Rare Case of a Congenital Single Coronary Artery: Right Coronary Artery Originating From the Distal Left Circumflex Artery. Vascular Disease Management. 2013;10:E244–7. [Google Scholar]
- 21. de Agustin JA, Gomez de Diego JJ, Marcos-Alberca P, Rodrigo JL, Almeria C, Nuñez-Gil IJ, et al. Single left coronary artery with the right coronary artery arising as a continuation from the distal circumflex coronary artery assessed by multislice computed tomography. Int J Cardiol 2014. pii: S0167-5273(14)00825-0. [DOI] [PubMed]
- 22.Pourbehi MR, Amini A, Farrokhi S. Single coronary artery with anomalous origin of the right coronary artery from the distal portion of left circumflex artery: a very rare case. J Tehran Heart Cent. 2013;8:161–3. [PMC free article] [PubMed] [Google Scholar]