

Abstract
We compare estimates of multiple and concurrent sexual partnerships from Demographic and Health Surveys (DHS) with comparable Population Services International (PSI) surveys in four African countries (Kenya, Lesotho, Uganda, Zambia). DHS data produce significantly lower estimates of all indicators for both sexes in all countries. PSI estimates of multiple partnerships are 1.7 times higher [1.4 for men (M), 3.0 for women (W)], cumulative prevalence of concurrency is 2.4 times higher (2.2 M, 2.7 W), the point prevalence of concurrency is 3.5 times higher (3.5 M, 3.3 W), and the fraction of multi-partnered persons who report concurrency last year is 1.4 times higher (1.6 M, 0.9 W). These findings provide strong empirical evidence that DHS surveys systematically underestimate levels of multiple and concurrent partnerships. The underestimates will contaminate both empirical analyses of the link between sexual behavior and HIV infection, and theoretical models for combination prevention that use these data for inputs.
Keywords: Sexual behavior, Data validation, Multiple and concurrent partnerships, HIV, Combination prevention
Introduction
Accurate, population-specific data on sexual behavior are needed for HIV prevention programming, including modeling the impact of treatment as prevention (TasP) and combination prevention packages. In addition, sexual behavior data are key to understand the direction of the epidemic and to measure the effectiveness of many behavioral interventions. In the generalized heterosexual epidemics that account for the majority of the global burden of HIV, rates of sexual partner acquisition and concurrent partnerships are some of the key variables.
There is an important interaction between the timing and sequence of partnerships and the short peak in infectivity (the “acute stage”) that occurs immediately after HIV infection [1, 2]. Though it lasts only a few weeks, the tenfold increase in transmission probability during the acute stage gives it a disproportionate impact: an estimated 25–40 % of all transmissions in the sub-Saharan African region occur during this stage [2, 3]. The timing of partnerships influences this impact. Once a person becomes infected, he or she only has a month or two to expose another partner during the acute stage. With serial monogamy, this can only happen if the rates of partner change are rapid enough that the original partnership dissolves and a new partner is acquired during this short acute stage. In contrast, with concurrency the rates of partner acquisition may be low, but the overlap in partnerships helps to ensure that another partner will be exposed during the acute stage. The acute stage is short and undetectable using traditional HIV antibody tests, so it will be difficult to capture with prevention strategies that rely on traditional testing. As a result, concurrency and partner reduction may be a useful strategy to complement TasP, particularly in hyperendemic settings where the principal mode of transmission is heterosexual intercourse and rates of partner acquisition are low. This makes it important to have good estimates of the prevalence of multiple partnerships and concurrency, for both combination prevention planning and program impact assessment.
The most comprehensive source of comparable, population-based, representative data on rates of sexual partner acquisition and concurrency are the Demographic and Health Surveys (DHS) [4]. Originally designed to collect data on nutrition, fertility and maternal and child health from women, the surveys have grown to collect a wide range of sociodemographic and behavioral data, with optional questionnaires for men, specialty surveys focusing on HIV/AIDS (the “AIDS Indicator Surveys”, or AIS), and collection of HIV infection biomarkers. In 1999 the DHS/ AIS added optional questionnaire modules on sexual partnerships to collect data on up to the three most recent sexual partners in the last 12 months. With some limitations, these data allow us to estimate the two recommended indicators of concurrency: point prevalence and cumulative annual prevalence.
The goal of this study is to assess the validity of the DHS data on multiple and concurrent partnerships in the sub-Saharan African region. We focus on this region because it has the largest concentration of generalized heterosexual HIV epidemics, and evidence suggests that the patterns of overlap in sexual partnerships, rather than high rates of partner acquisition, may be part of the explanation [5]. The validity of self-reported sexual behavior is often questioned, and generally recognized to be difficult to verify. There are no gold standards for validation, with a few exceptions when biomarkers can be used to rule out possibilities. Our approach is therefore to conduct a systematic comparison of behavioral estimates drawn from a different source: the nationally representative datasets collected by Population Services International (PSI) as part of their Tracking Results Continuously (TRaC) Surveillance system. The PSI HIV TRaC survey is used to measure levels, trends, and determinants of HIV-related risk behaviors to evaluate and improve its programming. While sexual behavior surveys are common in this region, PSI is the only organization that conducts cross-sectional studies across multiple countries with comparable national coverage and nearly identical questionnaire design.
Consistency between the DHS and PSI estimates is not necessarily an indicator of validity, but inconsistency is informative. At minimum, it is a good indicator of unreliable data, and systematically lower estimates for one of the studies across all countries and population subgroups are a strong indication the data from this study do not provide valid estimates of sexual behavior.
Data and Methods
Sampling and Measures
The data come from our countries in sub-Saharan Africa shown in Table 1 [6–9]. Each of these countries had a DHS and a PSI survey conducted within 2–3 years of each other. The sampling methodology and questionnaire items are comparable. Samples are designed to be nationally representative, and both organizations use the list of enumeration areas developed by the national statistical offices of each country. The DHS employ stratified two-stage cluster designs and provide a sample weights that adjust for both stratification and response rates in public data sets. PSI also employs two-stage cluster designs with equal probability of selection (the sample is self-weighted, except for Kenya which has sample weights). The DHS is generally regarded as representing the state of the art for measurement, so their questionnaire items are often adopted by other organizations, including PSI. As a result, the wording for the sexual behavior questions examined here are nearly identical for all surveys (Exact questionnaire wording can be found in the supplemental Web material A1).
Table 1.
Sample characteristics
| Kenya | Lesotho | Uganda | Zambia | |
|---|---|---|---|---|
| Year of study | ||||
| DHS | 2008–2009 | 2009–2010 | 2006 | 2007 |
| PSI | 2011 | 2008 | 2008 | 2009 |
| Unweighted sample size | ||||
| DHS | 9,753 | 6,597 | 5,358 | 11,312 |
| PSI | 3,180 | 1,211 | 1,869 | 2,680 |
| % Femalea | ||||
| DHS | 56.3 | 53.6 | 52.6 | 55.2 |
| PSI | 51.3 | 61.1 | 52.3 | 49.8 |
| % Urbana | ||||
| DHS | 26.9 | 31.1 | 13.3 | 40.3 |
| PSI | 23.6 | 51.9 | 13.9 | 39.9 |
| % Marrieda | ||||
| DHS | 65.0 | 49.6 | 100.0 | 67.5 |
| PSI | 63.1 | 45.8 | 100.0 | 66.2 |
| Mean Agea | ||||
| DHS | 30.5 | 24.7 | 34.4 | 29.9 |
| PSI | 29.4 | 24.0 | 33.1 | 29.0 |
| Range | 15–49 | 15–39 | 24–49 | 15–49 |
Weighted by original study sample weights
Samples for this analysis are restricted to the sexually active population. Within country, samples were further restricted by age and marital status, if necessary, for comparability. Kenya and Zambia include persons age 15–49 (the standard DHS age range), but the range for Uganda was 24–49, and for Lesotho was 15–39 due to more restricted PSI criteria. In addition, the Ugandan samples were restricted to married or cohabiting respondents due to PSI criteria. The resulting sample descriptions are shown in Table 1.
Our comparison focuses on two types of sexual behavior: multiple sexual partners reported in the last 12 months, and concurrent partnerships (point and cumulative prevalence). We use the consensus definition and indicators of concurrency [10]. Comparisons are based on four indicators which successively narrow down the sources of discrepancies across the surveys. The first indicator is the prevalence of persons reporting multiple partners in the past year. This is based on the number of partners reported in the summary question: “In total, with how many different people have you had sexual intercourse in the last 12 months?” Anyone reporting more than one partner is coded as having had multiple partners. The second indicator is the cumulative prevalence of concurrency. This uses the dates of first and last sex with each partner to identify overlap in the sexual partnership intervals during the last 12 months. The third is the point prevalence of concurrency. This also uses the partnership intervals constructed above, and identifies concurrency at single point in time, 6 months prior to the date of interview. The last indicators are the point and cumulative prevalence of concurrency among persons who report multiple partners in the last year.
Both of the concurrency measures depend on dating partnership intervals, so it is necessary to adopt a consistent strategy for handling missing dates. In some circumstances concurrency status may be determined despite missing data. For example, any respondent who reports a single partner in the last year can be classified as having no concurrency, even if dates are missing for that partner. A respondent with two partners in the last year who is missing a single date for one partner may still be classified as concurrent if the non-missing date lies in the interval defined by the other partner. If a person has reported multiple partners but there is not enough information given to definitively classify the case, we code the case as a “possible” concurrency. This allows us to define lower and upper bounds on the estimates of the prevalence of concurrency. The analysis presented here uses the lower bound estimates—only the cases that can be definitively classified as concurrent. Results for the upper bound estimates do not differ substantively (Missing data rates can be found in the supplemental web material A3).
Data Analysis
To control for differences in sample composition, we re-weight the PSI data to match the composition of the DHS weighted sample based on the full cross-tabulation of sex, 5-year age category, urban/rural residence and marital status (single, married/cohabiting, divorced/widowed/separated).
We start with simple descriptive analyses to show the magnitude and pattern of the differences between DHS and PSI surveys. We then estimate the composition-weighted country and sex-specific study effects as odds ratios (OR), using logistic regression to identify significant effects.
Results
Descriptive Results
Figure 1 presents aggregate results for the reporting of multiple partnerships broken down by sex and age (pooling across countries), and by sex and country (pooling across ages). Figure 2 presents the ratio of the PSI to DHS estimates for the two concurrency indicators, broken down by sex and by country, and sequentially adjusted for sample composition and multiple partnership reporting.
Fig. 1.
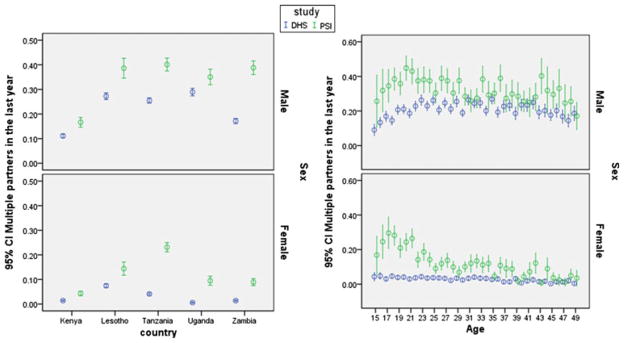
Prevalence of multiple partnerships in the last 12 months by country and age in the PSI surveys versus the DHS surveys. First panel compares the estimated prevalence (population percentage) by country for each sex. Second panel compares the prevalence by age for each sex, with the data pooled for all four countries. Cases are weighted to produce the DHS weighted sample composition by age, sex and marital status by country for both surveys
Fig. 2.
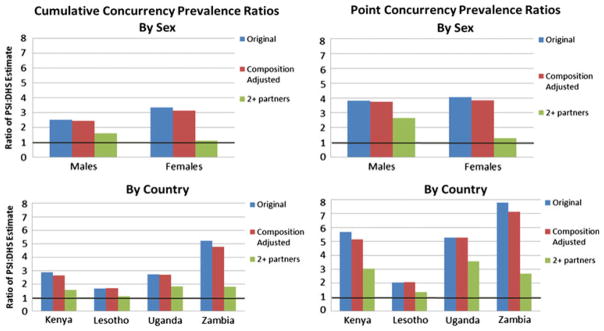
Ratios of estimated concurrency prevalence, PSI to: DHS—“Original” uses data weighted by the original sample weights for each survey, “Composition Adjusted” uses data weighted to have the same age-sex-marital status composition as the DHS samples, and “2+ partners” is restricted to persons reporting multiple partners in the last year, again using DHS sample weights. Values greater than 1 (dark black line) indicate PSI estimates are higher by the factor shown on the y-axis. The DHS underestimates of the point prevalence of concurrency are particularly severe, and the variations by sex and country are statistically significant
Multiple Partnerships
The reporting of multiple sexual partners in the last year is substantially higher in the PSI surveys than in the DHS surveys (Fig. 1). Summarizing the results in Fig. 1, after adjusting for sample composition, the average estimates are 11.4 versus 19.8 % in the DHS and PSI surveys respectively (across countries). The typical discrepancy is much larger in women’s reports, 2.8 versus 9.2 % (DHS vs. PSI), but the men’s reports also differ: 21.5 versus 32.3 % (DHS vs. PSI). The consistently higher reports of multiple partnerships found in the PSI studies is striking—ranging from 1.2 to 10.0 times higher by country and sex (for Ugandan married men and women, respectively), and higher at almost every age for both sexes, with the largest discrepancies among those under 25. The estimates shown in Fig. 1 adjust for differences in sample composition between the surveys in each country, but the compositional adjustment has little effect on the estimates: it reduces the overall discrepancy, measured as the ratio of the PSI to the DHS estimate, from 1.8 to 1.7.
Concurrency
Both of the concurrency prevalence indicators are also substantially higher in the PSI surveys, again for both sexes in all countries. Overall, the composition adjusted cumulative annual prevalence estimates are a factor of 2.6 times higher in the PSI surveys: 5.9 versus 15.1 % in the DHS and PSI respectively—and the point prevalence estimates are 3.8 times higher—2.7 versus 10.1 % respectively. Women’s cumulative prevalence estimates are 1.9 versus 6.0 % respectively, and their point prevalence estimates are 1.0 versus 3.7 % respectively. Men’s cumulative prevalence estimates are 10.6 versus 25.9 % respectively, and their point prevalence estimates are 4.7 versus 17.6 % respectively.
Prevalence estimate ratios (PSI:DHS) are broken down by country and sex in Fig. 2. Three sequential estimates are shown: first using the original data, second after adjustment for sample composition, and finally after restricting the sample to respondents who report multiple partners in the last year. Using the original sample weights, the PSI concurrency estimates are higher for both sexes (top panel), and higher in every country (bottom panel). The point prevalence estimates again show greater discrepancy, and the size of the discrepancy varies substantially by country. Adjusting for differences in sample composition has virtually no impact for either concurrency indicator, by country or by sex. The smallest differences are in Lesotho, where PSI estimates are about twice as high as DHS; the largest are in Zambia, where PSI estimates are 5–7 times higher than DHS. In the final estimates, restricted to those reporting multiple partners in the last year, the discrepancy is substantially reduced for both indicators. This indicates that the key reason for the discrepancy in the concurrency estimates is the lower rate of multiple partner disclosure in the DHS surveys, particularly among women. That said, a substantial unexplained discrepancy remains among those reporting multiple partnerships: overall, the PSI estimates of cumulative prevalence are still about 50 % higher, and the point prevalence estimates are 2.4 times higher among respondents reporting multiple partners in the last year.
Significance of Study Effects on Sexual Behavior Reporting
The size and statistical significance of the study effects on each indicator by country and sex are shown in Table 2. The table presents the OR for study (DHS is the reference category) for each sexual behavior indicator, adjusting for sample composition. Regressions are run within country and sex, for each of the sexual behavior indicators, using weights to adjust for sample composition. The ORs represent the relative odds of reporting the indicated behavior in the PSI surveys.
Table 2.
Odds ratios and statistical significance for study effect on estimates of sexual behaviors
| Full sample
|
Multiple partnered only
|
||||||||
|---|---|---|---|---|---|---|---|---|---|
| Sample Ns
|
Study effect (OR)*
|
Sample Ns
|
Study effect (OR)*
|
||||||
| DHS | PSI | Multiple partners | Cumulative concurrency | Point concurrency | DHS | PSI | Cumulative concurrency | Point concurrency | |
| Kenya | |||||||||
| Men | 2,718 | 2,216 | 1.57 | 2.70 | 6.17 | 340 | 400 | 7.17 | 9.18 |
| Women | 7,035 | 964 | 3.09 | 3.97 | 3.64 | 102 | 42 | 1.96† | 1.32†† |
| Lesotho | |||||||||
| Men | 1,968 | 471 | 1.66 | 2.01 | 2.37 | 537 | 190 | 2.03 | 2.01 |
| Women | 4,629 | 740 | 2.01 | 1.76 | 2.12 | 337 | 109 | 0.67†† | 1.13†† |
| Uganda | |||||||||
| Men | 1,232 | 891 | 1.26† | 2.79 | 5.82 | 370 | 311 | 3.99 | 7.80 |
| Women | 4,126 | 978 | 10.97 | 8.56 | 8.67 | 38 | 97 | 0.70†† | 0.78†† |
| Zambia | |||||||||
| Men | 5,099 | 1,346 | 3.07 | 5.91 | 7.48 | 909 | 535 | 8.73 | 4.62 |
| Women | 6,213 | 1,334 | 6.96 | 10.08 | 16.94 | 95 | 122 | 3.82 | 4.13 |
| Median** | |||||||||
| Men | 1.62 | 2.74 | 6.00 | 5.58 | 6.21 | ||||
| Women | 5.02 | 6.27 | 6.15 | 1.33 | 1.22 | ||||
Exp (β) for estimated study effect, all coefficients are statistically significant at p < 0.001 unless otherwise noted
Median across the four countries, within sex. Because the number of countries is even (4), the median is calculated as is the average of the middle two estimates
p <0.05
p > 0.05
The first set of columns shows results for the full sample. All of the ORs, for both sexes in every country, for all three indicators, are above 1, indicating uniformly higher rates of reporting in the PSI surveys. In general, the magnitude of the study effect increases as we move across the columns from multiple partner reporting to concurrency for both men and women. The effects are also highly significant: all but one is statistically significant at p < 0.001, and the exception is significant at p < 0.005.
The second set of columns shows results for the sample restricted to persons reporting multiple partners in the last 12 months. The resulting sample Ns are much smaller here, especially for women. All of the study effects for the women’s estimates have declined, and some have fallen below 1 (these are not significant). With the exception of Zambia, for women, the lower reports of multiple partners in the DHS appear to explain the lower reports of concurrency for women. By contrast, the effect sizes for men rise in six of the eight cases, and all remain statistically significant. The lower estimates of concurrency in the DHS for men cannot be explained solely by the lower reporting of multiple sexual partnerships.
Discussion
This study compared DHS estimates of multiple partnerships and concurrency in four different countries in sub-Saharan Africa where both the DHS and PSI conducted comparable nationally representative surveys of sexual behavior within the same time frame. The DHS studies consistently produce significantly lower estimates of multiple partnerships and concurrency than the PSI studies. This is true for both sexes, for every country compared, and for all three behavior indicators.
Overall, the fraction of the population reporting multiple partners was almost twice as high in the PSI studies than the DHS, the cumulative annual prevalence of concurrency was 2.6 times higher, and the point prevalence of concurrency was 3.8 times higher. For women, the discrepancies were 3.2, 3.1 and 3.8 times higher respectively, and for men 1.5 and 2.6 and 3.7 times higher respectively. Differences in sample composition explain less than 10 % of this overall discrepancy. The ORs for the composition-adjusted study effects remain highly significant within country and sex. Disclosure of multiple partners appears to explain almost all of the discrepancy for women, but little of the discrepancy for men, despite the fact that men are also less likely to disclose multiple partners in the DHS surveys.
It is clear that the DHS surveys obtain lower rates of reporting of multiple and concurrent partners. Explaining why this is the case is beyond the scope of this paper, but some points can be noted here. They fall into two categories: sample differences, and differences in interview procedures.
Both surveys use the same sample frames—enumeration areas defined by national statistical agencies—and a 2-stage cluster design. The DHS procedures, however, result in a non-self-weighting sample, and the sample weights they provide also adjust for non-response (assuming missing at random), while the PSI data have no sample weights (except for Kenya, which has stratification weights only). This could lead to differences in sample composition. We matched sample eligibility criteria within country, and adjusted for key demographic differences by weighting to obtain equal distributions for the full cross-tabulation of sex, 5-year age group, marital status, and urban residence (the marginal differences can be seen in Table 1). Note that we adjusted to match the DHS weighted sample composition, so this also accounts for differential response rates by these attributes. The adjustment had very little impact on the discrepancies, however. We also compared the detailed geographic distributions across surveys within countries, and found them to be very similar (data not shown). If there are residual differences in sample composition, they must be uncorrelated with the variables for which we have adjusted.
Both surveys use face-to-face interviewing for the sexual behavior questions, so the results are not induced by differences in the mode of administration. It is worth emphasizing that the PSI surveys get consistently higher rates of reporting of these sensitive behaviors, even among women, with face-to-face interviews. It is possible that still higher rates would be reported using self-administered techniques. A small validation study conducted by PSI in Kenya that used self-administered “ballot box” methods did obtain higher rates of disclosure, especially among women. In a systematic analysis of sexual behavior reporting across studies in the United States, however, face-to-face interviews did not produce lower estimates than self-administered surveys [11]. In any case, the differences between the DHS and PSI findings shows there is clearly a wide range of reporting that can be elicited using face-to-face interviewing.
One difference between the questionnaires is that the PSI question wording for eliciting the number of partners in the last year included phrasing to remind the respondent to include marital or cohabiting partners in their total. That may have played a role in the higher numbers of partners reported. It may be worth adding a reminder of this sort to ensure fuller disclosure.
Another difference between the PSI and DHS surveys is length: the PSI HIV TRaC studies focus almost exclusively on HIV related knowledge, attitudes, and behavior. By contrast, the general purpose nature of the DHS makes it a long survey to administer, with many repetitive segments triggered by multiple births, deaths, contraceptive choices and sexual partnerships. A typical DHS questionnaire has 10 sections with over 4,000 pieces of information collected. The DHS–AIS, while more restricted in scope, are equally long. This leads to well-known quality issues like “birth-displacement” that arise when interviewers (or respondents) seek to reduce the length of time they spend on an interview by intentional misreporting. A recent estimate suggests that this may bias total fertility rate underestimates downward by about 10 % [12]. That is regarded as an alarmingly high level of error by demographers, but it is a small fraction of the underestimates that we observe by comparison for sexual behaviors (90–500 %) (Table 2). It is possible that the sensitive nature of the sexual behavior questions makes them more vulnerable to displacement, for both interviewer and respondent.
The sensitive nature of the questions also may make sexual behavior data more difficult to collect specifically in the context of the DHS. While the DHS is one of the few surveys that has always addressed aspects of sexual behavior, it was traditionally framed in the context of fertility and family planning. Children, in contrast to multiple sexual partners, are generally regarded as a good thing. Once a study has been framed in terms of maternal and child health, it may be more difficult to address more stigmatized aspects of sexual behavior involving multiple partners. This could influence study results directly and indirectly, from interviewer recruitment and training, to the rapport established at the time of interview.
Two other procedural differences are worth noting, both involving privacy. The DHS surveys enumerate all household members, with names, and interview all adult members of a household, while the PSI enumerates but only interviews one adult member. The DHS procedures may reduce disclosure of sensitive information. DHS interviewers are strongly encouraged to conduct interviews in locations that ensure privacy for the respondent, however this is not always possible. The DHS datasets include indicators for the presence of other persons, and whether they were listening, but only for the women’s interviews. Overall, 9.7 % of the women’s interviews in the DHS studies used here show another person present during the time of interview, and just over 1.1 % show this person listening. This varies by country, from a low of 0 % in Lesotho, to a high of 26.5 % present and 4.2 % listening in Uganda. PSI guidelines also make interviewing in private a priority, especially for the TraC surveys that focus on sexual behavior. There is, however, no indicator in their surveys that records whether someone else is present. While it is likely that lack of privacy would lower rates of reporting among women in the DHS, it seems unlikely that this can explain the large discrepancy between the surveys. For this to be true, there would have to be a strong positive correlation between the presence of others and the probability that a woman has multiple partners—in the absence of this correlation, lack of privacy would affect interviews at random, inducing a difference more like the rate of others present, so a maximum of 26.5 %, not the 90–500 % we observed.
Further research is clearly needed to identify the reasons for lower rates of sexual partner disclosure in the DHS, and the options for improving the validity of these data. Until then, care should be taken when using these data. The under-reporting of multiple and concurrent partnerships in the DHS will contaminate both empirical analyses of the link between sexual behavior and HIV infection, and theoretical models for combination prevention packages that use these data for inputs. In particular, such models would underestimate the true impact of a behavioral intervention in reducing HIV infection, which would affect allocations of resources for HIV programming. In addition, because the magnitude of the underestimates vary by country, the DHS data should not be used for cross-country comparisons of multiple and concurrent partnerships, as any observed differences may be confounded with differences in reporting. This may have implications for already published findings that use DHS data, including a paper that found protective effects of polygyny [13] (that controlled for multiple partnerships), a model-based study that estimated 55–90 % of HIV incidence occurs within cohabiting discordant couples (these estimates rely on the reported prevalence of extra-cohabiting partners), [14] and a recent multi-level analysis of the determinants of HIV across the sub-Saharan African region [15].
The silver lining in this cloud is that the PSI studies demonstrate it is possible, using traditional survey interviewing techniques, to obtain substantially higher reporting of multiple and concurrent partners from both men and women. These include reduction of the survey length to avoid respondent’s fatigue, ensuring privacy and confidentiality for respondents, and the inclusion of probing reminders or transition statements to help participants follow the flow and changes in topics in the survey. The PSI survey data may still underestimate the true prevalence of multiple and concurrent partnerships, and the collection of self-reported sexual behavior data will, in all likelihood, remain an endeavor fraught with uncertainty. But the results of this analysis suggest that improvements are possible.
Supplementary Material
Acknowledgments
We would like to thank Measure DHS for generously sharing the data. Our special thanks go to these particular PSI researchers and to all who have contributed significantly to the study designs and data collection: Amy Kate Herman-Roloff; Noah Taruberekera; Lipolelo Mokhesi; Peter Buyungo; Nicholas Shiliya; Felton Mpasela; and Edna Ogada.
Footnotes
Electronic supplementary material The online version of this article (doi:10.1007/s10461-013-0618-6) contains supplementary material, which is available to authorized users.
Contributor Information
Martina Morris, Email: morrism@u.washington.edu, Department of Statistics, University of Washington, Box 354322, Seattle, WA 98195, USA.
Lung Vu, Email: lung.vu@gmail.com, Population Services International – Washington DC, 1120 19th Street, NW, Suite 600, Washington, DC 20036, USA.
Ayn Leslie-Cook, Department of Statistics, University of Washington, Box 354322, Seattle, WA 98195, USA.
Eniko Akom, Population Services International – Washington DC, 1120 19th Street, NW, Suite 600, Washington, DC 20036, USA.
Aloo Stephen, Population Services International – Kenya, 2nd Floor, Wing B, Jumuia Place, Lenana Road, Box 22591-00400, Nairobi, Kenya.
Donna Sherard, Population Services International – Washington DC, 1120 19th Street, NW, Suite 600, Washington, DC 20036, USA.
References
- 1.Eaton JW, Hallett TB, Garnett GP. Concurrent sexual partnerships and primary HIV infection: a critical interaction. AIDS Behav. 2010;15(4):687–92. doi: 10.1007/s10461-010-9787-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Goodreau SM, Cassels S, Kasprzyk D, Montano DE, Greek A, Morris M. Concurrent partnerships, acute infection and HIV epidemic dynamics among young adults in Zimbabwe. AIDS Behav. 2012;16(2):312–22. doi: 10.1007/s10461-010-9858-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Powers KA, Ghani AC, Miller WC, et al. The role of acute and early HIV infection in the spread of HIV and implications for transmission prevention strategies in Lilongwe, Malawi: a modelling study. Lancet. 2011;378(9787):256–68. doi: 10.1016/S0140-6736(11)60842-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Demographic and health surveys. 2012 http://www.measuredhs.com/publications/publication-FR194-DHS-Final-Reports.cfm.
- 5.Morris M, Epstein H, Wawer M. Timing is everything: international variations in historical sexual partnership concurrency and HIV prevalence. PLoS ONE. 2010;5(11):e14092. doi: 10.1371/journal.pone.0014092. 14010.11371/journal.pone.0014092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Central Statistical Office (CSO), Ministry of Health (MOH), Tropical Diseases Research Centre (TDRC), University of Zambia, Inc. MI. Zambia demographic and health survey 2007. Calverton, MD, USA: CSO and Macro International Inc; 2009. [Google Scholar]
- 7.Kenya National Bureau of Statistics, ICF Macro. 2008–09 Kenya demographic and health survey. Calverton, MD, USA: KNBS and ICF Macro; 2010. [Google Scholar]
- 8.Ministry of Health and Social Welfare (MOHSW) [Lesotho], ICF Macro. Lesotho Demographic and Health Survey 2009. Maseru, Lesotho: MOHSW and ICF Macro; 2010. [Google Scholar]
- 9.Uganda Bureau of Statistics (UBOS), Macro International Inc. Uganda Demographic and Health Survey 2006. Calverton, MD, USA: UBOS and Macro International Inc; 2007. [Google Scholar]
- 10.UNAIDS Reference Group on Measurement and Modeling. HIV: consensus indicators are needed for concurrency. Lancet. 2010;375(9715):621–2. doi: 10.1016/S0140-6736(09)62040-7. [DOI] [PubMed] [Google Scholar]
- 11.Hamilton D, Morris M. Consistency of self-reported sexual behavior in surveys. Arch Sex Behav. 2010;39(4):842–60. doi: 10.1007/s10508-009-9505-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Schoumaker B. Omissions of births in DHS birth histories in sub-Saharan Africa: measurement and determinants. Population Association of America; Washington, DC: 2011. [Google Scholar]
- 13.Reniers G, Watkins S. Polygyny and the spread of HIV in sub-Saharan Africa: a case of benign concurrency. Aids. 2010;24(2):299–307. doi: 10.1097/QAD.0b013e328333af03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dunkle KL, Stephenson R, Karita E, et al. New heterosexually transmitted HIV infections in married or cohabiting couples in urban Zambia and Rwanda: an analysis of survey and clinical data. Lancet. 2008;371(9631):2183–91. doi: 10.1016/S0140-6736(08)60953-8. [DOI] [PubMed] [Google Scholar]
- 15.Magadi M, Desta M. A multilevel analysis of the determinants and cross-national variations of HIV seropositivity in sub-Saharan Africa: evidence from the DHS. Health Place. 2011;17(5):1067–83. doi: 10.1016/j.healthplace.2011.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.