

Abstract
Background:
A good body balance requires a proper function of vestibular, visual, and somatosensory systems which can be reach with exercise practice and/or yoga.
Aim:
To determine the effects of a 5-month hatha yoga training program on body balance in young adults.
Materials and Methods:
This study used a controlled, nonrandomized design, where the experimental group underwent a 5-month training program and were then compared with the control group that had a sedentary lifestyle. A convenience sample of 34 out of 40 men aged 25-55 years old (34.0 ± 0.9) were deemed eligible for this study. They were randomly divided into two groups: Experimental and control groups. Subjects in the experimental group were engaged in 60 min sessions of hatha yoga three times a week for 5 months. We evaluated postural control by measuring the limit of stability and velocity of oscillation (VOS) in three conditions of the balance rehabilitation unit (BRU) and through field procedures (four position, plane, flamingo, hopscotch, and dynamic test).
Results:
We observed differences (P < 0.05) in postintervention scores between the groups regardless of BRU parameters and field procedures (except for flamingo) even after adjusting for preintervention scores, suggesting that these changes were induced by hatha yoga training. The partial eta squared on BRU parameters ranged from 0.78 (VOS1)-0.97 (COP2), and from 0.00 (flamingo)-0.94 (four position) for the field procedures.
Conclusions:
Our results provide substantial evidence that postural control in healthy young adults can be improved through practicing hatha yoga.
Keywords: Adults, balance, health, posture, yoga
INTRODUCTION
Body balance, whose goal is to stabilize the body against the law of gravity in both the upright position and during movement, is an important function for human beings.[1] The effectiveness of body balance requires the activities and proper functioning of the vestibular, visual, somatosensory, muscular, and central nervous systems.[2,3]
Physical exercises have been commonly used to improve body balance by employing individual protocols that use resistance exercises such as dynamic and static training or by applying exercises that facilitate adaptation (adjustment of sensory information due to new operating conditions) or habituation (modulation in the vestibular nuclei) to balance disturbances, thus lessening their effects on the body.[4,5,6]
Yoga, which requires individuals to practice self-control and be aware of their limits and potentials through the maintenance of their postures (asanas), could improve physical and emotional balance.[7,8] Yoga, which originated in India, is a set of techniques that have existed for more than 3000 years and has been a part of Indian medicine. Orientals believed that it affects nervous energy and the activities in the endocrine, cardiac, pulmonary, muscular, and nervous systems through stimulation and facilitates physical, emotional, and spiritual recovery.[8] Yoga seeks to unify the mind and body through self-recognition and emotional and physical realizations of the asanas; its principal features of maintaining control and comfort provide targets or patterns of implementation to help practitioners adopt a calmer and healthier lifestyle.[7,8]
Yoga is focused on physical and mental aspects where practitioners evolve in their own time.[7] Practitioners are instructed to maintain the asanas while focusing on stability, comfort, and breathing (pranayama) while aiming for self-control and body awareness.[8,9] These techniques enhance physiological responses, such as emotional balance and body harmony, in motion; they also enhance strength and flexibility, which are factors that induce important influence in the activities of daily living, and substantially improve dynamic postural control in individuals over the age of 60.[9,10]
Therefore, due to its low impact movements, yoga is a potential treatment for patients suffering from balance disorders, such as those involving the vestibular, muscular, and neurological systems. There is no study about the influence of yoga in body balance in patients and healthy individuals. This study, therefore, attempted to investigate the influence of regular hatha yoga practice on the control and maintenance of body balance in healthy adults.
MATERIALS AND METHODS
Experimental design
This nonrandomized, controlled study involved an intervention consisting of 60 hatha yoga sessions held thrice a week for 5 months, with each session lasting 60 min. Primary outcome was determined by measuring limit of stability (LOS), center of body pressure area (COP), and velocity of sway (VOS) in three visual, vestibular, and somatosensory conditions of static balance in the balance rehabilitation unit (BRU). The secondary outcome was determined through performance analysis and field tests such as the four position, plane, flamingo, hopscotch, and dynamic tests. Outcome measures were assessed before and immediately after the program in both the experimental and control (sedentary) groups.
Volunteers
A convenience sample of male volunteers aged 25-55 years (34.0 ± 0.9) was recruited from the police academy. They were informed about the procedures and risks before seeking a written informed consent. This study was approved by the research ethics committee of our university. A preliminary screening that focused on current health status, drug and cigarette use, and habitual physical activity was followed by an ambulatory visit to obtain a detailed history of past and current health status and physical examination. Volunteers who presented with the following were excluded: (1) Dizziness, vertigo, imbalance, or recurrent falls; (2) severe impairments in visual and auditory acuity even with corrective lenses or hearing aids; (3) orthopedic disorders resulting in movement limitations; (4) prosthetic lower limbs; (5) limited muscular strength of a member that would affect the performance of the activity or simultaneous performance of more than one physical activity; or (6) use of anabolic steroids or illegal drugs or a history of alcohol abuse.
Out of 40 volunteers, 34 met the criteria for participation and reported willingness to be assigned to either treatment condition (experimental [N = 17] or control [N = 17]).
Yoga
Eligible individuals (n = 17) already practicing yoga for at least 3 months, two time per week, to verify if continuing the practice for 5 more months would further improve body balance. The intervention consisted of 60 hatha yoga sessions held three times a week for 5 months, with each session lasting 60 min. The exercises were based on stretching postures (asanas), breath control techniques (pranayama), meditation techniques (dhyrana), relaxation techniques (nidra), and techniques of muscle or organ contractions and concentration (bandha).[11] All sessions were conducted by an experienced hatha yoga instructor. Subjects were instructed not to increase their spontaneous daily activities or to join any other exercise program throughout the study period.
The subjects in the control group (n = 17) did not perform any physical exercise during this period and showed no morbidity or decline in balance; those who did were excluded from the study.
Body balance
Balance rehabilitation unit (BRU®, Medicaa™, Montevideo, Uruguay)
The BRU is the gold standard measure for the LOS, COP, and VOS. The area of the ellipse corresponding to an area distribution of 95% of the sample is determined by the average total distance of body oscillation at a particular position and stimulation in 60 s.[12,13] The LOS evaluates how a person moves his base of support without experiencing instability or falling. Volunteers were instructed to move the body anteroposteriorly and laterally such that they could maintain a static position without falling. A high LOS indicates good stability, while low COP and VOS imply good balance control.[13] The following conditions of sensory conflict (visual, vestibular, and somatosensory) were selected: (1) Standing on firm ground, eyes open (basal position with no conflict); (2) standing on firm ground, eyes closed (blindfolded; to evaluate vestibular and somatosensory system activity without visual input); and (3) standing on a foam pad, eyes closed (visual and somatosensory conflict to assess the vestibular system). Movements of the upper limbs, ankles, or feet were prohibited for 60 s in all the conditions and only one attempt was allowed for each condition. The condition in which the COP and VOS is tested is indicated by its number (i.e., COP of condition 2: COP2).
Field procedures
We also applied some practical tests conducted in plane areas without any special equipment except a clock counter to determine body balance. Volunteers were instructed to perform each task for as long as possible (except for dynamic balance) and the result attained in a unique trial was used in the analysis. The procedures consisted of the “four position,” “plane,” “flamingo,” and “hopscotch” tests. The four position entailed standing barefoot with one foot up and resting on the knee of the leg that is supporting the weight of the body. Plane involves standing barefoot with one leg supporting the body and the other extended parallel to the ground. The torso should be bent parallel to the ground below the axis of the leg and accompanied by extension of the thigh-femoral, and upper limbs should be abducted horizontally by 90° with respect to the trunk and neck extension, mimicking an airplane. Flamingo tests the ability to stay on a wooden beam while standing barefoot, with one foot resting on the longitudinal axis of the beam and the knee of the other leg flexed and the foot up to the buttocks. This mimics the posture of a flamingo and is maintained with the aid of the hand on the same side, while the other arm could be used for balance. For these tests, it was offered only one attempt and the time counted (in seconds) was a period remained in this position, keeping in stable balance. In hopscotch, the volunteers had to skip back and forth on one foot without switching and without losing their balance (touch the ground with the foot or any other body part). The time taken in seconds to make the journey back and forth without losing balance was measured.
Dynamic test assessed the ability to jump and maintain equilibrium during and after the movement. Volunteers assumed standing positions and wore sports shoes with their right legs on the tag output. They then had to jump to the first mark and land on their left legs on tiptoe and remain in this position as long as possible or for a maximum of 5 s) before jumping to the second mark to the right and landing on the right leg on tiptoe, and so on. The tip of the foot should completely cover the marks placed on the floor. Reaching each mark awarded volunteers with five points, with the addition of one point for every second that remained balanced on each brand. If they lost their balance, volunteers returned to the mark. The seconds were counted aloud. The results of the landing and balance were recorded at each mark. The maximum score for each mark was 10 points, with a total of 100 points for the entire test. Volunteers lost five points when they (1) failed to reach the mark landing, (2) touched the ground with any part of body except their toe while in position, (3) failed to carry out the jump, or (4) moved their foot while in position. Volunteers who committed penalties had 5 s to compose themselves.
Statistical analysis
Using the Minitab statistical power (power and sample size), we calculated descriptive statistics of mean and standard deviation of the limit of stability for the total sample. The onset and final results were considered. The sample size was determined using a magnitude of effect corresponding to 1.4 times the range of 95%, resulting in β =0.785 and P < .05 (Jandel Scientific, CA, USA). The potential effect was based on a training-induced magnitude of 40%. Thus, a sample size of 30 individuals divided into two groups was deemed to have suitable statistical power. A one-sample Kolmogorov-Smirnov test demonstrated the normality of data distribution for all measured variables. A one-way between-groups analysis of covariance was conducted to compare the effectiveness of intervention. The results of the preintervention period were used as a strategy (i.e., covariate) for avoiding that any training-induced effect was due to baseline differences between both groups. Age and body mass were also covariated due to the fact that these variables are commonly intervenient factors for exercise performance. In addition, partial eta squared was calculated to determine the effect size of within-subjects effects. Statistical significance was set at P <.05. All analyses were performed with Predictive Analytics Software for Windows (PASW, version 19.0, Inc., Chicago, IL, USA).
RESULTS
Participant characteristics
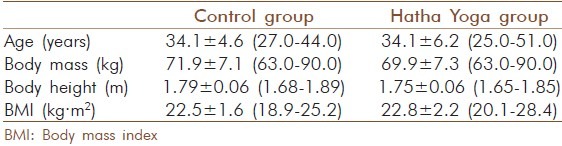
Both the control and experimental groups were matched for age, height, and body composition [Table 1].
Table 1.
Participant characteristics
Between-subjects analysis
There were differences between the groups in COP2 and COP3 when BRU parameters in the pre-intervention assessment were analyzed [Table 2]. Volunteers who went through the hatha yoga program had better performances in the field procedures [Table 3]. We also observed differences (P < 0.05) between groups of BRU parameters [Table 2] and field procedures (except for flamingo [Table 3]) in the postintervention scores even after adjusting for preintervention scores. In general, the partial eta squared ranged from 0.13 (hopscotch [Table 3])–0.90 for the VOS of condition 3 (VOS3) [Table 2].
Table 2.
Effect of hatha yoga on balance rehabilitation unit parameters
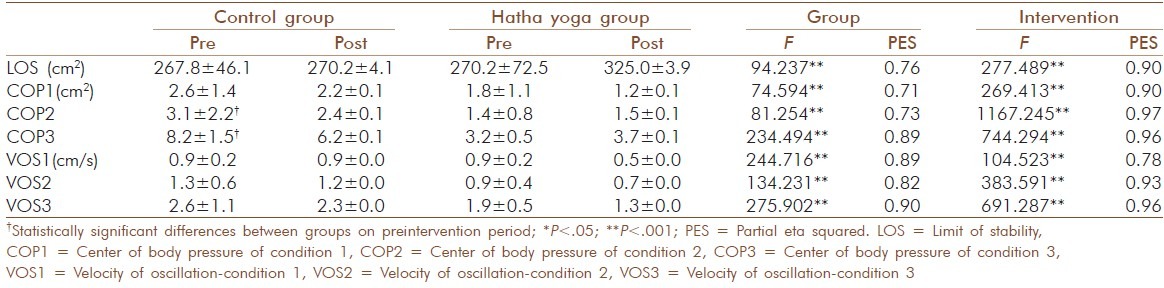
Table 3.
Effect of hatha yoga on balance measured through field procedures

Effects of hatha yoga
Analyses of body balance measured by BRU parameters [Table 2] and field procedures [Table 3] revealed key effects due to hatha yoga training. The partial eta squared on BRU parameters ranged from 0.78 (VOS1)–0.97 (COP2), and from 0.00 (flamingo)–0.94 (four position) for the field procedures. We also observed a strong effect induced by hatha yoga training, as indicated by the obtained partial eta squared.
DISCUSSION
Our results provide substantial evidence that postural control in young adults can be improved through the practice of hatha yoga. They also support the idea that measurements low in operating costs and high in convenience such as field procedures are comparable to more expensive tests such as the BRU in measuring postural control; this could be corroborated by some results of our group demonstrating that the predictive power of field tests varied from 48%-97% depending on the area of the BRU to which they are compared against (data not shown), suggesting a similar sensitivity for detecting the magnitude of the effects induced by training in both strategies (i.e., BRU and field procedures [except for Flamingo]).
Our obtained effect sizes demonstrated that a significant proportion of the variance in the dependent variables was explained by the independent variable; we were able to explain about 90% (four position) and 96% (COP3 and VOS3) of those variances, respectively [Tables 2 and 3] even after controlling for the independent variable. This indicated that our covariates explained the variance in the dependent variables. The effect size of intervention was higher when compared with the effect size of group, suggesting an important hatha yoga-induced effect, mainly for field procedures [Tables 2 and 3].
As the experimental and control groups had similar general characteristics, we were able to confirm that these characteristics do not influence body balance; although the yoga group performed better than the sedentary group in some tests of static posturography (COP and VOS) initially, their postural control was found to have improved further after intervention, providing additional evidence that support the positive effect of yoga on postural control.
LOS and COP1 did not differ between groups, similar to the tests where volunteers remained static without visual and vestibular conflicts. The second condition checks the integrity of the vestibular and somatosensory and the third condition is the most difficult and sensitive test to be carried out, in which the vestibular system is tested. In both conditions, the performance of the hatha yoga group, as measured by the COP and VOS, was better after physical exercise. In baseline, only COP2 and COP3 were different from the control group.
The field procedures showed that the pre- and postintervention performance of the hatha yoga group was significantly better compared with the control group. This is particularly true for the flamingo test, which is considered the most difficult test used in our study because a high level of concentration is needed to maintain the required position. Somatosensory conflict is higher in this test than for the other tests because the individual must remain balanced on a lower support surface (lock) in a static one-leg position, requiring greater postural control from the vestibular system. This corresponds with the results of the third condition of static posturography (unstable), which had the most conflict between systems.
Information concerning the positioning of the body segments is provided by the sensory systems, with the motor systems being responsible for proper muscle activation when performing the movements. This supports the idea that one needs to be physically prepared for the implementation of tasks that require fine motor control (e.g., dynamic balance) in terms of concentrating energy sources and optimizing the muscle groups involved. This optimization is emphasized in yoga, which focuses on employing the muscles necessary to perform the task with minimal effort.
Moreover, it has been reported that yoga practitioners train their balance in situations, where somatosensory stimuli are constantly required during the asana positions because many of the exercises are performed with the eyes closed, thus requiring the participation of the vestibular system. This corroborates with the principle of training specificity, where specific movements and motor coordination are needed to improve postural balance.
Many exercises in hatha yoga improve balance by inducing somatosensory and vestibular conflicts. The better outcomes of the hatha yoga group in conditions 2 and 3 of the posturography and the flamingo and dynamic tests have supported this.
Our study also supports the possibility of using hatha yoga on patients with vestibular disorders with or after vestibular rehabilitation. Hatha yoga-induced several conflict in the visual, vestibular, and somatosensory systems that are important mechanisms for maintain these systems working well. This is the central element used for balance retraining or vestibular rehabilitation in patients with vestibular disorders (exercises consisting of eye, head, and body movements).[14]
No study has investigated the use of yoga to help patients with vestibular and balance disorders or fall risk, but tai chi has been used with some success in people with these conditions and risk of falling.[15,16] Future studies should examine this possibility.
CONCLUSIONS
The results of static posturography and field procedures indicated that hatha yoga training improves body balance.
ACKNOWLEDGMENTS
We thank Wagner Oliveira do Espirito Santo, from the Physical Education School of Police of Sγo Paulo (EEF/PMESP), for providing assistance in data collection. We would also like to thank Editage for providing editorial assistance.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Horak FB, Macpherson JM. Handybook of Physiology. New York: Oxford; 1996. Postural orientation and equilibrium. Exercise: Regulation and integration of systems multiple; pp. 255–8. [Google Scholar]
- 2.Horlings CG, Carpenter MG, Honegger F, Allum JH. Vestibular and proprioceptive contributions to human balance corrections. Ann N Y Acad Sci. 2009;1164:1–12. doi: 10.1111/j.1749-6632.2009.03872.x. [DOI] [PubMed] [Google Scholar]
- 3.McCollum G, Shupert CL, Nashner LM. Organizing sensory information for postural control in altered sensory environments. J Ther Biol. 1996;3:257–70. doi: 10.1006/jtbi.1996.0101. [DOI] [PubMed] [Google Scholar]
- 4.Hayes KC. Biomechanics of postural control. Exerc Sport Sci Rev. 1982;10:363–91. doi: 10.1249/00003677-198201000-00011. [DOI] [PubMed] [Google Scholar]
- 5.Horak FB. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing. 2006;5:ii7–11. doi: 10.1093/ageing/afl077. [DOI] [PubMed] [Google Scholar]
- 6.Lubetzky-Vilnai A, Kartin D. The effect of balance training on balance performance in individuals poststroke: A systematic review. J Neurol Phys Ther. 2010;34:127–37. doi: 10.1097/NPT.0b013e3181ef764d. [DOI] [PubMed] [Google Scholar]
- 7.Raub JA. Psychophysiologic effects of hatha yoga on musculoskeletal and cardiopulmonary function: A literature review. J Altern Complement Med. 2002;8:797–812. doi: 10.1089/10755530260511810. [DOI] [PubMed] [Google Scholar]
- 8.Woodyard C. Exploring the therapeutic effects of yoga and its ability to increase quality of life. Int J Yoga. 2011;4:49–54. doi: 10.4103/0973-6131.85485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gauchard GC, Jeandel C, Tessier A, Perrin PP. Beneficial effect of proprioceptive physical activities on balance control in eldery5 human subjects. Neurosci Lett. 1999;273:81–4. doi: 10.1016/s0304-3940(99)00615-1. [DOI] [PubMed] [Google Scholar]
- 10.Oken BS, Zajdel D, Kishiyama S, Flegal K, Dehen C, Hass M, et al. Randomized, controlled, six-month trial of yoga in healthy seniors: Effects on cognition and quality of life. Altern Ther Health Med. 2006;12:40–7. [PMC free article] [PubMed] [Google Scholar]
- 11.Ramos-Jimenez A, Hernandez-Torres RP, Wall-Medrano A, Torres-Duran PV, Juarez-Oropeza MA. Cardiovascular and metabolic effects of intensive Hatha yoga training in middle-aged women from northen Mexico. Int J Yoga. 2009;2:49–54. doi: 10.4103/0973-6131.60044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gazzola JM, Doná F, Ganança MM, Suarez H, Ganança FF, Caovilla HH. Realidade virtual na avaliação e reabilitação dos distúrbios vestibulares. Acta ORL. 2009;27:22–7. [Google Scholar]
- 13.Suarez H, Arocena M, Geisinger D, Suarez A, Carrera M. Analysis of the role of virtual reality technology in the assessment and rehabilitation of instability in the elderly population. In: Vincent ML, Moreau TM, editors. Accidental Falls: Causes, Preventions and Interventions. New York: Nova Science Publishers Inc; 2008. pp. 1–14. [Google Scholar]
- 14.Yardley L, Beech S, Zander L, Evans T, Weinman J. A randomized controlled trial of exercise therapy for dizziness and vertigo in primary care. Br J Gen Pract. 1998;48:1136–40. [PMC free article] [PubMed] [Google Scholar]
- 15.McGibbon CA, Krebs DE, Parker SW, Scarborough DM, Wayne PM, Wolf SL. Tai chi and vestibular rehabilitation improve vestibulopathic gait via different neuromuscular mechanisms: Preliminary report. BMC Neurol. 2005;5:3. doi: 10.1186/1471-2377-5-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wayne PM, Krebs DE, Wolf SL, Gill-Body KM, Scarborough DM, McGibbon CA, et al. Can Tai Chi improve vestibulophatic postural control? Arch Phys Med Rehabil. 2004;85:142–52. doi: 10.1016/s0003-9993(03)00652-x. [DOI] [PubMed] [Google Scholar]