

Abstract
Introduction:
This study planned to compare immediate cardiovascular effects of different yoga asanas in healthy young volunteers.
Materials and Methods:
Heart rate (HR), systolic pressure (SP), and diastolic pressure (DP), blood pressure (BP), were recorded using the non invasive blood pressure (NIBP) apparatus in 22 healthy young subjects, before and after the performance of Dhanurasana (DA), Vakrasana (VA) (both sides), Janusirasasana (JSA) (both sides), Matsyasana and Shavasana for 30 s. HR and BP were further recorded during supine recovery at 2, 4, 6, 8, and 10 min. A repeated measure of ANOVA was used for statistical analysis.
Results:
There were significant changes in HR and BP both immediately after the Asanas as well as during the recovery period. Overall comparisons of ∆% changes immediately after the performance of the Asanas revealed significant differences with regard to HR that increased significantly after DA. In the recovery phase, there were significant intergroup differences from 2 min onward in both SP and DP. The decrease of SP after VA (right side) (VA-R) was significantly greater than Shavasana (4th, 6th, and 8th min) and JSA (left side) (JSA-L) at 6th and 8th min. DP decreased significantly after performing JSA-L compared to VA-R at the 6th and 8th min.
Discussion:
The cardiovascular changes immediately after the Asanas and during the recovery phase reveal inherent differences between the selected postures. The rise of HR in DA may be attributed to increased sympathetic response due to the relative difficulty of the posture as well as abdominal compression occurring in it. The effect of supine relaxation is more pronounced after the performance of the Asanas as compared to mere relaxation in Shavasana. This may be attributed to a normalization and resultant homeostatic effect occurring due to a greater, healthier de-activation of the autonomic nervous system occurring towing to the presence of prior activation. There were also subtle differences between the right sided and left sided performance of VA and JSA that may be occurring due to the different internal structures being either compressed or relaxed on either side.
Conclusion:
Our study provides initial evidence of differential cardiovascular effects of Asanas and subtle differences between right and left sided performance. Further, cardiovascular recovery is greater after the performance of the Asanas as compared to shavasan; thus, implying a better response when effort precedes relaxation.
Keywords: Asana, cardiovascular effects, research, Yoga
INTRODUCTION
Yoga has truly captured the imagination of scientists in recent times with a dramatic increase in the number of studies documenting various facets of this art and science.[1,2,3,4]However, though many studies have elucidated applied aspects of Yoga in different health conditions, very few have focused on the basic research needed to understand the intricate mind-body mechanisms involved in the different yogic techniques.[5]
The different Yogic psychophysiological techniques are bound to have different effects on each and every cell of the human body and this in turn will depend on the various body systems, organs, and tissues involved in the performance of such practices.[6]As the role of the spinal column is emphasized in Yoga, it follows logically that the effects of forward bending postures would be different than those of back bending ones and that these in turn may be different from the physiological effects of twisting postures. As both intra thoracic and intra-abdominal pressure-volume changes affect the cardiovascular system, it is plausible that these Asanas will produce changes in the heart rate (HR) and blood pressure (BP). The conscious self-effort made in Asana practice may be understood as the Spanda (tension) component whereas the relaxation of effort (Prayatna shaithilya) may be understood as the Nishpanda (relaxation) component. Even Maharishi Patanjali tells us that the pair of opposites (Dwandwa) is transcended (Dwandanabigata) when one perfects the state of Asana. Hence, it is essential to physiologically evaluate not only the actual performance of an Asana, but also the period of recovery following it.
However, there is a lacuna of studies on such effects and there is only one study[7]comparing cardiovascular effects of some Asanas and that too was carried out in untrained subjects with only a single recording without pre-post comparisons. That study had evaluated only the BP during the performance of Sukhasana, Vajrasana, and Dhanurasana (DA) by 25 medical students and compared these findings with the supine, sitting, and standing positions. As a pre-post comparison was lacking in that study, no concrete conclusion could be inferred about the actual effects of performing Asanas or about the recovery following their performance.
The Swara Yoga tradition[8]also emphasizes the subtle differences existing between energy flows on the right and left sides (Pingala and Ida nadi respectively) manifesting through the ultradian rhythmicity of right or left nostril dominance (Surya and Chandra Swara respectively). Autonomic function is affected by right-left brain activity[9,10]and as there is a sensory-motor crossover relationship between right and left sides of the body and the contralateral hemispheres, this leads to speculation to differences in autonomic function depending on techniques performed utilizing either right/left sides.
With the above rational in mind, this study was planned to compare the immediate cardiovascular effects of different Yoga Asanas in healthy young volunteers. In addition to studying the immediate effect of the Asanas, we also studied the post posture supine recovery period for ten min. Hence, Shavasana also served as a control to the supine rest being carried out after the performance of the other Asanas.
MATERIALS AND METHODS
This study was conducted at the Center for Yoga Therapy Education and Research (CYTER) functioning in Mahatma Gandhi Medical College and Research Institute, Puducherry, India. Ethical clearance was obtained from the Institutional Human Ethics Committee and 22 students (16 female, 6 male), aged 19.05 ± 0.79 standard deviation (SD) years, with body mass index of 20.54 ± 3.15 (SD) undergoing the B Sc., Nursing course at Kasthurba Gandhi Nursing College, Sri Balaji Vidyapeeth, Puducherry were recruited for the study by convenience sampling. CYTER staff was conducting regular Yoga training sessions twice weekly for 6 months for nursing students and these participants were selected as they could perform the required set of Asanas with an adequate level of proficiency. Asanas selected for the study were: DA, Vakrasana (VA) (both sides), Janusirasasana (JSA) (both sides), Matsyasana, and Shavasana [Figure 1].
Figure 1.
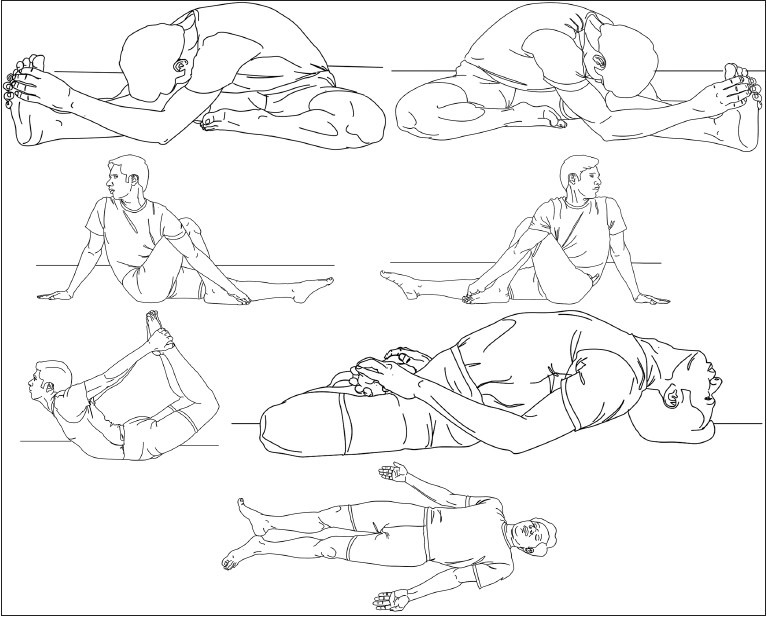
Asanas performed by participants in the study: Janusirasasana (right), Janusirasasana (left), Vakrasana (right), Vakrasana (left), Dhanurasana, Matsyasana, and Shavasana
We selected these Asanas as they manipulated the spinal column indifferent positions. The human spine is given great importance in the Yoga tradition (Brahma Danda or Meru Danda). The forward bending (JSA), backward bending (DA from the prone position and Matsyasana from supine position) and twisting VA nature of the Asanas was taken into consideration and also the fact that the effects of two of them (VA and JSA) could be evaluated on both right and left sides. These Asanas were also part of the syllabus of Yoga training the subjects had received earlier and hence an adequate level of proficiency in performance of the postures was also ensured.
Each subject came to CYTER on seven different days and the entire study took 3 weeks for its completion as all subjects couldn’t be studied on the same day due to the lack of space and manpower. On each of the days, they performed one of the Asanas that was selected by random selection of both subject and technique so as to avoid any bias or influence of different days on the group. All tests were carried out in CYTER between 10 and 12 noon. The environment was quiet, with a comfortable temperature and subdued lighting. The subjects were briefed about the study protocol and written informed consent was obtained from them. They were advised to finish their breakfast at least 2 h earlier and come after emptying bowel and bladder.
To ensure objectivity in measuring HR and BP, the recordings were performed using non-invasive semi-automatic BP monitor (CH - 432, Citizen Systems, Tokyo, Japan) with an instrumental accuracy of ± 5% for HR and ± 3 mm Hg for BP. Pre intervention HR and BP was recorded after 5 min of supine rest. The subjects then performed one of the Asanas for 30 s, following which the post-intervention recordings were taken. HR and BP were further recorded during the supine recovery period at 2,4,6,8 and 10 min.
Data were assessed for normality using GraphPad InStat version 3.06 for Windows 95, (GraphPad Software, San Diego California USA, www.graphpad.com). As all data passed normality testing by Kolmogorov-Smirnov Test, statistical analysis was carried out using repeated measures of ANOVA with Tukey-Kramer multiple comparisons test to compare differences between groups at each point of time. Student's paired t test and P values less than 0.05 were accepted as indicating significant differences for pre-post and recovery period intra-group comparisons.
RESULTS
There were significant changes in HR and BP both immediately after performing asanas as well as during the recovery period [Tables 1–3 and Figures 2–4]. Overall comparisons of changes immediately after the performance of the Asanas revealed significant differences with regard to HR that increased significantly after DA [Table 1, Figure 2]. In the recovery phase, there were significant intergroup differences from 2 min onward in both systolic pressure (SP) and diastolic pressure (DP) as given in Tables 2 and 3 and Figures 3 and 4. The decrease of SP after VA (right side) (VA-R) was significantly greater than Shavasana (4th, 6th, and 8th min) and JSA-L at 6th and 8th min [Table 2 and Figure 3]. DP decreased significantly after performing JSA-L compared to VA-R at the 6th and 8th min [Table 3 and Figure 4]. The plot of ∆% changes during the recovery period showed greater fall in SP and DP after all the other Asanas as compared to that following Shavasana [Figures 3 and 4].
Table 1.
Immediate HR response to the performance of DA, JSA-R, JSA-L, VA-R, VA-L, MA and SA for 30 s followed by subsequent HR recovery at 2,4,6,8 and 10 min
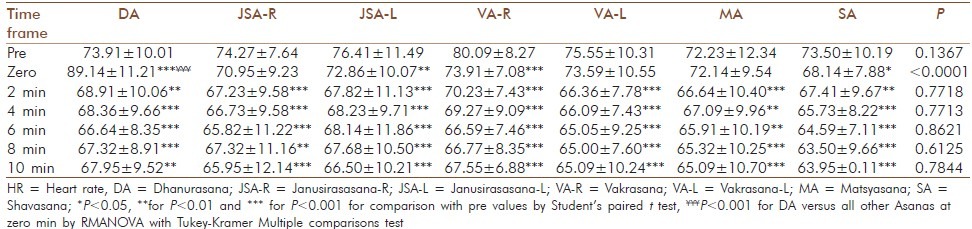
Table 3.
Immediate DP response to the performance of DA, JSA-R, JSA-L, VA-R, VA-L, MA and SA for 30 s followed by subsequent HR recovery at 2,4,6,8 and 10 min
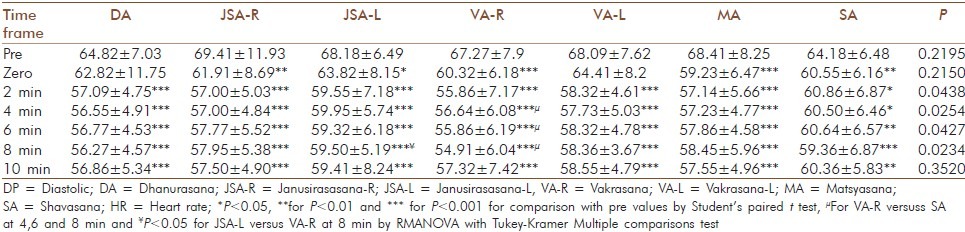
Figure 2.
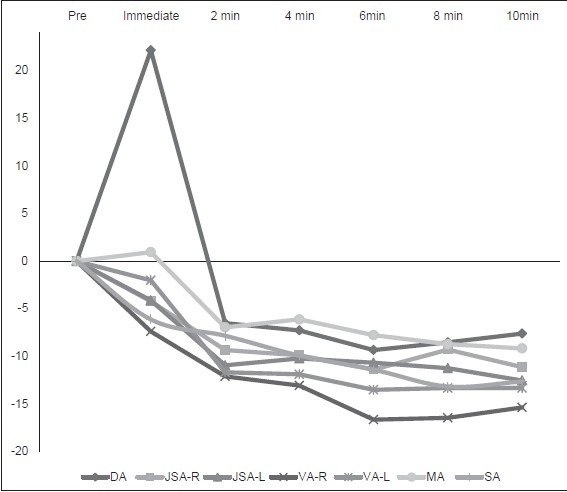
Heart rate response in Δ% immediately following performance of Dhanurasana, Janusirasasana-R, Janusirasasana-L, Vakrasana-R, Vakrasana-L, Matsyasana, and Shavasana for 30 s and at 2,4,6,8, and 10 min
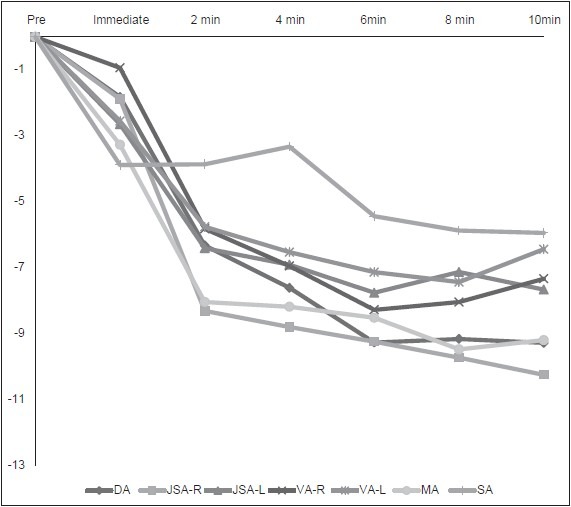
Figure 4.
Diastolic pressure response in Δ% immediately following performance of Dhanurasana, Janusirasasana-R, Janusirasasana-L, Vakrasana-R, Vakrasana-L, Matsyasana, and Shavasana for 30 s and at 2, 4, 6, 8 and 10 min
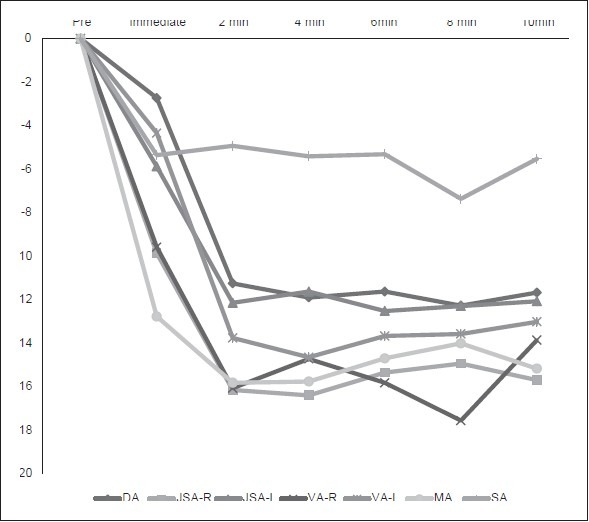
Table 2.
Immediate SP response to the performance of DA, JSA-R, JSA-L, VA-R, VA-L, MA and SA for 30 s followed by subsequent HR recovery at 2,4,6,8 and 10 min
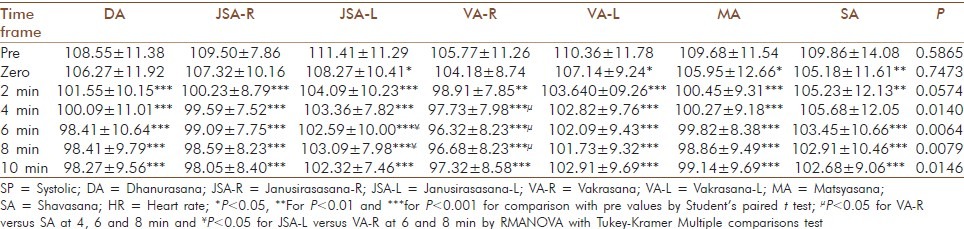
Figure 3.
Systolic pressure response in Δ% immediately following performance of Dhanurasana, Janusirasasana-R, Janusirasasana-L, Vakrasana-R, Vakrasana-L, Matsyasana and Shavasana for 30 s and at 2, 4, 6, 8 and 10 min
DISCUSSION
The cardiovascular changes immediately after performing the Asanas and during the recovery phase as evidenced in this study reveal inherent differences between the selected postures [Tables 1–3, Figures 2–4]. Differences between the selected Asanas were especially significant for HR immediately after performing DA [Table 1 and Figure 2]. There was a higher stress response to DA as opposed to the other Asanas and this may be attributed to an increased sympathetic response due in part to the relative difficulty of the posture as well as the intense abdominal compression occurring while performing it.
Each of the Asanas had its own pattern and through there were overall similarities, some differences can be made out in a detailed examination. VA-R had the greatest fall in HR during the recovery period while JSA-R had the greatest fall of both SP and DP by the end of the 10 min recovery period [Tables 1–3 and Figures 2–4]. There were significant differences between the selected Asanas mainly during the recovery period after 2 min and this finding helps us to understand that the effects of the Asanas is quite similar after 2 min. This also implies that a rest of 2 min should be given in between the Asanas if one is to attain the best relaxatory effect of Yoga practices.
A previous study on individual Asanas evaluated the BP while 25 medical students performed Sukhasana, Vajrasana and DA and also compared these findings with the supine, sitting, and standing positions.[7]DA had the highest BP as compared to all other postures in that study too. The main difference between our present study and that study is that they had measured the BP while the subjects were in the posture, whereas we have measured before and after the posture along with a 10 min recovery period. They had only recorded a single value and thus there was no pre-post comparison in their study. It is also to be noted that their subjects were not regular practitioners of Yoga while our subjects were undergoing a Yoga training program and had been practicing the techniques for more than 3 weeks at the time of the study.
Previous studies have reported the energy expenditure and ventilatory responses of Yogic standing (Virasana) and sitting (Siddhasana) postures.[11,12]They reported that Virasana induces temporarily a hyper metabolic state characterized by enhance sympathetic activity that gets inhibited upon the adoption of Shavasana.[11]Siddhasana was reported to be a mild type of exercise as it had higher energy expenditure and ventilatory responses as compared to supine and chair sitting postures.[12]
The effect of supine relaxation is more pronounced after the performance of the Asanas as compared to just relaxing in Shavasana [Figures 2–4]. This may be attributed to a normalization and resultant homeostatic effect occurring towing to a greater, healthier de-activation of the autonomic nervous system occurring due to the presence of prior activation.
A study by Telles et al. studied O2 consumption and respiration following four Yoga postures interspersed with relaxation and supine relaxation alone, and concluded that the combination of stimulating and relaxing techniques reduced physiological arousal better than the mere practice of relaxation techniques alone.[13]They also pointed out that though the practical performance of Yoga techniques seem to be stimulatory in nature, their physiological effects are in fact more relaxatory. This is corroborated by a previous study from JIPMER reporting that Shavasana relaxation is enhanced with the addition of Savitri Pranayama thus decreasing O2consumption by 26%.[14]
Manjunatha et al. studied the effects of selected Yogic postures on fasting and postprandial glycaemia and insulinemia in healthy young subjects and concluded that the performance of Asanas led to increased sensitivity of the β cells of the pancreas to the glucose signal.[15]It was found in that study that the performance of four different sets of Asanas had similar effects of reducing fasting and postprandial glycaemia and that blood insulin levels also fell after the performance of the Asanas. However, when oral glucose tolerance test ( GTT) was administered, there was a greater insulin response that may be interpreted as an enhanced sensitivity of pancreatic β cells to the glucose challenge too. At the metaphysical level, this may be taken to imply a dynamic state of balance where one is balanced, yet ready to face any challenge that may occur.
One of the extra findings of this study is the revelation of subtle differences between the right sided and left sided performance of VA and JSA that may be occurring as a result of the different internal structures being either compressed or relaxed on either side. This requires further exploration and studies with a greater number of subjects and doing the Asanas in different positions may help unravel the scientific basis of such differences.
The aim of Yoga is harmony or homeostatic balance at all levels of existence (Samatvam yogah uchyate) as elucidated in the Bhagavad Gita[16]and the psychophysiological nature of Yoga Asanas may be producing such a balance even if they initially have a hyper metabolic or cardio-respiratory stimulatory action. This is well evidenced by the cardiovascular responses to all the Asanas in our study, as the post postural HR and BP both fell below the initial values during the recovery period and this was consequently seen to be even lower than the responses to supine relaxation in Shavasana. This has been corroborated by recent reports that both the sympathetic and parasympathetic limbs of the autonomic nervous system activity were enhanced in hypertensives following Yoga training.[17,18]
In conclusion, our study provides initial evidence of differential cardiovascular effects of Asanas and subtle differences between right and left sided performance. Further, cardiovascular recovery is greater after the performance of the Asanas as compared to Shavasana; thus, implying a better response when effort precedes relaxation.
ACKNOWLEDGMENTS
The authors thank the management and authorities of Sri Balaji Vidyapeeth University for setting up the Centre for Yoga Therapy, Education and Research (CYTER) in Mahatma Gandhi Medical College and Research Institute (MGMCRI). The authors are grateful to Yogacharini Meenakshi Devi Bhavanani, Director ICYER and Dr. Madanmohan, Professor and Head Department of Physiology, MGMCRI for their constant motivation, encouragement and supportive guidance. We thank Miss Subashana, ANM for her valuable assistance during the recording sessions and data entry.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Khalsa SB. Yoga as a therapeutic intervention: A bibliometric analysis of published research studies. Indian J Physiol Pharmacol. 2004;48:269–85. [PubMed] [Google Scholar]
- 2.Innes KE, Bourguignon C, Taylor AG. Risk indices associated with the insulin resistance syndrome, cardiovascular disease, and possible protection with yoga: A systematic review. J Am Board Fam Pract. 2005;18:491–519. doi: 10.3122/jabfm.18.6.491. [DOI] [PubMed] [Google Scholar]
- 3.Innes KE, Vincent HK. The influence of yoga-based programs on risk profiles in adults with type 2 diabetes mellitus: A systematic review. Evid Based Complement Alternat Med. 2007;4:469–86. doi: 10.1093/ecam/nel103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bhavanani AB. Yoga as a therapy: A perspective. Yoga Mimamsa. 2011;42:235–41. [Google Scholar]
- 5.Bhavanani AB. Don’t put yoga in a small box: The challenges of scientifically studying yoga. Int J Yoga Therap. 2011;21:21. [PubMed] [Google Scholar]
- 6.Swami GG. Yoga: Step-by-Step. Pondicherry: Satya Press; 1981. [Google Scholar]
- 7.Malhotra V, Tandon OP. A study of the effect of individual Asanas on blood pressure. Indian J Tradit Knowl. 2005;4:367–72. [Google Scholar]
- 8.Bhavanani AB. Swarodaya vijnana-A scientific study of the nasal cycle. Yoga Mimamsa. 2007;39:32–8. [Google Scholar]
- 9.Werntz DA, Bickford RG, Bloom FE, Shannahoff-Khalsa DS. Alternating cerebral hemispheric activity and the lateralization of autonomic nervous function. Hum Neurobiol. 1983;2:39–43. [PubMed] [Google Scholar]
- 10.Shannahoff-Khalsa DS. Unilateral forced nostril breathing: Basic science, clinical trials, and selected advanced techniques. Subtle Energies and Energy Medicine Journal. 2002;12:79–106. [Google Scholar]
- 11.Rai L, Ram K. Energy expenditure and ventilatory responses during Virasana - A yogic standing posture. Indian J Physiol Pharmacol. 1993;37:45–50. [PubMed] [Google Scholar]
- 12.Rai L, Ram K, Kant U, Madan SK, Sharma SK. Energy expenditure and ventilatory responses during Siddhasana - A yogic seated posture. Indian J Physiol Pharmacol. 1994;38:29–33. [PubMed] [Google Scholar]
- 13.Telles S, Reddy SK, Nagendra HR. Oxygen consumption and respiration following two yoga relaxation techniques. Appl Psychophysiol Biofeedback. 2000;25:221–7. doi: 10.1023/a:1026454804927. [DOI] [PubMed] [Google Scholar]
- 14.Madanmohan S, Rai UC, Balavittal V, Thombre DP, Gitananda S. Cardiorespiratory changes during savitri pranayama and shavasan. Yoga Rev. 1983;3:25–34. [Google Scholar]
- 15.Manjunatha S, Vempati RP, Ghosh D, Bijlani RL. An investigation into the acute and long-term effects of selected yogic postures on fasting and postprandial glycemia and insulinemia in healthy young subjects. Indian J Physiol Pharmacol. 2005;49:319–24. [PubMed] [Google Scholar]
- 16.Swami C. The Bhagavad Gita. Trichy: Ramakrishna Tapovanam; 1984. [Google Scholar]
- 17.Vijayalakshmi P, Madanmohan, Bhavanani AB, Patil A, Babu K. Modulation of stress induced by isometric handgrip test in hypertensive patients following yogic relaxation training. Indian J Physiol Pharmacol. 2004;48:59–64. [PubMed] [Google Scholar]
- 18.Bhavanani AB, Madanmohan S, Zeena S. Suryanadi pranayama (right unilateral nostril breathing) may be safe for hypertensives. J Yoga Phys Ther. 2012;2:118. [Google Scholar]