

Abstract
Driving is an important part of everyday life for most adults, and restrictions on driving can place a significant burden on individuals diagnosed with epilepsy. Although sensorimotor deficits during seizures may impair driving, decreased level of consciousness often has a more global effect on patients’ ability to respond appropriately to the environment. Better understanding of the mechanisms underlying alteration of consciousness in epilepsy is important to decision making for people with epilepsy, their physicians, and regulators in regards to the question of fitness to drive. Retrospective cohort and cross-sectional studies based on surveys or crash records can provide valuable information about driving in epilepsy. However, prospective objective testing of ictal driving ability during different types of seizures is needed to more fully understand the role of impaired consciousness and other deficits in disrupting driving. Driving simulators adapted for use in the epilepsy video/EEG monitoring unit may be well-suited to provide both ictal and interictal data in patients with epilepsy. Objective information about impaired driving in specific types of epilepsy and seizures can provide better-informed recommendations regarding fitness to drive, potentially improving quality of life for people living with epilepsy.
Keywords: Epilepsy, consciousness, driving, complex partial seizures, simple partial seizures, generalized tonic-clonic seizures
Introduction
Loss of driving privileges can have a profound impact on the quality of life of individuals diagnosed with epilepsy [1]. For most adults, driving is a primary means of transportation and is necessary for employment, maintaining social ties, and performing other tasks essential to independent living.
Regulations restricting people with epilepsy (PWE) from obtaining or keeping a driving license seek to limit the risk that drivers with epilepsy might pose to themselves and others. Driving risk in PWE has two components: 1) general driving ability may be affected due to anti-epileptic drug (AED) side effects and/or by the underlying pathology generating the individual’s seizures [2–4], 2) intermittent risk of loss of consciousness or motor control due to a seizure while driving. In this review we will focus on transient impairment that may occur due to loss of consciousness during seizures, mechanisms, consequences and future directions to better understand and prevent this important co-morbidity of epilepsy.
1. Epilepsy and driving
The literature on epilepsy and driving consists largely of cohort studies based on analysis of government and medical databases or surveys of PWE which attempt to determine if PWE are at an elevated risk of motor vehicle accidents (MVA’s) [5]. One disadvantage of these studies is the inability to causally link specific MVA’s to the occurrence of a seizure while driving; as a result, most studies have made no distinction between MVA’s occurring with or without seizure.
Studies have generally reported moderate [6–12] or rarely no [13] increases in overall MVA rates for PWE (table 1). A 2012 analysis by Classen et al [5] of studies published between 1994 and 2010 determined that, based on 4 studies [9, 14–16] which met their criteria, epilepsy is likely not predictive of increased MVA’s, but also noted a lack of consistency in the literature. On the other hand, a meta-analysis conducted by the Department of Transportation Federal Motor Carrier Safety Administration as part of a 2007 comprehensive evidence report estimated PWE to have an accident rate of between 1.13 and 2.16 times that of normal subjects [17], based on 8 studies [6, 7, 9–13, 16]; heterogeneity in reported data was again noted. Conflicting results from different large sample studies may point to important differences in study methods, population samples, geographical locations, and time periods (see table 1).
Table 1.
Retrospective studies of driving and epilepsy.
| Authors, Title. (journal, year), location. | Data sources | Sample information | RR/O R, PWE vs controls | Rates of accidents reported (units reported) | Other findings regarding epilepsy | Findings regarding other medical conditions |
|---|---|---|---|---|---|---|
| Waller, Chronic Medical Conditions and Traffic Safety: Review of the California Experience. (NEJM, 1965), CA, USA [6] | CA DMV records under review of persons with reported chronic medical conditions. Periodic medical reports were submitted by these drivers’ physicians. | N=445 PWE, N=1,646 control | RR=1.95* | PWE: 16.0 vs 8.2, CVD: 14.6 vs 9.0, DB: 15.5 vs 8.7, ALC: 11.3 vs 6.8 (Accidents/1,000,000 miles driven, condition vs matched control) | Initial action following a driving violation in PWE was more likely to be license revocation (61%) than in CVD (39%) and DB (26%) | CVD (N=216): RR=1.62*, DB (N=257): RR=1.78*, ALC(N=261): RR=1.66* |
| Crancer and McMurray, Accident and Violation Rates of Washington’s Medically Restricted Drivers. (JAMA, 1968), WA, USA [12] | WA DMV records of all medically restricted drivers were analyzed between Jan 1, 1961 to Oct 1, 1967. | N=1,169 PWE, N=1,631,186 control | RR=1.33* | PWE: 41.40 vs 31.06, CVD: 25.87 vs 25.28, DB: 31.45 vs 26.50 (Accidents/100 drivers in study period, condition vs matched control) | -- | CVD (N=7,416): RR=1.02, DB (N=7,646): RR=1.19* |
| van der Lugt, Traffic accidents caused by epilepsy. (Epilepsia, 1975), Netherlands [19] | Police reports of accidents investigated and determined to be caused by epilepsy between 1959 and 1968. | N=155 crashes attributed to epilepsy, N=179,000 control | -- | -- | Of the 155 crashes attributed to epilepsy, the rate of serious injury (N=3, 1.9%) was lower than in comparison group (7.8%)*. | -- |
| Gastaut and Zifkin, The risk of automobile accidents with seizures occurring while driving: Relation to seizure type. (Neurology, 1987), location not reported [21] | Interviews with a set of drivers with epilepsy. Study does not specify where or how these drivers were recruited. | N=400 drivers with epilepsy, no control | -- | -- | 33% of the 400 drivers had one or more seizures at the wheel, and 17% had an accident due to seizure. 81% of seizures while driving were reported to be CPS, 9% SPS, 10% generalized. 55% of seizures led to an accident. | -- |
| Popkin and Waller, Epilepsy and driving in North Carolina: an exploratory study. (Accid Anal & Prev, 1988), NC, USA [8] | NC DMV records of patients treated at NC Division of Health Services clinics for epilepsy. | N=112 PWE, no control (a previously reported control rate was used) | RR=1.43 | PWE: 8.6 vs 6.0 (Accidents per 100 drivers per year, condition vs previously reported control rate) | -- | -- |
| Hansotio and Broste, The effect of epilepsy or diabetes mellitus on the risk of automobile accidents. (NEJM,1991), WI, USA [11] | WI Dept of Transportation records and medical records for PWE treated at a single medical center were analyzed. | N=241 PWE, N=30,420 control | RR=1.33* | PWE: 68.54 vs 51.54 (Accidents per 1000 person-years, condition vs matched control) | Crashes involving PWE were more likely to cause injury, RR=1.63*, as did crashes involving DB, RR=1.57*. | DB (N=484): RR=1.32* |
| Bener et al, The effect of epilepsy on road traffic accidents and casualties. (Seizure, 1996), El Ain, UAE [15] | Questionnaire given to drivers admitted to the ER of a large hospital between Oct 1992 and Jun 1994, with a response rate of 86%. | N=41 PWE, N=1,674 control | -- | -- | Accidents involving PWE were more likely to involve property damage, and thus were likely more serious, RR=1.85*. | -- |
| Taylor et al, Risk of accidents in drivers with epilepsy. (J Neurol Neurosurg Psychiatry, 1996), England [13] | Survey sent to PWE who reported their epilepsy to the Driver and Vehicle Licensing Authority; survey response rate of 72%. | N=16,958 PWE, N=8,888 control | OR=0.77 unadjusted, 0.95 adjusted† | Not explicitly reported. However, PWE: 24.78 vs 28.78, RR=0.86, (Accidents per 100 drivers over 3 years, calculated from numbers reported) | PWE were more likely to be in an accident involving severe injury, adjusted OR=1.33*. | -- |
| Krauss et al, Risk factors for seizure-related motor vehicle crashes in patients with epilepsy. (Neurology, 1999), MD, USA [22] | Review of medical charts and a questionnaire administered to epilepsy patients known to drive. | N=50 PWE who crashed, N=50 PWE who did not crash. | -- | -- | Risk of accidents was reduced 93% for PWE with ≥ 12 month SFI vs shorter SFI*. Higher seizure frequency related to odds of crash*. Reliable auras reduced odds of crash*. 26% crashed despite having aura with seizure. | -- |
| Berg et al, Driving in adults with refractory localization- related epilepsy. Multi-Center Study of Epilepsy Surgery. (Neurology, 2000), CT,NY,PA,MN, USA [18] | Structured interviews of PWE wih refractory epilepsy (pre-surgery) being followed as part of a study on outcomes of epilepsy surgery. | N=367 PWE (refractory epilepsy), no control | -- | -- | 39% of these high-risk subjects had experienced one or more seizures while driving. 27% of subjects had at least 1 accident due to a seizure while driving. 32% of these accidents caused injury to self, 20% injury to others. | -- |
| Lings, Increased driving accident frequency in Danish patients with epilepsy. (Neurology, 2001), Odense, Denmark [9] | Records from multiple government and civil databases, including Danish Central Person Registry, Central Register of Driving Licenses, and medical records at a hospital were analyzed. | N=159 PWE, N=559 control | -- | -- | PWE more likely to be admitted to a hospital for crash-related injury: RR=7.01*‡ (Rates of hospital admittance for crash- related injury per 1,000 person-years). All PWE with injuries in an accident (N=10) had grand mal attacks as their primary seizure type. | -- |
| Vernon et al, Evaluating the crash and citation rates of Utah drivers licensed with medical conditions, 1992–1996. (Accid Anal & Prev 2002), UT, USA [7] | Records were linked from: UT Drivers License Division, Dept of Transportation, Dept of Health for period of 1992–1996, for all drivers who reported a medical condition on a license application. | N=2,739 PWE, N=1,750,918 control (all UT licensed drivers) | RR=1. 73*, unrestricted drivers, RR=1. 47*, those with restrictions § | PWE: 2.69 vs 1.55, CVD: 1.04 vs 1.05, DB,1.70 vs 1.30, ALC/drugs: 3.09 vs 1.70. (Accidents/10,000 license days, unrestricted drivers, condition vs matched control) | RR=2.02 for at-fault crashes in unrestricted PWE drivers, RR=2.39 for PWE drivers with some restrictions. | Condition (RR for unrestricted drivers, RR for drivers with some restriction): CVD(0.99,1.37), DB(1.30*,1.38), ALC and drugs(1.82*,4.21*). |
| Drazkowski et al, Seizure-related motor vehicle crashes in Arizona before and after reducing the driving restriction from 12 to 3 months. (Mayo Clin Proc, 2003), AZ, USA [25] | Crash data from the AZ Motor Vehicle Division was analyzed for 3 years before (1991–1993) and 3 years after (1994–1996) a change in seizure-free-interval required for PWE to be allowed to drive. | N=125 seizure- related crashes, N ≈ 614,000 total crashes. | -- | -- | No significant change was found in rates of crashes attributable to seizures following the change in policy (RR=0.98, comparison of accident rates after to before). | -- |
| Sheth et al, Mortality in epilepsy: driving fatalities vs other causes of death in patients with epilepsy. (Neurology, 2004), USA [16] | Death certificates for fatal crashes in the entire USA compiled from the National Center for Health Statistics for the period of 1995–1997, analyzed based on the conditions recorded as contributing to the crash. | N=259 fatal crashes attributed to seizures, N=131,823 other fatal crashes. | -- | -- | Fatal crash rates lower in PWE: RR=0.38 §§ (rates of fatal crashes per 100,000 people). 4.2% of medically related and 0.2% of all fatal crashes were seizure related. No significant difference in rates of fatal crashes among states with different seizure-free- interval requirements. | CVD: RR(fatal crashes)=0.17, DB: RR=0.08, ALC: RR=3.23. |
finding was reported to be statistically significant with at least p<0.05. Due to widely different statistical tests used and methods of report, no attempt was made to distinguish between different levels of significance.
List of abbreviations: PWE, people with epilepsy, RR, relative rate, OR, odds ratio, CVD, cardiovascular disease, DB, diabetes, ALC, alcohol addiction or abuse, DMV, Department (or Division) of Motor Vehicles, CPS, complex partial seizure, SPS, simple partial seizure, SFI, seizure free interval.
Odds ratio was adjusted for covariates: age, age squared, sex, whether or not driving in previous year, annual mileage, years of driving experience, years of driving experience squared. Logistic regression was used.
Only 10 cases of treatment of injury were recorded in PWE vs 5 for the control group; such a small sample might account for this very high RR.
These restrictions included speed limitations, area limitations, time of day limitations, or other special restrictions.
The numbers of certain medically attributable fatal crashes may be underrepresented, as it is difficult to determine post-mortem from a death certificate whether a crash was related to epilepsy, cardiovascular disease or diabetes, versus alcohol abuse (blood alcohol level). In addition, prevalence rates of medical conditions used did not take into account that not all people with a condition drive or are licensed. These factors may have led to the low RR reported for PWE, CVD, and DB.
Although overall risk of driving accidents in PWE may be only minimally or moderately increased compared to controls, another important question is the severity of damage in accidents that do occur. Several studies have reported that crashes in PWE are more likely to cause injury, death or property damage than in controls (table 1) [9, 11, 13, 15, 18]. Two studies which reported a lower risk of serious of fatal MVA in PWE may have been biased by the difficulty of determining an epilepsy diagnosis from death certificates [16], or small sample size [19]. In any case, the rate of fatal accidents in PWE has been reported to be lower than that of the highest-risk groups such as young drivers and those who abuse alcohol [6, 16, 20].
Few studies have attempted to stratify driving risk based on levels of ictal impairment or types of seizures [21]. The beliefs that auras provide sufficient warning of seizures, and that PWE are able to drive safely through auras or simple partial seizures, have not been well studied [5], although some studies (based on self-report) indicate that PWE who experience warnings before their seizures may be less likely to crash [21, 22]. The difficulty of making case by case decisions on fitness to drive is compounded by the fact that the self-report of PWE and their family and friends on the frequency and level of impairment of seizures can be unreliable [23].
Objective evidence on driving and epilepsy is crucial for decision making of physicians, patients, and regulators. A mosaic of regulatory procedures currently exists in the United States. More than half of states require PWE to demonstrate a seizure-free interval of between 3 and 24 months before being allowed to drive [24, 25]. Some states have adopted more flexible procedures in place of or in addition to seizure free intervals: fitness to drive can be determined by a medical advisory board or by the individual’s physician [24, 26]. In many states physicians are legally liable for the driving advice they give to PWE [24, 26]. International regulations are similarly variable, with a number of countries banning PWE from ever driving [27].
2. Impaired consciousness in epilepsy and driving
The diverse semiology of epileptic seizures includes motor convulsions or other motor impairments, sensory impairment in vision, audition and proprioception, hallucinations, emotional distress, memory impairment, aphasia, as well as alterations of overall level of responsiveness or consciousness. While any one or combination of these symptoms potentially jeopardizes safe driving, some, such as motor and visual impairment and especially loss of consciousness, may pose greater risk than others.
Recurrent episodes of alteration of consciousness during epileptic seizures are a cause of significant disability in PWE [28]. Seizures that alter consciousness interfere with a specialized network of cortical and sub-cortical brain structures, termed the consciousness system, crucial to the maintenance of the waking state, attentiveness to and awareness of memory, sensory and motor systems, emotions and drives, all of which comprise normal consciousness [29]. The components of the consciousness system include the higher-order frontal and parietal association cortices (figure 1), as well as subcortical arousal systems in the upper brainstem, thalamus, basal forebrain, hypothalamus, and other structures [29]. Cortical and subcortical structures interact strongly through reciprocal connections to produce a great variety of states differing in levels of wakefulness, attention, and awareness.
Figure 1.
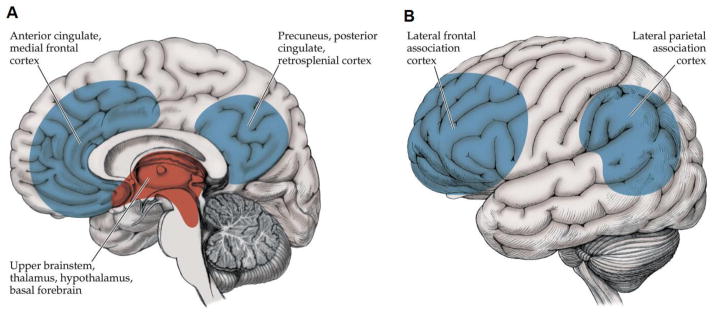
The consciousness system. (A) Medial view and (B) lateral view of anatomical structureswhich regulate the level of consciousness. Generalized tonic-clonic, absence and complex partial seizures disrupt function in these structures bilaterally and cause impaired consciousness. Cortical components are shown in blue. Subcortical components are shown in red. Other circuits, such as the basal ganglia and cerebellum, might also participate. Reproduced from Blumenfeld by permission of Sinauer Associates [70].
Not surprisingly, brain structures related to alert, attentive driving overlap with many of the same structures necessary for consciousness [30–32]. Parieto-occipital cortices and other brain regions important for perception and motor control were found to be activated during driving in one neuroimaging study [32]. Avoidance of collisions was found to involve mid and anterior cingulate, precuneus, posterior parietal cortex, and bilateral ventrolateral pre-frontal cortex [32]. Information processing, sensory-motor integration based on visual, proprioceptive and auditory input, coordination, attention, memory, and decision making are all critical components of consciousness and driving that are at risk of being impaired during seizures.
Seizures which cause loss of consciousness include three types: generalized tonic-clonic seizures (GTCs), complex partial seizures, and absence seizures. GTCs, or grand mal seizures, are perhaps the most widely known to the general public due to their association with convulsions. GTCs cause severe impairment of consciousness for the duration of the seizure and for a significant post-ictal period [29, 33, 34]. The impairment is likely caused by abnormal electrical activity in the brain affecting specific brain structures in the ictal and post-ictal periods [35–37]. SPECT imaging during secondarily generalized complex partial seizures showed involvement of regions of the brain important for consciousness [36]. In general, GTCs last about 2 minutes and cause profound impairment of consciousness along with convulsions; lasting impairment is found post-ictally for a significant duration as the patient recovers [29, 33, 34, 38]. Patients are unable to remember events around the time of the seizure [34, 38], and during the seizure cannot perform simple tasks such as grasping a ball and visual tracking [33]. These seizures pose catastrophic risk if occurring during driving [21, 39].
Complex partial seizures affect a focal region of the brain, often the temporal lobe, but are associated with loss or alteration of consciousness. An explanation for this mismatch in effect in temporal lobe epilepsy has been proposed and studied by our lab and others. The network inhibition hypothesis offers the following mechanism: focal seizure discharges in the temporal lobe are carried to subcortical structures via known anatomical connections and activate GABA-ergic neurons, causing powerful inhibition of subcortical arousal structures in the upper brainstem, thalamus, basal forebrain and hypothalamus [29, 40]. This results in deactivation of neocortex and impairment of consciousness. Intracranial electroencephalography (EEG) during complex partial seizures shows slow wave activity similar to that recorded during deep sleep and coma; on the other hand, simple partial seizures do not exhibit strong slow wave activity in the neocortex [41, 42]. The network inhibition hypothesis is borne out by animal and human studies linking activity in subcortical regions to slow wave activity and decreased blood flow in neocortex [40]. Cutting the fornix prevented the spread of seizures to subcortical regions and spared behavioral arrest in rats [41], and other recent work showed that subcortical neurons important for arousal are inactivated during limbic seizures in rats [43]. Complex partial seizures last 1–2 minutes and are associated with alteration of consciousness, but sometimes spare automatic or simple functions such as grasping a ball and visual tracking [33]. It is unclear whether a more complex task such as driving might be spared, even partially, during some complex partial seizures.
Absence seizures are most commonly found in children and are associated with abrupt onset and offset of brief (5–20s) behavioral arrest. Abnormal hyper-synchronous oscillations in thalamocortical networks are thought to be central to the generation of the characteristic spike-wave discharge seen on EEG, and to ictal impairment of consciousness [44–46]. Behavioral testing during absence seizures shows that simple tasks such as repetitive tapping are relatively spared compared to more complex tasks involving higher order processing [45, 46]. It is unclear whether the short duration and sparing of simple behaviors during absence seizures would lead to partial sparing of driving ability.
Perhaps most important to characterize in relation to driving are seizures that do not impair consciousness, including auras and simple partial seizures. These seizures are focal but vary greatly in the regions of the brain affected and therefore cause symptoms which may have variable effects on driving. Whether ictal effects of simple partial seizures, or interictal effects of brief epileptiform discharges are benign during driving have not been well studied.
3. Approaches to studying impaired consciousness and driving in epilepsy
Efforts have been made to test ictal deficits in consciousness associated with different types of seizures [34, 38, 47–52]. A standardized battery of questions and commands administered during seizures to patients undergoing continuous video-EEG (vEEG) monitoring demonstrated the feasibility of prolonged ictal and post-ictal testing of components of consciousness. Results of this battery, named the Responsiveness in Epilepsy Scale (RES) [39], and its revised form (RES-II) [34], showed greater impairment in generalized tonic-clonic seizures than partial seizures [33, 34, 39]. In addition, partial seizures with impairment were more likely to be associated with changes on EEG. It was also reported that a task involving grasping of a ball and visual tracking were spared in 52% of complex partial seizures as compared to 7% of GTCs [33]. Simple non-verbal tasks may be spared in some cases of complex partial seizures [34, 39, 50, 52].
Other groups have used retrospective analysis of vEEG and self-report of seizures by patients to study pre-ictal, ictal and post-ictal impairment of consciousness [51–53]. Ictal cognitive assessment in the form of a command with verbal and non-verbal cues (shake my hand) and a verbal and visual memory task was administered during seizures by semi-trained staff and family members in one study [48]. Some responsiveness (any verbal or non-verbal responses to the command), was found in 21/115 (18%) complex partial seizures, but full responsiveness in only 2/115 (2%) [48].
Cavanna et al [51] used a carefully designed quantitative questionnaire to tease out patient’s self-report of ictal deficits in content and level of consciousness [54], providing a subscore for each category. The study compared temporal, frontal lobe, and idiopathic generalized epilepsies, finding that generalized seizures caused significantly greater impairment in level of consciousness, while temporal lobe seizures spared content of consciousness relative to the other two seizure types [51].
In summary, testing of patients during seizures occurring in controlled settings has yielded some insight into ictal deficits in consciousness, which in turn may shed some light on ictal ability to drive. In order to better understand deficits in driving ability, however, testing must include complex tasks more relatable to driving.
To this end, artificial driving systems of varying real world fidelity may provide useful data. Driving simulators have been used to capture objective driving performance data in populations with risk factors such as alcohol use, dementia, cardiovascular disease, sleep apnea [30, 38, 55–65], and may represent a safe way of separately testing the two components of risk in driving with epilepsy described above. However, to date few studies have attempted to characterize deficits in driving ability in PWE using simulators [38, 57, 58, 60].
Yang et al utilized a driving video game with steering wheel and pedals to evaluate performance during seizures monitored by vEEG (N=22 seizures in 13 patients) [38]. Impairment in different types of seizures showed similar trends to a study by Gastaut and Zifkin [21], in that GTCs showed the greatest impairment, while partial seizures and absence seizures caused more variable impairment (Table 2, Figure 2). Auras and subclinical seizures had no discernible effect on driving [38]. The daunting challenge of capturing infrequent seizures during a driving task was highlighted by the fact that on average one seizure was captured for every 18.5 hours of game play [38].
Table 2.
Impairment during seizures while playing driving video game
| Seizure type | Analysis of Video/EEG | Analysis of driving game output variables
|
|||||
|---|---|---|---|---|---|---|---|
| Behavioral description | At least one collision during seizure | Total collisions during seizures | Steering wheel velocity impairment | Throttle impairment | Car velocity impairment | Seizures with any evidence of impairment | |
| Subclinical seizures | 0/3 stopped playing | 0/3 (0%) | 0 | 0/3 (0%) | 0/3 (0%) | 0/3 (0%) | 0/3 (0%) |
| Aurasa | 0/1 stopped playing | -- | -- | -- | -- | -- | -- |
| Partial seizuresb | 4/6 stopped playing and behaved differently | 3/4 (75%) | 4 | 1/3 (33%)c | 2/3 (67%)c | 2/3 (67%)c | 3/4 (75%) |
| Absence seizuresd | 1/4 stared and paused playing ~10 s, 1/4 off camera, (2/4 continued play) | 1/2 (50%) | 3 | 0/2 (0%) | 0/2 (0%) | 0/2 (0%) | 1/2 (50%) |
| Secondarily generalized seizures | 2/2 sudden tonic posturing and stopped playing | 0/2 (0%) | 0 | 1/2 (50%) | 2/2 (100%) | 2/2 (100%) | 2/2 (100%) |
For all entries, numerator is number of seizures and denominator is total number of seizures analyzed.
One patient had an aura while playing the video game but output variables could not be analyzed due to technical problems.
Two partial seizures were analyzed by video/EEG review but could not be analyzed by video game output variables because of technical problems.
Steering, throttle and car velocity were not analyzed for one partial seizure because the patient was stopped from playing by a family member. However, there was one collision before this happened.
Two absence seizures were analyzed by video/EEG review but could not be analyzed by video game output variables because of technical problems. Reproduced with permission from Yang et al [38].
Figure 2.

Performance on driving simulator during examples of different seizure types. (A) Partial seizure with impaired driving. (B) Partial seizure with impaired driving. Note that after the second collision, the throttle remained depressed for a while but the car did not move as it had collided with a wall. (C) Absence seizure with collisions. Note that the first two collisions occurred very close together and appear merged at this time resolution. (D) Secondarily generalized seizure with impaired driving. Driving performance variables are all shown in arbitrary game units. Steering wheel velocity (top row) is the absolute value of the derivative of the steering wheel position versus time. Throttle (second row) shows engagement of the throttle, where 1.0 means the gas pedal is fully depressed and 0 means the patient’s foot is off the pedal. Car position (third row) displays the location of the vehicle in terms of the game world grid, according to two dimensions X and Y versus time. Car velocity (fourth row) shows total speed versus time. In all plots, time is relative to seizure onset, which is time 0. Reproduced with permission from Yang et al [38].
A central question in the use of simulations is whether they are valid measures of real driving performance. Face validity, or validity of users’ reaction to the system, and relative validity, or agreement in overall trends of performance between simulation and real life performance, have been established in specific cases [58, 59, 62, 63, 66, 67]. Although it is important to acknowledge the limitations of simulator data in making generalizable conclusions, we should also recognize the value of the qualitative insights they may contribute.
Conclusions
There is a present need to understand the impact of epilepsy on driving in both the ictal and interictal periods. In addition to broad retrospective studies analyzing the driving safety patterns of large cohorts, prospective ictal testing of PWE is needed to understand acute effects of seizures on consciousness and driving ability. Prospective testing of driving ability in PWE also provides objective data on the impact of seizure-related pathology and/or AEDs on fitness to drive in the interictal period.
Impaired consciousness during seizures is likely to be an important factor in determining driving risk. However, additional studies are needed to rigorously determine which seizure types are specifically associated with impaired driving and whether impaired consciousness, impaired motor function or other deficits interfere with driving in individual cases. Ideally, patients could be tested with realistic driving simulators to estimate their real-world risk of driving during their habitual seizures, auras and interictal epileptiform activity.
Liberalization of driving restrictions in parts of the United States and elsewhere has come about in response to recognition that many cases of epilepsy can be effectively controlled by AEDs [20], and to evidence suggesting that well-controlled epilepsy does not pose an extraordinary risk to traffic safety [5, 17] in comparison to other risk factors such as age or medical conditions besides epilepsy [6, 11, 16].
Ultimately, driving safety in epilepsy relies on the judgment of individuals with epilepsy and their compliance with regulations and medical advice [18, 68, 69]. Better evidence strengthens the ability of physicians and regulators to provide convincing and appropriate advice, and may promote adherence among at-risk drivers with epilepsy to regulations intended to keep themselves and others safe. At the same time, a stronger understanding of the effects of different types of seizures on consciousness and driving ability may help remove driving restrictions for those who pose little risk to themselves and others, potentially improving quality of life among people living with epilepsy.
Highlights.
Loss of consciousness during seizures is an important factor in driving risk
Testing of ictal behavior is needed to better understand effects of seizures
Driving simulators are a safe method of ictal and interictal testing
Different types of seizures may pose different levels of risk to driving
Better evidence will encourage more flexible driving restrictions
Acknowledgments
This work was supported by NIH R01 NS055829 and by the Betsy and Jonathan Blattmachr family.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Gilliam F, Kuzniecky R, Faught E, Black L, Carpenter G, Schrodt R. Patient-validated content of epilepsy-specific quality-of-life measurement. Epilepsia. 1997;38:233–6. doi: 10.1111/j.1528-1157.1997.tb01102.x. [DOI] [PubMed] [Google Scholar]
- 2.Pulliainen V, Kuikka P, Jokelainen M. Motor and cognitive functions in newly diagnosed adult seizure patients before antiepileptic medication. Acta Neurol Scand. 2000;101:73–8. doi: 10.1034/j.1600-0404.2000.101002073.x. [DOI] [PubMed] [Google Scholar]
- 3.Kwan P, Brodie MJ. Neuropsychological effects of epilepsy and antiepileptic drugs. Lancet. 2001;357:216–22. doi: 10.1016/S0140-6736(00)03600-X. [DOI] [PubMed] [Google Scholar]
- 4.Karceski SC. Seizure medications and their side effects. Neurology. 2007;69:E27–9. doi: 10.1212/01.wnl.0000296051.34044.07. [DOI] [PubMed] [Google Scholar]
- 5.Classen S, Crizzle AM, Winter SM, Silver W, Eisenschenk S. Evidence-based review on epilepsy and driving. Epilepsy Behav. 2012;23:103–12. doi: 10.1016/j.yebeh.2011.11.015. [DOI] [PubMed] [Google Scholar]
- 6.Waller JA. Chronic medical conditions and traffic safety: review of the California experience. N Engl J Med. 1965;273:1413–20. doi: 10.1056/NEJM196512232732605. [DOI] [PubMed] [Google Scholar]
- 7.Vernon DD, Diller EM, Cook LJ, Reading JC, Suruda AJ, Dean JM. Evaluating the crash and citation rates of Utah drivers licensed with medical conditions, 1992–1996. Accid Anal Prev. 2002;34:237–46. doi: 10.1016/s0001-4575(01)00019-7. [DOI] [PubMed] [Google Scholar]
- 8.Popkin CL, Waller PF. Epilepsy and driving in North Carolina: an exploratory study. Accid Anal Prev. 1989;21:389–93. doi: 10.1016/0001-4575(89)90032-8. [DOI] [PubMed] [Google Scholar]
- 9.Lings S. Increased driving accident frequency in Danish patients with epilepsy. Neurology. 2001;57:435–9. doi: 10.1212/wnl.57.3.435. [DOI] [PubMed] [Google Scholar]
- 10.Davis TG, Wehling EH, Carpenter RL. Oklahoma’s medically restricted drivers. A study of selected medical conditions. J Okla State Med Assoc. 1973;66:322–7. [PubMed] [Google Scholar]
- 11.Hansotia P, Broste SK. The effect of epilepsy or diabetes mellitus on the risk of automobile accidents. N Engl J Med. 1991;324:22–6. doi: 10.1056/NEJM199101033240105. [DOI] [PubMed] [Google Scholar]
- 12.Crancer AML. Accident and Violation Rates of Washington’s Medically Restricted Drivers. JAMA. 1968;205:272–276. [Google Scholar]
- 13.Taylor J, Chadwick D, Johnson T. Risk of accidents in drivers with epilepsy. J Neurol Neurosurg Psychiatry. 1996;60:621–7. doi: 10.1136/jnnp.60.6.621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Beaussart M, Beaussart-Defaye J, Lamiaux JM, Grubar JC. Epileptic drivers--a study of 1,089 patients. Med Law. 1997;16:295–306. [PubMed] [Google Scholar]
- 15.Bener A, Murdoch JC, Achan NV, Karama AH, Sztriha L. The effect of epilepsy on road traffic accidents and casualties. Seizure. 1996;5:215–9. doi: 10.1016/s1059-1311(96)80039-2. [DOI] [PubMed] [Google Scholar]
- 16.Sheth SG, Krauss G, Krumholz A, Li G. Mortality in epilepsy: driving fatalities vs other causes of death in patients with epilepsy. Neurology. 2004;63:1002–7. doi: 10.1212/01.wnl.0000138590.00074.9a. [DOI] [PubMed] [Google Scholar]
- 17.Evidence Report: Seizure Disorders and Commercial Motor Vehicle Safety (Comprehensive Review). Presented to Federal Motor Carrier Safety Administration; 2007. [Google Scholar]
- 18.Berg AT, Vickrey BG, Sperling MR, Langfitt JT, Bazil CW, Shinnar S, Walczak TS, Pacia S, Spencer SS. Driving in adults with refractory localization-related epilepsy. Multi-Center Study of Epilepsy Surgery. Neurology. 2000;54:625–30. doi: 10.1212/wnl.54.3.625. [DOI] [PubMed] [Google Scholar]
- 19.van der Lugt PJ. Traffic accidents caused by epilepsy. Epilepsia. 1975;16:747–51. doi: 10.1111/j.1528-1157.1975.tb04760.x. [DOI] [PubMed] [Google Scholar]
- 20.Krumholz A. Driving issues in epilepsy: past, present, and future. Epilepsy Curr. 2009;9:31–5. doi: 10.1111/j.1535-7511.2008.01283.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gastaut H, Zifkin BG. The risk of automobile accidents with seizures occurring while driving: relation to seizure type. Neurology. 1987;37:1613–6. doi: 10.1212/wnl.37.10.1613. [DOI] [PubMed] [Google Scholar]
- 22.Krauss GL, Krumholz A, Carter RC, Li G, Kaplan P. Risk factors for seizure-related motor vehicle crashes in patients with epilepsy. Neurology. 1999;52:1324–9. doi: 10.1212/wnl.52.7.1324. [DOI] [PubMed] [Google Scholar]
- 23.Hoppe C, Poepel A, Elger CE. Epilepsy: accuracy of patient seizure counts. Arch Neurol. 2007;64:1595–9. doi: 10.1001/archneur.64.11.1595. [DOI] [PubMed] [Google Scholar]
- 24.Krauss GL, Ampaw L, Krumholz A. Individual state driving restrictions for people with epilepsy in the US. Neurology. 2001;57:1780–5. doi: 10.1212/wnl.57.10.1780. [DOI] [PubMed] [Google Scholar]
- 25.Drazkowski JF, Fisher RS, Sirven JI, Demaerschalk BM, Uber-Zak L, Hentz JG, Labiner D. Seizure-related motor vehicle crashes in Arizona before and after reducing the driving restriction from 12 to 3 months. Mayo Clin Proc. 2003;78:819–25. doi: 10.4065/78.7.819. [DOI] [PubMed] [Google Scholar]
- 26.Driving laws by state. Epilepsy Foundation; [Google Scholar]
- 27.Ooi WW, Gutrecht JA. International regulations for automobile driving and epilepsy. J Travel Med. 2000;7:1–4. doi: 10.2310/7060.2000.00001. [DOI] [PubMed] [Google Scholar]
- 28.Vickrey BG, Berg AT, Sperling MR, Shinnar S, Langfitt JT, Bazil CW, Walczak TS, Pacia S, Kim S, Spencer SS. Relationships between seizure severity and health-related quality of life in refractory localization-related epilepsy. Epilepsia. 2000;41:760–4. doi: 10.1111/j.1528-1157.2000.tb00239.x. [DOI] [PubMed] [Google Scholar]
- 29.Blumenfeld H. Impaired consciousness in epilepsy. Lancet Neurol. 2012;11:814–26. doi: 10.1016/S1474-4422(12)70188-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schweizer TA, Kan K, Hung Y, Tam F, Naglie G, Graham SJ. Brain activity during driving with distraction: an immersive fMRI study. Front Hum Neurosci. 2013;7:53. doi: 10.3389/fnhum.2013.00053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Calhoun VD, Pekar JJ, McGinty VB, Adali T, Watson TD, Pearlson GD. Different activation dynamics in multiple neural systems during simulated driving. Hum Brain Mapp. 2002;16:158–67. doi: 10.1002/hbm.10032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Spiers HJ, Maguire EA. Neural substrates of driving behaviour. Neuroimage. 2007;36:245–55. doi: 10.1016/j.neuroimage.2007.02.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.McPherson A, Rojas L, Bauerschmidt A, Ezeani CC, Yang L, Motelow JE, Farooque P, Detyniecki K, Giacino JT, Blumenfeld H. Testing for minimal consciousness in complex partial and generalized tonic-clonic seizures. Epilepsia. 2012;53:e180–3. doi: 10.1111/j.1528-1167.2012.03657.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bauerschmidt A, Koshkelashvili N, Ezeani CC, Yoo JY, Zhang Y, Manganas LN, Kapadia K, Palenzuela D, Schmidt CC, Lief R, Kiely BT, Choezom T, McClurkin M, Shorten A, Detyniecki K, Hirsch LJ, Giacino JT, Blumenfeld H. Prospective assessment of ictal behavior using the revised Responsiveness in Epilepsy Scale (RES-II) Epilepsy Behav. 2013;26:25–8. doi: 10.1016/j.yebeh.2012.10.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Enev M, McNally KA, Varghese G, Zubal IG, Ostroff RB, Blumenfeld H. Imaging onset and propagation of ECT-induced seizures. Epilepsia. 2007;48:238–44. doi: 10.1111/j.1528-1167.2007.00919.x. [DOI] [PubMed] [Google Scholar]
- 36.Blumenfeld H, Varghese GI, Purcaro MJ, Motelow JE, Enev M, McNally KA, Levin AR, Hirsch LJ, Tikofsky R, Zubal IG, Paige AL, Spencer SS. Cortical and subcortical networks in human secondarily generalized tonic-clonic seizures. Brain. 2009;132:999–1012. doi: 10.1093/brain/awp028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Blumenfeld H, Westerveld M, Ostroff RB, Vanderhill SD, Freeman J, Necochea A, Uranga P, Tanhehco T, Smith A, Seibyl JP, Stokking R, Studholme C, Spencer SS, Zubal IG. Selective frontal, parietal, and temporal networks in generalized seizures. Neuroimage. 2003;19:1556–66. doi: 10.1016/s1053-8119(03)00204-0. [DOI] [PubMed] [Google Scholar]
- 38.Yang L, Morland TB, Schmits K, Rawson E, Narasimhan P, Motelow JE, Purcaro MJ, Peng K, Raouf S, Desalvo MN, Oh T, Wilkerson J, Bod J, Srinivasan A, Kurashvili P, Anaya J, Manza P, Danielson N, Ransom CB, Huh L, Elrich S, Padin-Rosado J, Naidu Y, Detyniecki K, Hamid H, Farooque P, Astur R, Xiao B, Duckrow RB, Blumenfeld H. A prospective study of loss of consciousness in epilepsy using virtual reality driving simulation and other video games. Epilepsy Behav. 2010;18:238–46. doi: 10.1016/j.yebeh.2010.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Yang L, Shklyar I, Lee HW, Ezeani CC, Anaya J, Balakirsky S, Han X, Enamandram S, Men C, Cheng JY, Nunn A, Mayer T, Francois C, Albrecht M, Hutchison AL, Yap EL, Ing K, Didebulidze G, Xiao B, Hamid H, Farooque P, Detyniecki K, Giacino JT, Blumenfeld H. Impaired consciousness in epilepsy investigated by a prospective responsiveness in epilepsy scale (RES) Epilepsia. 2012;53:437–47. doi: 10.1111/j.1528-1167.2011.03341.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Blumenfeld H, McNally KA, Vanderhill SD, Paige AL, Chung R, Davis K, Norden AD, Stokking R, Studholme C, Novotny EJ, Jr, Zubal IG, Spencer SS. Positive and negative network correlations in temporal lobe epilepsy. Cereb Cortex. 2004;14:892–902. doi: 10.1093/cercor/bhh048. [DOI] [PubMed] [Google Scholar]
- 41.Englot DJ, Modi B, Mishra AM, DeSalvo M, Hyder F, Blumenfeld H. Cortical deactivation induced by subcortical network dysfunction in limbic seizures. J Neurosci. 2009;29:13006–18. doi: 10.1523/JNEUROSCI.3846-09.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Englot DJ, Yang L, Hamid H, Danielson N, Bai X, Marfeo A, Yu L, Gordon A, Purcaro MJ, Motelow JE, Agarwal R, Ellens DJ, Golomb JD, Shamy MC, Zhang H, Carlson C, Doyle W, Devinsky O, Vives K, Spencer DD, Spencer SS, Schevon C, Zaveri HP, Blumenfeld H. Impaired consciousness in temporal lobe seizures: role of cortical slow activity. Brain. 2010;133:3764–77. doi: 10.1093/brain/awq316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Motelow JEGA, Zayyad Z, et al. Brainstem cholinergic and thalamic dysfunction during limbic seizures: possible mechanism for cortical slow oscillations and impaired consciousness. Society for Neuroscience; Washington D.C: 2011. [Google Scholar]
- 44.Blumenfeld H, McCormick DA. Corticothalamic inputs control the pattern of activity generated in thalamocortical networks. J Neurosci. 2000;20:5153–62. doi: 10.1523/JNEUROSCI.20-13-05153.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bai X, Vestal M, Berman R, Negishi M, Spann M, Vega C, Desalvo M, Novotny EJ, Constable RT, Blumenfeld H. Dynamic time course of typical childhood absence seizures: EEG, behavior, and functional magnetic resonance imaging. J Neurosci. 2010;30:5884–93. doi: 10.1523/JNEUROSCI.5101-09.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Berman R, Negishi M, Vestal M, Spann M, Chung MH, Bai X, Purcaro M, Motelow JE, Danielson N, Dix-Cooper L, Enev M, Novotny EJ, Constable RT, Blumenfeld H. Simultaneous EEG, fMRI, and behavior in typical childhood absence seizures. Epilepsia. 2010;51:2011–22. doi: 10.1111/j.1528-1167.2010.02652.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Arthuis M, Valton L, Regis J, Chauvel P, Wendling F, Naccache L, Bernard C, Bartolomei F. Impaired consciousness during temporal lobe seizures is related to increased long-distance cortical-subcortical synchronization. Brain. 2009;132:2091–101. doi: 10.1093/brain/awp086. [DOI] [PubMed] [Google Scholar]
- 48.Bell WL, Park YD, Thompson EA, Radtke RA. Ictal cognitive assessment of partial seizures and pseudoseizures. Arch Neurol. 1998;55:1456–9. doi: 10.1001/archneur.55.11.1456. [DOI] [PubMed] [Google Scholar]
- 49.Profitlich T, Hoppe C, Reuber M, Helmstaedter C, Bauer J. Ictal neuropsychological findings in focal nonconvulsive status epilepticus. Epilepsy Behav. 2008;12:269–75. doi: 10.1016/j.yebeh.2007.10.011. [DOI] [PubMed] [Google Scholar]
- 50.Lux S, Kurthen M, Helmstaedter C, Hartje W, Reuber M, Elger CE. The localizing value of ictal consciousness and its constituent functions: a video-EEG study in patients with focal epilepsy. Brain. 2002;125:2691–8. doi: 10.1093/brain/awf276. [DOI] [PubMed] [Google Scholar]
- 51.Cavanna AE, Mula M, Servo S, Strigaro G, Tota G, Barbagli D, Collimedaglia L, Viana M, Cantello R, Monaco F. Measuring the level and content of consciousness during epileptic seizures: the Ictal Consciousness Inventory. Epilepsy Behav. 2008;13:184–8. doi: 10.1016/j.yebeh.2008.01.009. [DOI] [PubMed] [Google Scholar]
- 52.Inoue Y, Mihara T. Awareness and responsiveness during partial seizures. Epilepsia. 1998;39 (Suppl 5):7–10. doi: 10.1111/j.1528-1157.1998.tb05142.x. [DOI] [PubMed] [Google Scholar]
- 53.Johanson M, Valli K, Revonsuo A. How to assess ictal consciousness? Behav Neurol. 2011;24:11–20. doi: 10.3233/BEN-2011-0316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Monaco F, Mula M, Cavanna AE. Consciousness, epilepsy, and emotional qualia. Epilepsy Behav. 2005;7:150–60. doi: 10.1016/j.yebeh.2005.05.018. [DOI] [PubMed] [Google Scholar]
- 55.Biederman J, Fried R, Monuteaux MC, Reimer B, Coughlin JF, Surman CB, Aleardi M, Dougherty M, Schoenfeld S, Spencer TJ, Faraone SV. A laboratory driving simulation for assessment of driving behavior in adults with ADHD: a controlled study. Ann Gen Psychiatry. 2007;6:4. doi: 10.1186/1744-859X-6-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Carvalho KN, Pearlson GD, Astur RS, Calhoun VD. Simulated driving and brain imaging: combining behavior, brain activity, and virtual reality. CNS Spectr. 2006;11:52–62. doi: 10.1017/s1092852900024214. [DOI] [PubMed] [Google Scholar]
- 57.Crizzle AM, Classen S, LaFranca C, Winter SM, Roper SN, Eisenschenk S. Assessing the driving performance of a person with epilepsy presurgery and postsurgery. Am J Occup Ther. 2013;67:e24–9. doi: 10.5014/ajot.2013.006569. [DOI] [PubMed] [Google Scholar]
- 58.Crizzle AM, Classen S, Winter SM, Silver W, LaFranca C, Eisenschenk S. Associations between clinical tests and simulated driving performance in persons with epilepsy. Epilepsy Behav. 2012;23:241–6. doi: 10.1016/j.yebeh.2011.12.019. [DOI] [PubMed] [Google Scholar]
- 59.Ghosh D, Jamson SL, Baxter PD, Elliott MW. Continuous measures of driving performance on an advanced office-based driving simulator can be used to predict simulator task failure in patients with obstructive sleep apnoea syndrome. Thorax. 2012;67:815–21. doi: 10.1136/thoraxjnl-2011-200699. [DOI] [PubMed] [Google Scholar]
- 60.Krestel HE, Nirkko A, von Allmen A, Liechti C, Wettstein J, Mosbacher A, Mathis J. Spike-triggered reaction-time EEG as a possible assessment tool for driving ability. Epilepsia. 2011;52:e126–9. doi: 10.1111/j.1528-1167.2011.03252.x. [DOI] [PubMed] [Google Scholar]
- 61.Meda SA, Calhoun VD, Astur RS, Turner BM, Ruopp K, Pearlson GD. Alcohol dose effects on brain circuits during simulated driving: an fMRI study. Hum Brain Mapp. 2009;30:1257–70. doi: 10.1002/hbm.20591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Reimer B, D’Ambrosio LA, Coughlin JE, Kafrissen ME, Biederman J. Using self-reported data to assess the validity of driving simulation data. Behav Res Methods. 2006;38:314–24. doi: 10.3758/bf03192783. [DOI] [PubMed] [Google Scholar]
- 63.Shechtman O, Classen S, Awadzi K, Mann W. Comparison of driving errors between on-the-road and simulated driving assessment: a validation study. Traffic Inj Prev. 2009;10:379–85. doi: 10.1080/15389580902894989. [DOI] [PubMed] [Google Scholar]
- 64.Stein AC, Dubinsky RM. Driving simulator performance in patients with possible and probable Alzheimer’s disease. Ann Adv Automot Med. 2011;55:325–34. [PMC free article] [PubMed] [Google Scholar]
- 65.Vakulin A, Baulk SD, Catcheside PG, Antic NA, van den Heuvel CJ, Dorrian J, McEvoy RD. Driving simulator performance remains impaired in patients with severe OSA after CPAP treatment. J Clin Sleep Med. 2011;7:246–53. doi: 10.5664/JCSM.1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Calhoun VD, Pearlson GD. A selective review of simulated driving studies: Combining naturalistic and hybrid paradigms, analysis approaches, and future directions. Neuroimage. 2012;59:25–35. doi: 10.1016/j.neuroimage.2011.06.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Chan E, Pradhan AK, Pollatsek A, Knodler MA, Fisher DL. Are Driving Simulators Effective Tools for Evaluating Novice Drivers’ Hazard Anticipation, Speed Management, and Attention Maintenance Skills. Transp Res Part F Traffic Psychol Behav. 2010;13:343–353. doi: 10.1016/j.trf.2010.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Tatum WO, Worley AV, Selenica ML. Disobedience and driving in patients with epilepsy. Epilepsy Behav. 2012;23:30–5. doi: 10.1016/j.yebeh.2011.10.015. [DOI] [PubMed] [Google Scholar]
- 69.Bautista RE, Wludyka P. Driving prevalence and factors associated with driving among patients with epilepsy. Epilepsy Behav. 2006;9:625–31. doi: 10.1016/j.yebeh.2006.08.020. [DOI] [PubMed] [Google Scholar]
- 70.Blumenfeld H. Neuroanatomy through clinical cases. 2. Sunderland, Mass: Sinauer Associates; 2010. [Google Scholar]