

Abstract
Context:
There is a paucity of published telepsychiatry results in India.
Aims:
This study was conducted to assess the feasibility of asynchronous telepsychiatry and to study the referral patterns.
Settings and Design:
This study was conducted in the telemedicine unit of a tertiary care center and design was retrospective analysis of 94 cases, which were diagnosed and treated by telepsychiatry.
Materials and Methods:
All 94 patients who were referred between January 2007 and August 2013 for telepsychiatry consultations were retrospectively analyzed to assess the referral pattern and feasibility.
Statistical Analysis Used:
Comparisons between demographic parameters and psychiatric diagnosis was done using Chi-square test.
Results:
In 89 out of 94 (95%) patients it was possible to make a definitive diagnosis and recommend appropriate treatment only on the basis of data received from the primary care physician by telepsychiatry. This indicates the feasibility of telepsychiatry. The most common problems for which referrals were made included schizophrenia and other psychotic disorders, mood disorders and substance related disorders.
Conclusions:
This study demonstrates the feasibility of Asynchronous telepsychiatry. Additional Indian studies should be conducted to build the evidence base for the best use of asynchronous telepsychiatry.
Keywords: Asynchronous, India, telepsychiatry
INTRODUCTION
India is geographically large with many towns and villages located in remote rural areas, where few medical facilities exist.[1] Telemedicine uses information and communication technologies (ICT) to overcome geographical barriers and increase access to health care services.[2] Telepsychiatry (E-mental health/telemental health) is the use of ICT to provide mental health services.[3] Overall, there are two main types of communication technologies:
Synchronous or interactive-provides live, two-way interactive transmission between patient and provider at distant locations via telephony, online communication (e.g., chat forums) and video-conferencing,
Asynchronous or store-and-forward-involves acquiring medical data and then transmitting this clinical information in the form of data, audio, video clips, or recordings via E-mail or Web applications for later review by a specialist.[3]
According to the second global eHealth survey by World Health Organization, 2009, the store-and-forward approach is the least commonly reported in telepsychiatry, in comparison to teleradiology, telepathology and teledermatology.[2] This study was done to assess the feasibility of asynchronous telepsychiatry and to study the referral pattern.
MATERIALS AND METHODS
Under the banner of National Rural Health Mission, Telemedicine is one of the key initiatives to improve the health services for the rural people of India. The Maharashtra State Telemedicine project (operationalized in the year 2007) is a part of larger initiative undertaken by Government of India and World Health Organization. It uses dedicated lease lines of fiber optic cables having a high bandwidth capacity. From the six specialist telemedicine centers (KEM Hospital Mumbai, B. J. Medical College Pune, GMC Aurangabad, GMC Nagpur, Sir J. J. Hospital Mumbai, Nanavati Hospital Mumbai), medical consultations (asynchronous and synchronous) are given to primary care physicians attached to 27 district and four sub district hospitals of Maharashtra. An Electronic Health Record is generated for each patient and is archived in digital format.[4] In the center under study, due to the non-availability of synchronous timeframes between the primary care physician and psychiatrist, asynchronous communication was the preferred mode of referral. The primary care physicians made the psychiatric referrals by E-mailing the psychiatric findings and general examination notes of the patient. Investigation reports if available were scanned and E-mailed. The psychiatrist reviewed the clinical information provided and E-mailed an opinion of psychiatric diagnosis according to Diagnostic and Statistical Manual of Mental Disorders-IV-text revision and management suggestions. After obtaining approval from the Institution Ethics Committee, the data of psychiatric referrals from January 2007 to August 2013 was collected. The parameters assessed were gender, age, marital status, religion and the psychiatric diagnostic profile. Data is expressed as mean with standard deviation and percentages. Comparisons were made using Chi-square test. A value of P < 0.05 was considered to be statistically significant. Graphpad software, 2013 was used to find the P value.
RESULTS
In all, 492 psychiatric referrals were made between January 2007 and August 2013 from all the district and sub-district hospitals of Maharashtra to the six specialist telemedicine centers of which 94 referrals were made to our center.
Demographic profile
Age of the patients ranged from 6 years to 69 years (mean 35.18 + 15.37). The male to female ratio was around 1.76:1.
Diagnostic profile
The psychiatric diagnostic profile of patients was as shown in Table 1.
Table 1.
Psychiatric diagnostic profile of patients, 89 (z95%)
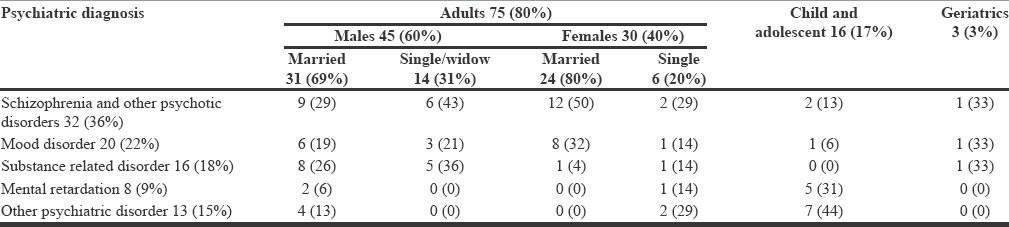
Over all, out of 94 patients, Axis III disorder was present in seven patients (8%). Comorbidity was present in six patients (6%) and in five patients (5%) a definite psychiatric diagnosis could not be made due to inadequate history and differential diagnoses were offered. Males (in all age groups) were referred significantly more compared with females (χ2 = 4.67, df = 1, P = 0.0307). Substance dependence was significantly more common in males (χ2 = 6.76, df = 1, P = 0.0093).
DISCUSSION
World Health Organization's eHealth resolution adopted in 2005,[2,5] focuses on strengthening health systems in countries through the use of eHealth; building public-private partnerships in ICT development and deployment for health; supporting capacity building for the application of eHealth in Member States; and the development and adoption of standards. The chief objectives of the National Mental Health Program[6,7] are to ensure the availability and accessibility of minimum mental healthcare for all in the foreseeable future, particularly to the most vulnerable and underprivileged sections of the population and to apply mental health knowledge in general health care and in social development. Telepsychiatry holds promise to further such objectives. Of the two types of communication technologies, the literature has focused more on video-conferencing (synchronous) as a mode of communication.[7] Synchronous telepsychiatry requires additional infrastructure, funds and synchronous presence of psychiatrist. In developing nation like ours, where there is already a dearth of mental health professionals, burdening the existing manpower to provide such services might prove to be counterproductive.[7] Store-and-forward approaches are the most formalized initiatives; they are relatively simple to implement, require basic infrastructure and are generally not disruptive to traditional workflows of health professionals and patients.[2] There is limited literature available about telepsychiatry units functioning in India.[8] In the present study, out of 94 non-emergency referrals 89 patients (95%) received a definite psychiatric diagnosis. This demonstrates that asynchronous telepsychiatry is possible. Yellowlees et al., in an article in 2010[9] conducted psychiatric consultations using asynchronous, video based telepsychiatry and concluded that it is feasible. In this study majority were males (60 out of 94, 64%), married (57 out of 78, 73%) and 76% (68 out of 89) diagnoses included schizophrenia and other psychotic disorders, mood disorders and substance related disorders. The demographic and diagnostic profile of this sample was consistent with routine psychiatry out-patient sample.[10] In other telepsychiatry studies, more female patients were present (55.34%,[8] 67%[9]). In an Indian study, the telepsychiatry diagnoses made were schizophrenia (36%), other psychosis (11%), bipolar (9%)[8] while in a western study the telepsychiatry diagnosis were mood disorders −85%, substance use disorders −32%, anxiety disorders −53% and other axis I diagnoses −5%.[9] In the present study, anxiety disorder was present in two patients (2%). Experiences with telemedicine in India could have far-reaching benefits for poorer communities in developed countries as well as for developing countries.[1] The importance of evaluation within the field of telemedicine cannot be overstated: the field is in its infancy and while its promise is great, evaluation can ensure maximization of benefit.[2] Rigorous evaluations of telemedicine initiatives are required to generate reliable data for use by policy-makers to create and shape national telemedicine policy and strategies.[2] Limitations of the study include:
Small sample,
A cross sectional study,
No assessment of the patients and the primary care physician's satisfaction,
No assessment of cost-effectiveness.
ACKNOWLEDGMENT
The authors are thankful to Sayed Mahedi (State coordinator, Telemedicine, Sir JJ Hospital) and Priyanka D. Kamble (Facility Manager, Telemedicine, Sir JJ Hospital for their cooperation and assistance.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Pal A, Mbarika VW, Cobb-Payton F, Datta P, McCoy S. Telemedicine diffusion in a developing country: the case of India (March 2004) IEEE Trans Inf Technol Biomed. 2005;9:59–65. doi: 10.1109/titb.2004.842410. [DOI] [PubMed] [Google Scholar]
- 2.WHO Library Cataloguing-in-Publication Data. World Health Organization; 2010. [Last accessed on 2013 Oct 26]. Telemedicine: opportunities and Developments in Member States: report on the Second Global Survey on eHealth 2009 (Global Observatory for eHealth Series 2) Available from: http://www.who.int/goe/publications/goe_telemedicine_2010.pdf . [Google Scholar]
- 3.Melaka A, Edirippulige S. Psych-technology: A systematic review of the telepsychiatry literature. Telepsychiatry appendices. 2009. [Last accessed on 2013 Jan 13]. Available from: http://www.priory.com/psychiatry/telepsychiatry.htm .
- 4.Kumar R, Choudhary PK, Pasha SM. Telemedicine in the state of Maharashtra: A case study. CSI Communications. 2012. [Last accessed on 2013 Oct 23]. pp. 24–6. Available from: http://www.csi-india.org .
- 5.Geneva: 2005. May 16-25, [Last accessed on 2014 Jan 6]. Resolution WHA58. 28. eHealth. In: Fifty-eighth World Health Assembly. Available from: http://www.apps.who.int/iris/bitstream/10665/20378/1/WHA58_28-en.pdf . [Google Scholar]
- 6.New Delhi: Ministry of Health and Family Welfare, Government of India; 1982. Directorate General of Health Services (DGHS). National Mental Health Programme for India. [Google Scholar]
- 7.Malhotra S, Chakrabarti S, Shah R. Telepsychiatry: Promise, potential, and challenges. Indian J Psychiatry. 2013;55:3–11. doi: 10.4103/0019-5545.105499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thara R, John S, Rao K. Telepsychiatry in Chennai, India: The SCARF experience. Behav Sci Law. 2008;26:315–22. doi: 10.1002/bsl.816. [DOI] [PubMed] [Google Scholar]
- 9.Yellowlees PM, Odor A, Parish MB, Iosif AM, Haught K, Hilty D. A feasibility study of the use of asynchronous telepsychiatry for psychiatric consultations. Psychiatr Serv. 2010;61:838–40. doi: 10.1176/ps.2010.61.8.838. [DOI] [PubMed] [Google Scholar]
- 10.Nayak S, Sonaliya KN. Morbidity patterns of patients attending psychiatry OPD in tertiary care hospital in Ahmedabad. Natl J Med Res. 2011;1:7–9. [Google Scholar]