

Abstract
Lithium has been the gold standard drug for bipolar disorders. The efficacy of lithium is dose-dependent and reliably correlates with that of serum lithium levels (trough levels). Trough levels are best measured when tested just before the next dose. In clinical practice, when lithium was administered in divided doses, trough levels were measured at 12 h after the last dose. Does this practice of 12 h lithium estimation apply to once a day (OD) administration of lithium also? This study was undertaken to test this hypothesis. Serum lithium levels were measured at 12 and 24 h post the last dose in 48 patients taking an OD dosing of sustained preparations of lithium. The mean and (standard deviation) of serum lithium levels at 12 h (0.82 [0.29]) and at 24 h (0.60 [0.20]) were calculated. The serum lithium level at 12 h was 1.3 times higher than that of the 24 h levels (actual trough levels). Thus, it seems appropriate to estimate the serum lithium levels (trough levels) at 24 h post the last dose in patients taking lithium as an OD dosage, which may prevent patient maintained on a lower than required dose of lithium.
Keywords: Lithium, once a day dose, therapeutic level, trough values
A study to determine appropriate time for serum level estimation for once a day administration of lithium
INTRODUCTION
Lithium has been the gold standard drug for treatment in bipolar disorder. It was administered as thrice daily with standard preparation; later twice daily with the availability of sustained release preparations. The efficacy of lithium is dose-dependent and reliably correlates with serum concentrations. Therapeutic efficacy of lithium demands maintenance of serum concentrations in the range of 0.8 and 1.2 mmol/L (trough level).[1] Lower levels are considered to be noneffective, and serum level above this range would lead to side-effects and toxicity. Amdisen[2] proposed the use of a standardized 12 h serum lithium concentration, which subsequently became the universally accepted mode of monitoring lithium levels in patients who have been taking the drug in two or more divided dosages with standard preparations where the last dose would be administered at bed time. It is convenient for the patient to provide a blood sample to check the trough levels before the next morning dose. However, in the current day, clinical practice once a day (OD) dose is being prescribed for reasons of better compliance.[3] The current practice is to measure serum lithium levels at 12 h after the last dosing, irrespective of BD/OD administration.
Now the clinical question is whether this standardized 12 h serum level estimation indicates true trough level when lithium is administered as OD dosage. If not, would it lead to misleading clinical decisions in estimating the correct dose of lithium and also erroneous interpretations of lithium nonresponse? The current study is undertaken to test this hypothesis! To the best of our knowledge, this would be the first study to be published in the literature to determine the appropriate time for serum lithium level estimation for OD administration of sustained release preparations of lithium.
METHODS AND RESULTS
We present the results of a cross sectional study which involves analyzing serum lithium levels in bipolar disorder patients compliant with sustained release preparation of lithium. The dose was administered at 8 pm and blood samples were collected at 12 and 24 h after the last dose, at 8 am and 8 pm on the next day (medication is obtained from a single manufacturer and serum level estimation of lithium was done in a single laboratories). The results were analyzed using standard statistical techniques.
We found that serum lithium levels after 12 h (μ = 0.82, σ = 0.29) was 1.3 times higher than the 24 h levels (μ = 0.6, σ = 0.20) after an OD dose [Table 1 and Figure 1].
Table 1.
Serum lithium levels at 12 h and 24 h post an OD dose of sustained preparation of lithium
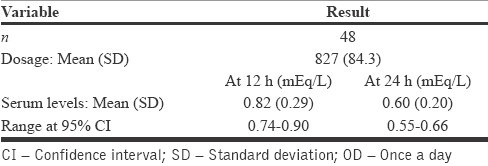
Figure 1.
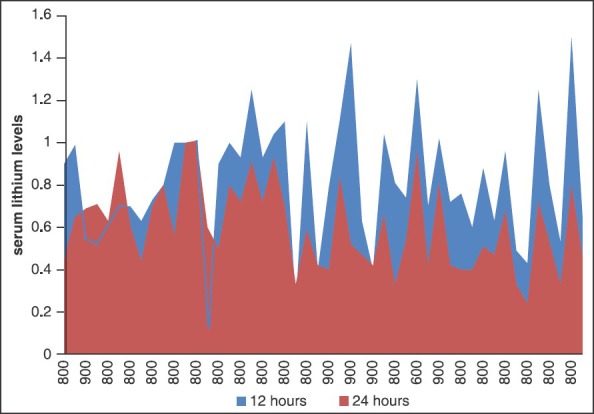
Chart depicting the individual subject's serum lithium level at 12 and 24 h postdose
DISCUSSION
In contrast to the usual practice of measuring serum lithium levels at 12 h irrespective of the dosing pattern, it is observed that measuring at 24 h is recommended, which provides an accurate trough value for patients on OD dosage. Measuring serum lithium levels at 12 h in case of OD dosing would give 1.3 times higher value than the actual trough value, leading to probable erroneous assumption, maintaining the patient on a lesser than required lithium doses, which in turn may lead to conclusions of patient being a lithium nonresponder.
The recent years have witnessed a disturbing trend of decline in use of lithium as mood stabilizer, surprisingly uniformly in all the centers. Of several reasons cited, one being relatively more nonresponsiveness to lithium. Does our practice of testing serum lithium levels at 12 h (not measuring the true trough level) after the last dose in case of OD dosing contributes to it to an extent?
Lithium is generally prescribed in the nights, it might be inconvenient for the patient to test serum lithium levels at 24 h post the last dose, late evening hours. The alternative approach to circumvent this problem is by administrating lithium in the morning as it is a nonsedative drug. If the dosing is still preferred at nights, we can still do a serum lithium estimation at 12 h post the last dose, but deduce the level by 1.3 times to calculate the actual trough level (at 24 h).
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Jefferson JW, Greist JH. New Delhi: Wolters Kluwer (India) Pvt. Ltd; 2009. Lithium. Kaplan and Saddock's Comprehensive Text Book of Psychiatry. [Google Scholar]
- 2.Amdisen A. Clinical and serum-level monitoring in lithium therapy and lithium intoxication. J Anal Toxicol. 1978;2:193–202. [Google Scholar]
- 3.Mohan R, Suresh KP, Prasad KM, Ashok MV, Andrade C, Sreenivas KN, et al. Once daily lithium in the prophylaxis of mood disorders. Indian J Psychiatry. 1996;38:104–8. [PMC free article] [PubMed] [Google Scholar]