

Sir,
Divalproex sodium extended release (ER) preparations received Food and Drug Administration approval as monotherapy for management of acute mania in 2005.[1] It is intended for once daily (OD) oral administration and maintains a steady state plasma concentration for 24 h.[2] The therapeutic range is maintained through controlling its release. Therapeutic efficacy is associated with a trough level concentration between 50 and 100 mmol/L (trough levels). Though it does not have a narrow therapeutic range as in the case of lithium, accurate estimation of its trough level is essential as any value below the lower limit of the therapeutic range is not effective and above it may result in adverse effects.[3] Trough levels are more accurate when measured just before the next dose. After a once-daily divalproex-ER dose, the timing of the blood sample does matter and impacts the proper interpretation of the valproic acid (VPA) concentration. There is no one consensus that we depend upon for an optimal time to estimate the trough levels, which impacts the proper interpretation of the VPA concentration. In general, when taking divalproex-ER once daily in the morning, a blood sample collected at 21-24 h after OD dose of ER preparation is expected to have a concentration within 3% of the trough value. Conversely, blood sample 12-15 h after the last dosing will give a value that is 18-25% higher, than the actual trough value.[2] The current study is undertaken with an aim to provide with an appropriate time for serum VPA level estimation (for trough levels) after a single dose of divalproex sodium ER.
This cross-sectional study involves analyzing serum VPA levels in patients with bipolar disorder compliant with ER preparations of divalproex sodium. The dose was administered at 8 pm and blood samples were collected at 12 and 24 h after the last dose (medication is obtained from a single manufacturer and analysis was done in a single lab). The results were analyzed using standard statistical techniques. Mean and standard deviation [Table 1] was calculated for the serum VPA levels at 12 h and at 24 h.
Table 1.
Serum VPA levels at 12 h and 24 h post an OD dose of extended release preparation of divalproex sodium
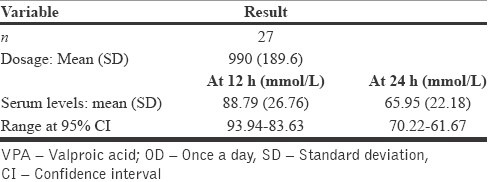
Serum VPA levels after 12 h (μ = 88.9, σ = 26.8) was 1.3 times higher than the 24 h levels (μ = 66, σ = 22.1) after an OD dose [Figure 1].
Figure 1.
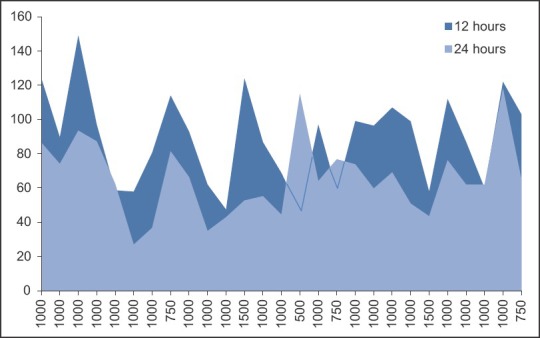
Chart depicting the individual subject's serum valproic acid levels at 12 and 24 h
It is observed that measuring serum VPA levels at 24 h is recommended and provides a more accurate value for patients on OD dosage. Measuring it at 12 h in case of OD dosing would give a 1.3 times higher value than the actual trough value. Trough sampling is easily achieved just before a morning daily dose, but the issue arises when patient receives a night dose, because collecting a blood sample 21-24 h later may be limited by the operational hours of laboratory. To avoid patients’ inconvenience, serum VPA levels can be tested at 12 h though have to be reduced by 1.3 times to calculate the accurate trough levels.
REFERENCES
- 1.Centorrino F, Kelleher JP, Berry JM, Salvatore P, Eakin M, Fogarty KV, et al. Pilot comparison of extended-release and standard preparations of divalproex sodium in patients with bipolar and schizoaffective disorders. Am J Psychiatry. 2003;160:1348–50. doi: 10.1176/appi.ajp.160.7.1348. [DOI] [PubMed] [Google Scholar]
- 2.Reed RC, Dutta S. Does it really matter when a blood sample for valproic acid concentration is taken following once-daily administration of divalproex-ER? Ther Drug Monit. 2006;28:413–8. doi: 10.1097/01.ftd.0000211814.12311.3f. [DOI] [PubMed] [Google Scholar]
- 3.Ghaemi SN. 2nd ed. New Delhi, Philadelphia: Lippincott Williams and Wilkins, Wolters Kluwer Pvt. Ltd; 2009. Mood Disorders; A Practical Guide. [Google Scholar]