

Abstract
We report an unusual case of a giant primary retroperitoneal mature cystic teratoma in right adrenal region in a 39-year-old Chinese female. The patient has complained of dizziness and a high blood pressure approximately 170/110 mmHg for half one year. A plain helical and enhanced CT scan showed a huge tumor with a mixing density in recessus hepatorenalis. This tumor had calcification and fat, as well as a mild enhancement in part of the tumor. The patient was successfully treated with a right surgical resection of the mass. Although the primary retroperitoneal mature cystic teratomas in right adrenal regions are extremely rare, we should pay attention to it and close follow up is indispensable on account of the incidence of malignant transformation is approximately 3-6%.
Keywords: Mature cystic teratoma, primary retroperitoneal, adrenal region
Introduction
Teratoma is a germ cell tumor which is derived from totipotential cells and originated from more than 1 and usually all 3 of the primordial germ cells. Primary teratomas in the retroperitoneum are very rare, especially present as a primary mature cystic teratoma in adrenal region [1]. We report a case with a huge size and unusual origination.
Case presentation
A 39-year-old woman from Anhui province in China was referred to our hospital for further examination and treatment after a elementary diagnoses of retroperitoneal mass in the local hospital. She began to feel dizzy and was measured a high blood pressure for approximately 170/110 mmHg half one year ago. However, she didn’t take sufficient attention about that until a computed tomography (CT) scan showing the huge mass.
She did not appear ill at physical examination, even though the arterial blood pressure was 170/130 mmHg when hospitalizing. A global lump palpation was disclosed at abdominal palpation, with a duller tenderness on the right. No more physical findings were observed.
A plain helical and enhanced CT scan showed a huge tumor with a mixing density in recessus hepatorenalis (Figure 1). This tumor had calcification and fat, as well as a mild enhancement in part of the tumor. There was no evidence of distant metastasis, and normal ovaries were identified. The surrounding tissues were constricted, in particular the dexter lobi hepatis and the right kidney. So we take a kidney emission computed tomography (ECT) to detect the function of the kidneys. The glomerular filtration rate (GFR) of the left kidney was 42.6 ml/min, whereas the right was kidney 24.9 ml/min.
Figure 1.

CT showed the encapsulated, cystic tumor located between the dexter lobi hepatis and the right kidney, with a mixing density of calcification and fat, as well as a mild enhancement in part of the tumor. The liver and the right kidney were compressed seriously.
Results of complete blood count and routine biochemistry evaluations, including renal and liver function tests, were normal, though immune index cued that anti-HBs and anti-HBc were positive. Furthermore, some tumor markers, containing serum alpha-fetoprotein (AFP), lactate dehydrogenase (LDH), carcino embryonie antigen (CEA), carbohydrate antigen 125 (CA125), neuron-specific enolase (NSE), carbohydrate antigen 19-9 (CA19-9) etc were examined to exclude possibility that the tumor did not originate from the adrenal gland. The CEA value, 13.6 ng/ml, was only slightly increased (normal range < 5 ng/ml). At the same time, the CA19-9 value, 122.40 U/ml, had a light rise, too (normal range < 34.0 U/ml).
Surgical resection of the mass was carried out. A giant mass was found between the right hepatic lobe and the right kidney. The liver and the right kidney were compressed seriously, and the right adrenal gland was not founded in the operation. The pancreas, spleen, uterus, and ovaries were not infiltrated by the tumor. The tumor measured 22.5×17×7 cm, and weighed 1620 g (Figure 2). Histological and pathological analysis was performed. The diagnosis of a mature cystic teratoma was confirmed without malignant components. The tumor abounded abundant fat deposits and bones, and with a cephalomere in the cystic wall (Figure 3). The postoperative period was uneventful despite of a hypoproteinemia. It was interesting that the patient’s blood pressure returned to normality and the dizziness died away after the operation. And this situation has been sustained for 18 months at the clinical follow-up.
Figure 2.

Photograph of gross specimen shows macroscopic appearance of excised mass with a size of 22.5×17×7 cm.
Figure 3.
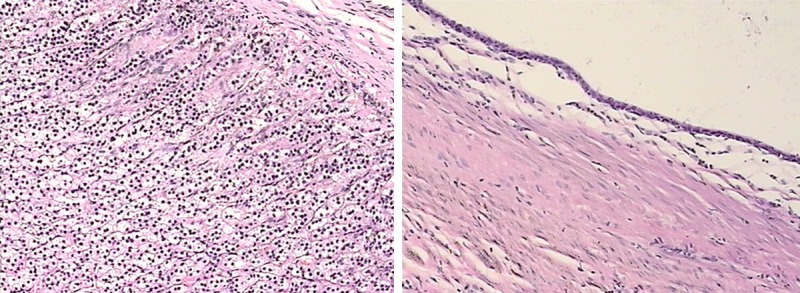
Histopathological findings of the tumor showed that the inside was filled with abundant fat deposits and bones, without malignant components (hematoxylin and eosin staining, ×40).
Summary
Teratoma is a germ cell tumor developing from more than 1 and usually all 3 of the primordial germ cells, which differentiate to different tissues such as skin, muscle, nerve, fat, and tooth structures. etc [2]. Most teratomas are found in the gonads. Extragonadal sites account for 15% of all teratomas, and the retroperitoneum is the least common location [3]. This patient had a retroperitoneal mature cystic teratoma that was not derived from any specific organ. The radiographic examination didn’t recognize the possible origination from ovaries as the nature of the retroperitoneal mass. Because of its relationship to the adrenal gland, and absence of normal adrenal gland, the mass was thought to be a neoplasm arising from the adrenal gland. Another evidence was exhibited that the patient’s blood pressure changed back to normal level after the operation.
The occurrence of retroperitoneal mature cystic teratomas peaks in the first 6 months of infantile and in early adulthood [1]. Only 10% to 20% occur in adults over 30 years old [4]. The left suprarenal location appears to be the predominant location for a retroperitoneal cystic teratoma. And 26% retroperitoneal teratomas are malignant [2], and the rate of malignancy in children is lower than in adults [1]. Although it was a benign tumor, close follow up is indispensable on account of the incidence of malignant transformation is approximately 3-6% [5].
Disclosure of conflict of interest
None.
References
- 1.Gatcombe HG, Assikis V, Kooby D, Johnstone PA. Primary retroperitoneal teratomas: a review of the literature. J Surg Oncol. 2004;86:107–113. doi: 10.1002/jso.20043. [DOI] [PubMed] [Google Scholar]
- 2.Scott AL, Abbassi-Ghadi N, Archer CM, Swamy R, Gupta S. Neuroendocrine carcinoma arising within a retroperitoneal mature teratoma. Ann R Coll Surg Engl. 2010;92:W5–W8. doi: 10.1308/147870810X12699662980952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bedri S, Erfanian K, Schwaitzberg S, Tischler AS. Mature cystic teratoma involving adrenal gland. Endocr Pathol. 2002;13:59–64. doi: 10.1385/ep:13:1:59. [DOI] [PubMed] [Google Scholar]
- 4.Panageas E. General diagnosis case of the day. Primary retroperitoneal teratoma. AJR Am J Roentgenol. 1991;156:1292–1294. doi: 10.2214/ajr.156.6.2028883. [DOI] [PubMed] [Google Scholar]
- 5.Sato F, Mimata H, Mori K. Primary retroperitoneal mature cystic teratoma presenting as an adrenal tumor in an adult. Int J Urol. 2010;17:817. doi: 10.1111/j.1442-2042.2010.02591.x. [DOI] [PubMed] [Google Scholar]