

Abstract
Objectives
The purpose of the analyses was to study development, stability and changes in oral health behaviour; tooth brushing frequency, use of fluoride lozenges and fluoridated tooth paste in children from 1.5 to 5 years of age, and to study associations between oral health behaviour and family characteristics.
Methods
This study was based on data from the Norwegian Mother and Child Cohort Study conducted by the Norwegian Institute of Public Health and data from the Public Dental Services. A total of 771 children were followed from 1.5 to 5 years of age. Questionnaires regarding oral health behaviour in children were completed by the parents three times during preschool age.
Results
More than half of the children (52%) had their teeth brushed twice daily at 1.5 years of age, increasing to 61% at 3 years and 76% at 5 years of age. At 1.5 years of age 37% of the children used fluoride lozenges daily, increasing to 74% at 3 years and 75% at 5 years of age. The majority of the children who had started brushing twice daily and used fluoride lozenges daily at 1.5 year of age continued these behaviours until the age of 5 years. At 1.5 years of age, children who brushed twice daily were more likely to use fluoride lozenges daily than children who brushed less frequently (p = 0.03). Multiple logistic regression showed that the probability of a child having its teeth brushed twice daily continuously during preschool age was higher when both parents were of western origin (OR 4.0, CI 1.3 – 11.9) than when one or both parents were of non-western origin. Children with one older sibling brushed more frequently (OR 1.4, CI 1.0 – 1.9) and used fluoride lozenges more often (OR 1.6, CI 1.1 – 2.2) during preschool age than children without older siblings.
Conclusions
Oral health behaviour established in early life was stable during preschool age. The results indicate that tooth brushing frequency and use of fluoride lozenges were not in accordance with the present recommendations based on the scientific literature. The teeth of Norwegian pre-schoolers were brushed less frequently than recommended, and more children than recommended were using fluoride lozenges.
Keywords: children, fluoride supplement, MoBa, oral health behaviour, tooth brushing
Introduction
Two main strategies to prevent caries in children are to promote tooth brushing and to use fluoride. Tooth brushing twice a day with fluoridated tooth paste has an impact on caries development in preschool children (1, 2). The reported tooth brushing frequencies in preschool children vary; in 2 to 3 year old children, the reported proportion of children brushing at least once a day varies from 17% to 80% (3-6). In a cohort study from Norway, 83% of the children had their teeth brushed regularly at 18 and 36 months of age (7). In 4 to 6 year old children, nearly 95% have been reported to brush at least once a day (8, 9), and 73% to 88% twice a day or more often (5, 10). Ages of the studied children and the reported tooth brushing frequency (once a day or twice a day) differ in these studies. Few studies follow the development of oral health behaviour in children during preschool age.
Fluoridated tooth paste is widely recommended, and has been documented to have caries preventive effect in children (11). In Norway, tooth brushing twice a day with tooth paste containing at least 0.1% fluoride from the time of eruption of the first primary tooth is recommended by the health authorities (12).
Recommendations regarding use of fluoride supplements in children vary. In most countries in Europe and in the USA, fluoride supplements are recommended to children considered to be at risk of developing caries (13, 14). Fluoride content of drinking water influences recommendations regarding fluoride supplementation. Water fluoridation is not common in Europe; only Spain, Ireland, UK, Poland and Serbia have fluoridated drinking water (15). Norway has not fluoridated water, and the fluoride content naturally occurring in water is limited. Use of fluoride lozenges was recommended for all children until 1996 when new guidelines recommending risk based use of fluoride supplements were introduced (12). Even if tooth brushing with fluoridated tooth paste and fluoride lozenges are widely recommended to prevent dental caries in children, knowledge of how these oral health behaviour change with age in preschool children is scarce.
Oral health behaviours are established early in life, and these behaviours are often maintained and associated with oral health conditions later in life (16). Oral health in childhood is a major predictor of adult oral health (17, 18). Early establishment of favourable oral health behaviour is considered a goal in the prevention of oral disease in children (12).
Children are dependent on their environment to establish and maintain oral health behaviour (16, 19). The parents' own oral health behaviour has been shown to influence children's oral health (20, 21). Parents have been shown to have greater impact on oral health behaviour in preschool children than in older children (22). Parental oral health behaviour may be influenced by social norms, cultural background and educational level (23, 24). In addition, some studies have shown that conditions in the family, such as family status or especially a change in it, and number of children in the family, are associated with the preschool child's oral health (21, 22, 25).
In the Norwegian Mother and Child Cohort Study, a prospective pregnancy cohort study, data regarding tooth brushing frequency, use of fluoridated tooth paste and fluoride lozenges in the children was collected several times during preschool age. These data provide opportunity to study the development of oral health behaviour during early childhood.
The aims of the present analyses were to study development, stability and changes in oral health behaviours, tooth brushing frequency, use of fluoridated tooth paste and fluoride lozenges in children from 1.5 to 5 years of age, and to study associations between oral health behaviour and family characteristics.
Materials and Methods
This study was based on data from the Norwegian Mother and Child Cohort Study conducted by the Norwegian Institute of Public Health (26, 27) and data from dental examination of 5-year-old children in the Public Dental Services.
The Mother and Child Cohort Study is a prospective pregnancy cohort study including 108 000 pregnancies recruited from 1999 to 2008. Participants were recruited by postal invitation in connection with routine ultrasound examination offered to all pregnant women in Norway at 17-18 weeks of gestation; 38.5% of all invited pregnant women agreed to participate. Data were collected by questionnaires completed by the mothers in pregnancy and early childhood. The current study was based on quality-assured data files (version 3) released for research in 2007, and was restricted to children born in 2002 in the county of Akershus. Altogether, 1607 children were included, 27% of the children born in Akershus in 2002. The study population was restricted to children with questionnaire data concerning oral health behaviour at 1.5, 3 and 5 years of age. In 836 children, the data were incomplete and these children were excluded. To evaluate loss to follow up the demographics in the initial material and the final study population were compared. The only significant difference was that more mothers with low education were found among the excluded children (p < 0.01). The final study population consisted of 771 children, 414 boys and 357 girls.
Parents were asked about the children's tooth brushing, use of fluoridated toothpaste and fluoride lozenges at 1.5, 3 and 5 years of age. Tooth brushing frequency was reported as brushing twice a day or more often, once a day or sometimes, and categorized in the analyses as brushing twice a day or less than twice a day. Use of fluoridated toothpaste and fluoride lozenges were reported as daily, sometimes or never, and in the analyses categorized as daily or less than daily. In Norway, all kinds of tooth pastes contain fluoride mainly two concentrations, tooth paste marketed for children contains 0.1% fluoride, and tooth paste marketed for adults 0.15% fluoride. Information about tooth brushing assistance given by the parents at 5 years of age was reported as twice a day, once a day or sometimes.
To study associations between family characteristics and oral health behaviour two variables were constructed: stable frequent brushing from 1.5 to 5 years of age and stable daily use of fluoride lozenges from 1.5 to 5 years of age. Data on tooth brushing frequencies at 1.5, 3 and 5 years of age were used and the children categorized as brushing twice a day at all three age points or brushing less than twice a day at at least one point in time. Data on the use of fluoride lozenges at 1.5, 3 and 5 years of age were used and the children categorized as using fluoride lozenges daily at all three ages or using fluoride lozenges less than daily at at least one point in time.
The family characteristics studied were parental national background, maternal education, stability of family status and number of children in the family. National background was recorded according to the country of birth of the mother and father. This information was combined to distinguish both parents being of western origin and one or both parents being of non-western origin. Non-western origin included parents born in Asia, Africa, South America, Central America and Eastern Europe. Maternal education was reported during pregnancy and included completed and ongoing education. High education was defined as more than 12 year at school and low education was defined as 12 year or less at school. The stability of family status was measured by registering whether mother and father lived together or not in pregnancy and when the child was aged 5 years, and dichotomized as having changed from two parents to one parent or not in the period. The number of siblings was reported in pregnancy as mother living in a household with children in addition to the studied child. In the analyses, the variable was trichotomized as none, one and two or more older siblings. The distribution of the family characteristics is given in Table 1.
Table 1.
Distribution of family characteristics (n = 771).
| % | (n*) | |
|---|---|---|
| Gender | ||
| Girl | 46 | (357) |
| Boy | 54 | (414) |
| Parental origin | ||
| One or both non-western | 3 | (25) |
| Both western | 97 | (746) |
| Maternal education | ||
| Short | 30 | (233) |
| Long | 70 | (536) |
| Older siblings | ||
| None | 45 | (349) |
| One | 38 | (290) |
| Two or more | 17 | (132) |
| Family status | ||
| Change | 8 | (60) |
| No change | 92 | (688) |
Reduced because of internal drop out
The statistical analyses were performed using IBM SPSS, version 20. Bivariate and multivariable logistic regression analyses were conducted with stable frequent brushing from 1.5 to 5 years of age, and stable daily use of fluoride lozenges from 1.5 to 5 years of age as dependent variables, and the family characteristics; parental national origin, maternal education, family status, older siblings and child gender as independent variables. Spearman's Rank correlation was used to explore collinearity between the independent variables before the multivariable analyses were conducted. Chi-square was used to test associations between the oral health behaviour variables. Results were reported using frequencies, odds ratios (OR), and 95% confidence intervals (CI).
Written, informed consent was obtained from all parents. The investigation was approved by the Regional Committee for Medical Research Ethics in South-Eastern Norway, The Norwegian Social Science Data Services and The Norwegian Data Inspectorate.
Results
The oral health behaviour of the children at 1.5, 3 and 5 years of age are shown in Table 2. The trend was that more children started brushing twice daily and used fluoride lozenges daily with increasing age. At child age 1.5 years, half of the children had their teeth brushed twice daily, increasing to 61% at 3 years of age and 76% at 5 years of age. At the age of 5 years, tooth brushing assistance was given by the parents twice daily to 35% of the children, daily to 59% and sometimes to 6% of the children. At 1.5 years of age, 37% of the children used fluoride lozenges daily and the proportion of children using fluoride lozenges daily increased to 74% at 3 years and remained at this level at 5 years of age. Fluoridated tooth paste was used by nearly all children at 1.5 years, 3 years and 5 years of age. Use of fluoridated tooth paste was not analysed further because of its nearly universal use in this population.
Table 2.
Description of oral health behaviour in the children at 1.5, 3 and 5 years of age (n = 771).
| % | (n*) | |
|---|---|---|
| Tooth brushing frequency | ||
| 1.5 years | ||
| Twice daily | 52 | (402) |
| Less than twice daily | 48 | (369) |
| 3 years | ||
| Twice daily | 61 | (468) |
| Less than twice daily | 39 | (303) |
| 5 years | ||
| Twice daily | 76 | (585) |
| Less than twice daily | 24 | (186) |
| Fluoride lozenges | ||
| 1.5 years | ||
| Daily | 37 | (288) |
| Less than daily | 63 | (483) |
| 3 years | ||
| Daily | 74 | (541) |
| Less than daily | 26 | (189) |
| 5 years | ||
| Daily | 75 | (574) |
| Less than daily | 25 | (195) |
| Fluoridated toothpaste | ||
| 1.5 years | ||
| Daily | 92 | (705) |
| Less than daily | 8 | (64) |
| 3 years | ||
| Daily | 95 | (731) |
| Less than daily | 5 | (37) |
| 5 years | ||
| Daily | 96 | (733) |
| Less than daily | 4 | (33) |
Reduced because of internal drop-out
The longitudinal changes in tooth brushing frequency at the individual level from 1.5 to 5 years of age are presented in Figure 1. The figure show that tooth brushing frequency established early was quite stable; of the children who had their teeth brushed twice daily at 1.5 years of age, the majority continued this behaviour at 3 years of age (88%) and at 5 years of age (85%). Children who had their teeth brushed twice daily at 1.5 years more often brushed twice daily at 3 years of age (p < 0.001), and at 5 years of age (p < 0.001) than other children. Of the children who brushed less than twice daily at 1.5 years of age, 39% still brushed less than twice daily at 5 years of age.
Figure 1.
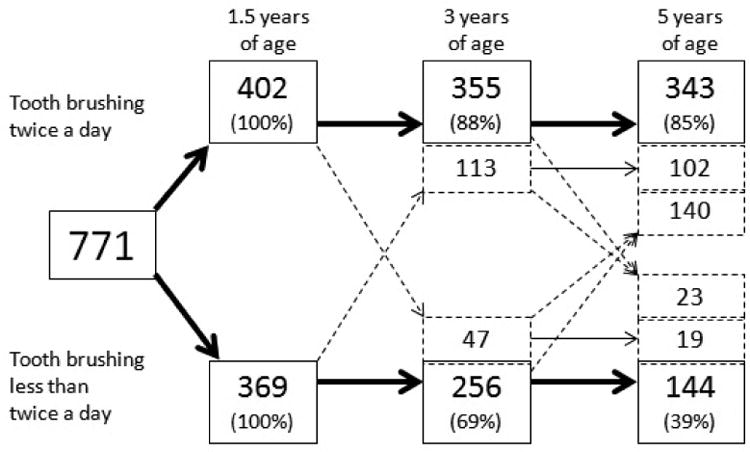
The longitudinal changes in tooth brushing frequency in children from 1.5 to 5 years of age (n = 771). Black arrows shows constant tooth brushing frequency and dotted arrows shows changes in tooth brushing frequency. The percentages give the proportion of children with stable behaviour.
The longitudinal changes in use of fluoride lozenges at the individual level from 1.5 to 5 years of age are presented in Figure 2. The figure show that daily use of fluoride lozenges established early was stable; the majority of the children using fluoride lozenges daily at 1.5 years of age continued to use fluoride lozenges daily at 3 years of age (90%) and at 5 years of age (83%). Children who used fluoride lozenges daily at 1.5 years more often used fluoride lozenges daily at 3 years of age (p < 0.001) and 5 years of age (p < 0.01) than other children.
Figure 2.
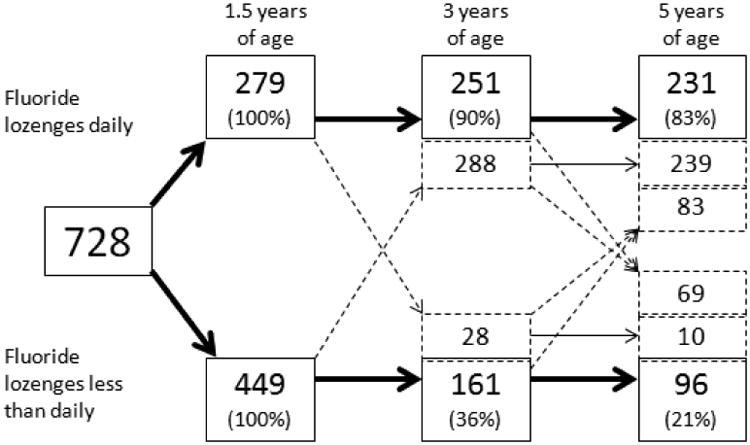
The longitudinal changes in use of fluoride lozenges in children from 1.5 to 5 years of age (n = 728). Black arrows shows constant use of fluoride lozenges and dotted arrows shows changes in use of fluoride lozenges. The percentages give the proportion of children with stable behaviour.
Table 3 shows the association between tooth brushing frequency and use of fluoride lozenges at the ages 1.5, 3 and 5 years respectively. At 1.5 years of age children who brushed twice daily more often used fluoride lozenges daily than children brushing less than twice daily (p = 0.03). At 3 and 5 years of age no statistically significantly associations between tooth brushing frequency and use of fluoride lozenges were found.
Table 3.
Association between tooth brushing frequency and daily use of fluoride lozenges at the ages 1.5, 3 and 5 years (n = 771).
| Age | Tooth brushing frequency | Use of fluoride lozenges | ||||
|---|---|---|---|---|---|---|
|
| ||||||
| Daily | Less than daily | p | ||||
| % | (n*) | % | (n*) | |||
| 1.5 years | Twice daily | 41 | (163) | 59 | (239) | |
| Less than twice daily | 34 | (125) | 66 | (244) | 0.03 | |
| 3 years | Twice daily | 76 | (333) | 24 | (104) | |
| Less than twice daily | 71 | (208) | 29 | (85) | ns | |
| 5 years | Twice daily | 76 | (440) | 24 | (143) | |
| Less than twice daily | 72 | (134) | 28 | (52) | ns | |
Reduced because of internal drop-out
Table 4 shows the results of the bivariate and multivariable analyses exploring the associations between stable frequent brushing from 1.5 to 5 years of age and family characteristics: parental national origin, maternal education, older siblings, family status and gender. The multivariable analysis showed that children whose parents were of western origin had an increased chance of brushing twice daily during preschool age compared with children one or both of whose parents were of non-western origin (OR 4, CI 1.3 – 11.9). Children with one older sibling had an increased chance of brushing twice daily during preschool age compared with children who had no older siblings (OR 1.4, CI 1.02 – 1.9).
Table 4.
Bivariate and multivariable logistic regression analysis of associations between stable frequent brushing from 1.5 to 5 years of age and parental national origin, maternal education, older siblings, family status and child gender.
| Stable frequent brushing | ||||
|---|---|---|---|---|
|
|
||||
| Bivariate (n = 771) | Multivariable (n = 746*) | |||
|
|
||||
| OR | 95% CI | OR | 95% CI | |
| Parental origin | ||||
| One or both non-western (ref) | ||||
| Both western | 3.3 | 1.2 – 8.9 | 4.0 | 1.3 – 11.9 |
| Maternal education | ||||
| Short (ref) | ||||
| Long | 1.2 | 0.9 - 1.6 | 1.1 | 0.8 – 1.6 |
| Older siblings | ||||
| None (ref) | ||||
| One | 1.4 | 1.0 - 1.9 | 1.4 | 1.02 – 1.9 |
| Two or more | 0.6 | 0.4 - 0.9 | 0.7 | 0.4 – 1.01 |
| Family status | ||||
| Change (ref) | ||||
| No change | 1.7 | 1.0 - 2.9 | 1.5 | 0.9 – 2.7 |
| Gender | ||||
| Girl (ref) | ||||
| Boy | 1.1 | 0.9 - 1.5 | 1.1 | 0.9 – 1.5 |
Reduced because of internal drop-out
Table 5 shows the results of the bivariate and multivariable analyses exploring the associations between stable daily use of fluoride lozenges from 1.5 to 5 years of age and the family characteristics: parental national origin, maternal education, older siblings and family status. Children with one older sibling had an increased chance of using fluoride lozenges daily during preschool age compared with children with no older siblings (OR 1.6, CI 1.1 – 2.2).
Table 5.
Bivariate and multivariable logistic regression analysis of associations between stable daily use of fluoride lozenges from 1.5 to 5 years of age and parental national origin, maternal education, older siblings, family status and child gender.
| Stable daily use of fluoride lozenges | ||||
|---|---|---|---|---|
|
| ||||
| Bivariate (n = 771) | Multivariable (n = 704*) | |||
|
| ||||
| OR | 95% CI | OR | 95% CI | |
| Parental origin | ||||
| One or both non-western (ref) | ||||
| Both western | 1.8 | 0.7 – 4.9 | 1.5 | 0.6 – 4.2 |
| Maternal education | ||||
| Short (ref) | ||||
| Long | 1.1 | 0.8 – 1.6 | 1.1 | 0.7 – 1.5 |
| Older siblings | ||||
| None (ref) | ||||
| One | 1.6 | 1.1 – 2.2 | 1.6 | 1.1 – 2.2 |
| Two or more | 1.1 | 0.7 – 1.8 | 1.1 | 0.7 – 1.8 |
| Family status | ||||
| Change (ref) | ||||
| No change | 2.1 | 1.1 – 4.1 | 2.0 | 0.99 – 3.9 |
| Gender | ||||
| Girl (ref) | ||||
| Boy | 0.9 | 0.7 – 1.3 | 0.9 | 0.7 – 1.3 |
Reduced because of internal drop-out
Discussion
The aim of this longitudinal study was to study the development, stability and changes of oral health behaviour in children from 1.5 to 5 years of age. The results showed that when the practices of tooth brushing twice daily and use of fluoride lozenges daily were established in early childhood, these behaviours were quite stable during preschool age. In addition, the study showed that some family characteristics were associated with tooth brushing frequency and use of fluoride lozenges.
This study was based on data from the Norwegian Mother and Child Cohort Study. The cohort study design, with data collection several times during early childhood, has the advantage of reducing the risk of bias resulting from parents' ability to recall the oral health behaviour. In this study, the proportion of parents of non-western origin and the proportion of mothers with low education were lower than in the Norwegian population (28, 29), probably due to self selection and loss to follow-up, known findings in studies with longitudinal designs (30). The under representation of non-western parents and mothers with low education probably resulted in a lower proportion of risk children in the study population than in the Norwegian population. If more risk children had been included probably a higher proportion of children would be brushing less than twice daily and using fluoride lozenges less than daily. Even if the reported proportion of children with favourable oral health behaviour probably was overestimated in the study population, the reported tooth brushing frequencies were in line with results from Sweden (5). Selection bias influence on the level of the variables but to a less extent the associations between the variables, and previous analyses of other variables in the Mother and Child Cohort Study have shown no statistically significant differences in association measures between participants and the total population regarding exposure-outcome associations (31). In the multivariate analyses in this study maternal education did not influence the stability of the oral health behaviours and national origin influenced only the stability of tooth brushing frequency. This indicates that the loss to follow up had limited consequences on the results of the study.
Tooth brushing twice daily at age 1.5 year was reported by more than half (52%) of the parents. This behaviour is recommended for all children from eruption of the first tooth in Norway (12), and the result indicates that preventive advice to parents is still needed. As expected, the proportion of children who brushed twice daily was shown to increase with increasing child age. The tooth brushing frequencies reported at 5 years of age (76% brushed twice daily) were in line with reported tooth brushing frequency in children at the same age in Sweden (73%) (5). Less frequent brushing has been reported in studies from Finland (18%), Australia (61%) and Belgium (23%), countries that also report higher caries prevalence in 5-year-olds than in Norway (3, 4, 8, 32).
Daily use of fluoridated tooth paste is documented to prevent caries development in preschool children, and is recommended worldwide (11-13). The results from this study showed that almost all parents reported daily use of fluoridated tooth paste from 1.5 to 5 years of age, indicating that information on the caries preventive effect of fluoride has influenced the behaviour of Norwegian parents. The limited availability of tooth paste without fluoride may have facilitated the implementation of fluoridated tooth paste.
Most children (75%) were reported to use of fluoride lozenges daily at 3 and 5 years of age, and one third of the children was reported to use fluoride lozenges daily at 1.5 year of age. The scientific evidence in support of fluoride supplements for caries prevention in preschool children is poor, and it has not been documented that fluoride supplements give additional caries prevention in children who already use fluoridated tooth paste (33, 34). Nearly twenty years after the change in Norwegian recommendations from universal to risk based use of fluoride lozenges, the majority of the preschool children still use lozenges daily. Fewer than 20% of 5-year-olds in Norway have caries experience (20, 32), indicating that children at low risk of caries also use fluoride lozenges. Combining use of fluoride lozenges and fluoride tooth paste may entail risk of dental fluorosis, especially among young preschool children. A substantial increase in the proportion of children using fluoride lozenges daily was found between 1.5 and 3 years of age. In this period, the children have their first routine examination in the Public Dental Services which may indicate that dental health personnel still recommend fluoride lozenges to the majority of preschool children.
It is documented that risk behaviours tend to cluster (35). An association between daily use of fluoride lozenges and frequent tooth brushing was found at 1.5 year of age, showing that parents who introduce caries preventive practices in their children early often introduces more than one behaviour.
Frequent tooth brushing and daily use of fluoride lozenges established early were quite stable throughout the preschool period in this study. Previous studies on development of oral health behaviour in this age are sparse, but the present results are in line with one previous study that showed that oral health behaviour established before 3 years of age remained fairly stable over a two year period (8). Behaviours performed daily, such as tooth brushing, will often become routine and previous behaviours have been shown to predict future behaviours (36). Early establishment of daily routines, such as tooth brushing and use of fluoride, may facilitate maintenance of good oral health during childhood and into adult life.
The results showed associations between stable frequent brushing from 1.5 to 5 years of age and parental origin. The teeth of preschool children with parents of non-western origin were brushed less often than those of children with parents of western origin. This finding could be due to differences in culture or social norms (23). Parents of non-western origin have been shown to introduce tooth brushing later than parents of western origin (23, 37, 38) and have been shown to be more negligent regarding oral health behaviour than parents of western origin (20, 23, 39).
In this study, the teeth of children with one older sibling were more frequently brushed and these children more often used fluoride lozenges during preschool age than children living in families without older children. In these families, oral health behaviour may already have been established and transferred to the younger child at an early age. This finding may indicate that giving oral health preventive advice to parents of a first child will benefit younger siblings. Focusing on preventive dental care when parents have their first child may reduce the resources needed for repeated advice. However, repeated advice may benefit some children.
In conclusion, oral health behaviour established in early life was stable during preschool age. The results indicate that tooth brushing frequency and daily use of fluoride lozenges were not in accordance with the present recommendations, based on the scientific literature, and the preventive practices recommended by the health authorities. The teeth of Norwegian preschool children were brushed less frequently than recommended, and daily fluoride lozenges were used by more children than recommended.
Acknowledgments
We would like to thank the participants in the study, and the Public Dental Services in Akershus for their cooperation. The Norwegian Mother and Child Cohort Study is supported by the Norwegian Ministry of Health and the Ministry of Education and Research, NIH/NIEHS (contract no N01-ES-75558), NIH/NINDS (grant no.1 UO1 NS 047537-01 and grant no.2 UO1 NS 047537-06A1), and the Norwegian Research Council/FUGE (grant no. 151918/S10).
References
- 1.Gibson S, Williams S. Dental caries in pre-school children: associations with social class, toothbrushing habit and consumption of sugars and sugar-containing foods. Further analysis of data from the National Diet and Nutrition Survey of children aged 1.5-4.5 years. Caries Res. 1999;33:101–13. doi: 10.1159/000016503. [DOI] [PubMed] [Google Scholar]
- 2.Dos Santos AP, Nadanovsky P, de Oliveira BH. A systematic review and meta-analysis of the effects of fluoride toothpastes on the prevention of dental caries in the primary dentition of preschool children. Community Dent Oral Epidemiol. 2013;41:1–12. doi: 10.1111/j.1600-0528.2012.00708.x. [DOI] [PubMed] [Google Scholar]
- 3.Kilpatrick NM, Neumann A, Lucas N, Chapman J, Nicholson JM. Oral health inequalities in a national sample of Australian children aged 2-3 and 6-7 years. Aust Dent J. 2012;57:38–44. doi: 10.1111/j.1834-7819.2011.01644.x. [DOI] [PubMed] [Google Scholar]
- 4.Leroy R, Jara A, Martens L, Declerck D. Oral hygiene and gingival health in Flemish pre-school children. Community Dent Health. 2011;28:75–81. [PubMed] [Google Scholar]
- 5.Hugoson A, Koch G, Gothberg C, Helkimo AN, Lundin SA, Norderyd O, et al. Oral health of individuals aged 3-80 years in Jonkoping, Sweden during 30 years (1973-2003). I. Review of findings on dental care habits and knowledge of oral health. Swed Dent J. 2005;29:125–38. [PubMed] [Google Scholar]
- 6.Paunio P, Rautava P, Sillanpää M, Kaleva O. Dental health habits of 3-year-old Finnish children. Community Dent Oral Epidemiol. 1993;21:4–7. doi: 10.1111/j.1600-0528.1993.tb00708.x. [DOI] [PubMed] [Google Scholar]
- 7.Grytten J, Rossow I, Holst D, Steele L. Longitudinal study of dental health behaviors and other caries predictors in early childhood. Community Dent Oral Epidemiol. 1988;16:356–9. doi: 10.1111/j.1600-0528.1988.tb00581.x. [DOI] [PubMed] [Google Scholar]
- 8.Mattila ML, Paunio P, Rautava P, Ojanlatva A, Sillanpää M. Changes in dental health and dental health habits from 3 to 5 years of age. J Public Health Dent. 1998;58:270–4. doi: 10.1111/j.1752-7325.1998.tb03008.x. [DOI] [PubMed] [Google Scholar]
- 9.Stecksen-Blicks C, Borssen E. Dental caries, sugar-eating habits and toothbrushing in groups of 4-year-old children 1967-1997 in the city of Umea, Sweden. Caries Res. 1999;33:409–14. doi: 10.1159/000016544. [DOI] [PubMed] [Google Scholar]
- 10.Petersen PE. Oral health behavior of 6-year-old Danish children. Acta Odontol Scand. 1992;50:57–64. doi: 10.3109/00016359209012747. [DOI] [PubMed] [Google Scholar]
- 11.Marinho VC, Higgins JP, Sheiham A, Logan S. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003:CD002278. doi: 10.1002/14651858.CD002278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Norwegian Directorate of Health. Tenner for livet Helsefremmende og forebyggende arbeid [Teeth for life Health promotion and health prevention] Oslo: 1999. Report No.: IS-2659. [Google Scholar]
- 13.European Academy of Paediatric Dentistry. Guidelines on the use of fluoride in children: an EAPD policy document. Eur Arch Paediatr Dent. 2009;10:129–35. doi: 10.1007/BF03262673. [DOI] [PubMed] [Google Scholar]
- 14.Rozier RG, Adair S, Graham F, Iafolla T, Kingman A, Kohn W, et al. Evidence-based clinical recommendations on the prescription of dietary fluoride supplements for caries prevention: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2010;141:1480–9. doi: 10.14219/jada.archive.2010.0111. [DOI] [PubMed] [Google Scholar]
- 15.The British Fluoridation Society. The extent of fluoridation worldwide. British Fluoridation Society; Available from: URL: http://www.bfsweb.org/onemillion/onemillion2012.html [cited 2013 Jul 31] [Google Scholar]
- 16.Christensen P. The health-promoting family: a conceptual framework for future research. Soc Sci Med. 2004;59:377–87. doi: 10.1016/j.socscimed.2003.10.021. [DOI] [PubMed] [Google Scholar]
- 17.Leroy R, Bogaerts K, Lesaffre E, Declerck D. Effect of caries experience in primary molars on cavity formation in the adjacent permanent first molar. Caries Res. 2005;39:342–9. doi: 10.1159/000086839. [DOI] [PubMed] [Google Scholar]
- 18.Li Y, Wang W. Predicting caries in permanent teeth from caries in primary teeth: an eight-year cohort study. J Dent Res. 2002;81:561–6. doi: 10.1177/154405910208100812. [DOI] [PubMed] [Google Scholar]
- 19.Poutanen R, Lahti S, Tolvanen M, Hausen H. Parental influence on children's oral health-related behavior. Acta Odontol Scand. 2006;64:286–92. doi: 10.1080/00016350600714498. [DOI] [PubMed] [Google Scholar]
- 20.Wigen TI, Wang NJ. Caries and background factors in Norwegian and immigrant 5-year-old children. Community Dent Oral Epidemiol. 2010;38:19–28. doi: 10.1111/j.1600-0528.2009.00502.x. [DOI] [PubMed] [Google Scholar]
- 21.Mattila ML, Rautava P, Sillanpää M, Paunio P. Caries in five-year-old children and associations with family-related factors. J Dent Res. 2000;79:875–81. doi: 10.1177/00220345000790031501. [DOI] [PubMed] [Google Scholar]
- 22.Christensen LB, Twetman S, Sundby A. Oral health in children and adolescents with different socio-cultural and socio-economic backgrounds. Acta Odontol Scand. 2010;68:34–42. doi: 10.3109/00016350903301712. [DOI] [PubMed] [Google Scholar]
- 23.Skeie MS, Riordan PJ, Klock KS, Espelid I. Parental risk attitudes and caries-related behaviours among immigrant and western native children in Oslo. Community Dent Oral Epidemiol. 2006;34:103–13. doi: 10.1111/j.1600-0528.2006.00256.x. [DOI] [PubMed] [Google Scholar]
- 24.Van den Branden S, Van den Broucke S, Leroy R, Declerck D, Hoppenbrouwers K. Effects of time and socio-economic status on the determinants of oral health-related behaviours of parents of preschool children. Eur J Oral Sci. 2012;120:153–60. doi: 10.1111/j.1600-0722.2012.00951.x. [DOI] [PubMed] [Google Scholar]
- 25.Wigen TI, Espelid I, Skaare AB, Wang NJ. Family characteristics and caries experience in preschool children. A longitudinal study from pregnancy to 5 years of age. Community Dent Oral Epidemiol. 2011;39:311–7. doi: 10.1111/j.1600-0528.2010.00596.x. [DOI] [PubMed] [Google Scholar]
- 26.Magnus P, Irgens LM, Haug K, Nystad W, Skjaerven R, Stoltenberg C. Cohort profile: the Norwegian Mother and Child Cohort Study (MoBa) Int J Epidemiol. 2006;35:1146–50. doi: 10.1093/ije/dyl170. [DOI] [PubMed] [Google Scholar]
- 27.Irgens LM. The Medical Birth Registry of Norway. Epidemiological research and surveillance throughout 30 years. Acta Obstet Gynecol Scand. 2000;79:435–9. [PubMed] [Google Scholar]
- 28.Statistics Norway. Immigrants and Norwegian-born to immigrant parents. Statistisk sentralbyrå; Available from: URL: http://www.ssb.no/en/innvbef [cited 2013 Jul 31] [Google Scholar]
- 29.Statistics Norway. Education. Statistisk sentralbyrå; Available from: URL: http://www.ssb.no/en/utdanning [cited 2013 Jul 31] [Google Scholar]
- 30.Rothman KJ, Greenland S, Lash TL. Modern epidemiology. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins; 2008. [Google Scholar]
- 31.Nilsen RM, Vollset SE, Gjessing HK, Skjaerven R, Melve KK, Schreuder P, et al. Self-selection and bias in a large prospective pregnancy cohort in Norway. Paediatr Perinat Epidemiol. 2009;23:597–608. doi: 10.1111/j.1365-3016.2009.01062.x. [DOI] [PubMed] [Google Scholar]
- 32.Statistics Norway. Dental status by age. Statistisk sentralbyrå; Available from: URL: http://www.ssb.no/en/sok?sok=dental+status+by+age [cited 2013 Feb 6] [Google Scholar]
- 33.Riordan PJ. Fluoride supplements for young children: an analysis of the literature focusing on benefits and risks. Community Dent Oral Epidemiol. 1999;27:72–83. doi: 10.1111/j.1600-0528.1999.tb01994.x. [DOI] [PubMed] [Google Scholar]
- 34.Tubert-Jeannin S, Auclair C, Amsallem E, Tramini P, Gerbaud L, Ruffieux C, et al. Fluoride supplements (tablets, drops, lozenges or chewing gums) for preventing dental caries in children. Cochrane Database Syst Rev. 2011:CD007592. doi: 10.1002/14651858.CD007592.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Sanders AE, Spencer AJ, Stewart JF. Clustering of risk behaviours for oral and general health. Community Dent Health. 2005;22:133–40. [PubMed] [Google Scholar]
- 36.Ouellette JA, Wood W. Habit and intention in everyday life:The multiple process by which past behavior predicts future behavior. Psychol Bull. 1998;124:54–74. [Google Scholar]
- 37.Vanobbergen J, Martens L, Lesaffre E, Bogaerts K, Declerck D. Assessing risk indicators for dental caries in the primary dentition. Community Dent Oral Epidemiol. 2001;29:424–34. doi: 10.1034/j.1600-0528.2001.290603.x. [DOI] [PubMed] [Google Scholar]
- 38.Verrips GH, Frencken JE, Kalsbeek H, ter HG, Filedt Kok-Weimar TL. Risk indicators and potential risk factors for caries in 5-year-olds of different ethnic groups in Amsterdam. Community Dent Oral Epidemiol. 1992;20:256–60. doi: 10.1111/j.1600-0528.1992.tb01694.x. [DOI] [PubMed] [Google Scholar]
- 39.Adair PM, Pine CM, Burnside G, Nicoll AD, Gillett A, Anwar S, et al. Familial and cultural perceptions and beliefs of oral hygiene and dietary practices among ethnically and socio-economicall diverse groups. Community Dent Health. 2004;21:102–11. [PubMed] [Google Scholar]