

A 52-year-old male was referred for treatment of a 4-month history of right palmar numbness and tingling that was unresponsive to analgesics. Electrophysiological studies confirmed the diagnosis of carpal tunnel syndrome. He reported drinking more than 100 g of alcohol per day and had a > 15-year history of hypertensive nephropathy and chronic tophaceous gout. To date, he had intermittently taken colchicine and low doses of steroids and allopurinol. On physical examination, swelling was present over the right volar aspect of the carpal region, and he was unable to flex because of subcutaneous rigidity. Positive Tinel's sign and Phalen's maneuver were present.
All routine laboratory test results were within the reference ranges, with the exception of the uric acid level (9.8 mg/dL) and erythrocyte sedimentation rate (48.0 mm/hr), both of which exceeded the high end of the reference ranges. Computed tomography of the right wrist showed extensive amorphous, cloud-like calcifications (Fig. 1A, arrow) and multiple punched-out bony erosions in the carpal bones (Fig. 1A, arrowheads). On the three-dimensional reconstruction, extensive tophi were easily seen in the intercarpal and radiocarpal joints with compression overlying the flexor tendons (Fig. 1B and 1C).
Figure 1.
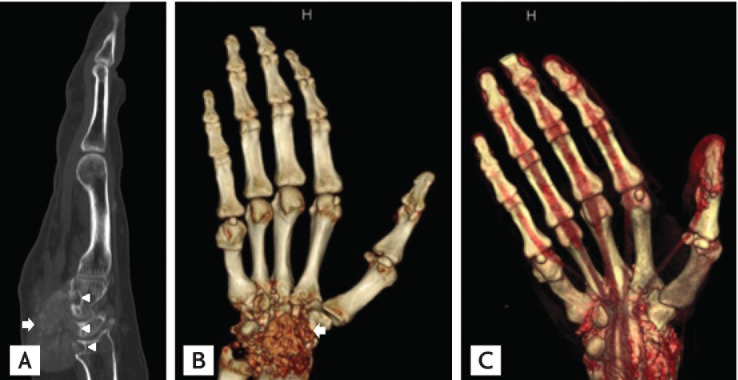
Computed tomography of the right hand. (A) It shows extensive compressive amorphous mass (arrow) with multiple carpal bone erosion (arrowheads). (B, C) On the three-dimensional reconstruction, amplectant tophi are located in the wrist joint (arow) with compression overlying the flexor tendon.
The carpal tunnel is a rigid cannular path formed by bony walls on three sides and roofed by a tough transverse carpal ligament. The median nerve may be directly damaged or secondarily compressed. Secondary compression can be further divided into traumatic and nontraumatic conditions. Gout, a result of an increased volume of contents within the rigid tunnel, may be one cause of nontraumatic compression of the median nerve. Despite the space-occupying nature of gouty tophi, carpal tunnel syndrome secondary to gout is uncommon. Tophaceous gout may involve not only the median nerve but also the flexor tendons inside the carpal tunnel.
In a patient with established gout, tophi should be considered to be a potential cause of mechanical or neurological symptoms originating from the carpal tunnel. Surgery is recommended to decompress the median nerve, confirm the diagnosis, and immediately improve the relief of the flexor tendon's rigidity. Uricase can be recommended as medical treatment. Early diagnosis and control of gout are necessary to avoid irreversible complications.
Acknowledgments
This study is supported by the Soonchunhyang University.
Footnotes
No potential conflict of interest relevant to this article was reported.