

Abstract
With the rapid aging of the population in Korea, the number of older people with dementia is projected to increase, forecasting an epidemic of dementia. Recent trends in dementia in several western countries, however, depict a gradual decline in prevalence and incidence. This decrease has been attributed to an improvement in education and living environments, engagement in healthy behaviors, and reduction in the prevalence of vascular risk factors. In Korea, however, trends in modifiable risk factors do not favor an optimistic outlook due to the continuous increase in the prevalence of hypertension, diabetes mellitus, and obesity. Given these observations, there is much to be gained through the promotion of healthy lifestyles. Moreover, public health resources need to be directed toward the provision of health promotion and preventive services, control and management of vascular risk factors, and improvement in the standard of living. Nationwide initiatives to develop and implement policies and strategies to protect cognitive health throughout the lifespan should be considered a public health priority.
Keywords: Dementia, Prevalence, Incidence, Risk Factors, Prevention and Control, Health Promotion, Health Behavior
INTRODUCTION
With the aging of the population, dementia is widely recognized as a serious threat to health in later life. It was estimated in 2010 that 35.6 million people aged 60 yr and older worldwide have dementia, with a prevalence of 4.7% (1). This means that there are 7 million incident dementia patients every year or one new case every 4 seconds. The number with dementia is projected to double every 20 yr to 65.7 million in 2030 and 115.4 million in 2050.
In the Republic of Korea, the number of older people with dementia was estimated to be 540,000 in 2012, with a prevalence of 9.2%, and projected to double every 20 yr, increasing to 1.27 million (10.0%) in 2030 and 2.71 million (15.1%) by 2050 (2). Older adults aged 65 yr and above were estimated to number 6 million in 2013, comprising 12.2% of the total population (3). Korea has one of the fastest aging population of any country in the world, with the proportion of older people expected to increase to 24.4% (11.7 million) by 2030, and approaching 38.8% (15.6 million) in 2050. The rapid aging of the population in Korea is expected to have a major impact on future dementia prevalence, given that age is a major risk factor for dementia. The trend in the increase in dementia cases is expected to outpace the increase in numbers of the older population, foreshadowing an epidemic of dementia.
Dementia imposes a huge economic burden on society, with an estimated cost of USD 604 billion in 2010 worldwide (4). This amounts to a cost of USD 16,986 per person with dementia. Among the total costs, medical care accounts for 16%, while social care in community and residential care settings comprise 42.3% and informal care, 41.7%. Just factoring in the projected increase in the number of people with dementia, the societal cost is expected to increase by 85% in 2030. The socioeconomic cost of dementia in Korea was estimated to be KRW 8.7 trillion (USD 8 billion) in 2010 and projected to double every 10 yr to KRW 38.9 trillion (USD 35.9 billion) (5). The estimated annual total cost per person with dementia was KRW 18.5 million (USD 17,113), with 53.4% for direct medical care, 32.7% for indirect medical care (19.3% on informal care), and 13% for long-term care (5).
The burden of caring for dementia is high due to limitations in activities of daily living and dependency caused by the disease. The average years lived with disability (YLD) for dementia is 7.4 yr, ranked second among chronic conditions by YLD (6). The caregiver spends on average 3.6 hr per day providing help with daily activities and 2.6 hr per day supervising the individual patient (4). The time spent on caregiving negatively affects the work, family, and leisure life of the family caregiver, putting economic pressure and a psychological burden on the family. Chronic stress due to caregiving itself takes a heavy toll on the caregiver, with 40%-75% suffering from serious mental illness and 15%-32% having major depression.
RECENT TRENDS IN DEMENTIA WORLDWIDE
Dementia prevalence
Although the prevalence of dementia worldwide has been projected to increase due to population aging, a growing number of studies in recent years are reporting a decreasing trend in the dementia prevalence (Table 1). In 2005, Manton et al. (7), analyzing data from the National Long-Term Care Survey (NLTCS), reported a decline in the prevalence of dementia in the US elderly aged 65 yr and older. The prevalence of severe cognitive impairment (SCI), defined using a cognitive screening test, decreased from 5.7% in 1982 to 2.9% in 1999, amounting to 310,000 fewer cases. The decline in prevalence was more pronounced in men than women. Using diagnosis data from the medical records, a significant decline in mixed dementias but not in Alzheimer's dementia was also observed.
Table 1.
Studies reporting declining prevalence or incidence of dementia and cognitive impairment
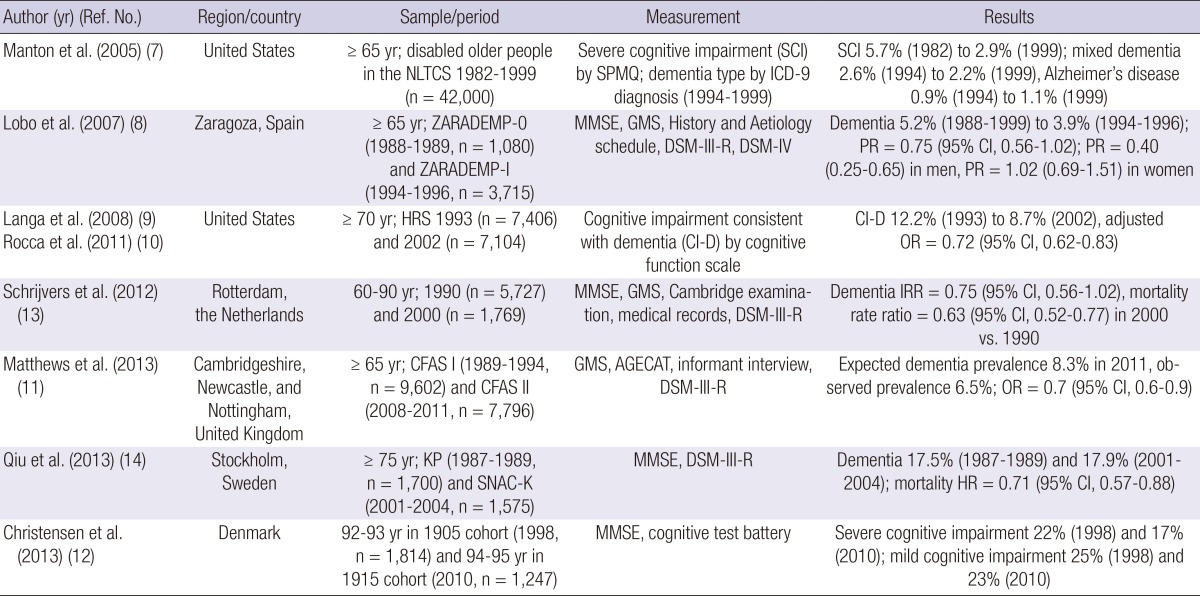
AGECAT, Automated Geriatric Examination for Computer Assisted Taxonomy; CFAS, Cognitive Functional and Ageing Study; CI, confidence interval; DSM, Diagnostic and Statistical Manual of Mental Disorders (III-R: 3rd version, IV: 4th version); GMS, Geriatric Mental State schedule; HR, hazard ratio; HRS, Health and Retirement Survey; ICD-9, International Classification of Diseases, 9th Revision; IRR, incidence rate ratio; KP, Kungsholmen Project; MMSE, Mini-Mental State Examination; NLTCS, National Long-Term Care Survey; OR, odds ratio; PR, prevalence ratio; SNAC-K, Swedish National study on Aging and Care in Kungsholmen; SPMQ, Short Portable Mental State Questionnaire; ZARADEMP, ZARAgoza DEMentia DEPression Project.
The Zaragoza Study (8) examined the prevalence of dementia in a representative sample of both institutionalized and non-institutionalized older people in Spain. Dementia cases were identified using a standardized clinical interview schedule according to Diagnostic and Statistical Manual of Mental Disorders (DSM) IV criteria. Among urban residents aged 65 yr and older, the dementia prevalence was found to be quite stable between two periods, 1988-1989 (5.2%; 95% confidence interval [CI], 3.9-6.6) and 1994-1996 (3.9%; 95% CI, 3.3-4.5), with a prevalence ratio (PR) of 0.75 (95% CI, 0.56-1.02). The prevalence, however, significantly decreased among men (PR, 0.40; 95% CI, 0.25-0.65), particularly those in the 70 to 84 yr age group, but not in women (PR, 1.02; 95% CI, 0.69-1.51).
Langa et al. (9) and Rocca et al. (10) used the Health and Retirement Survey (HRS), a national survey in the US, to examine temporal trends in the prevalence of cognitive impairment between 1993 and 2002. A 35-point cognitive function scale was used to define cognitive impairment consistent with dementia (CI-D). CI-D showed a significant decrease from 12.2% to 8.7% over the decade. The unadjusted odds ratio (OR) in the prevalence between 2002 and 1993 was 0.68 (95% CI, 0.60-0.77). Even adjusting for demographic and lifestyle factors and chronic conditions, the trend toward decreasing prevalence remained significant (OR, 0.72; 95% CI, 0.62-0.83). A significant decline in mortality from cognitive impairment during the same decade suggested compression of cognitive morbidity. In contrast, analysis using population-based data from the US states of Minnesota (1975-1994), Illinois (1997-2008), and Indiana (1992 vs. 2001) did not support a decrease in the prevalence of dementia (10).
The Medical Research Council Cognitive Function and Ageing Study (MRC CFAS) reported a decreased prevalence of dementia during a 20-yr period among residents of Cambridgeshire, Newcastle, and Nottingham in the UK (11). CFAS I (1989-1994) and CFAS II (2008-2011) employed an identical sampling design and methods. Based on the estimated 664,000 with dementia in 1991, 884,000 were expected to have dementia in 2011 due to population aging. However, the actual observed number in 2011 was 670,000, demonstrating a decrease of 24%. This translated to a decrease of 1.8 percentage points, from 8.3% to 6.5%, in the predicted prevalence (OR, 0.7; 95% CI, 0.6-0.9). The prevalence of dementia in residential and nursing homes increased from 56.4% to 69.6% during the same period, but with a coinciding reduction in the proportion of older people in care settings from 5% to 3%.
In two Danish cohorts of nonagenarians, cognitive functioning was found to be significantly better in the 1915 birth cohort in 1998 than in the 1905 birth cohort in 2010 (12). The proportion with cognitive impairment, measured on the Mini-Mental State Examination (MMSE) scale, was estimated to be 47% among the 1905 birth cohort and 40% in the 1915 birth cohort. The proportion of respondents exhibiting a maximum score range of 28-30, the highest level of cognitive functioning, on the MMSE was higher in the 1915 birth cohort (23%) than in the 1905 birth cohort (13%). Moreover, cognitive performance, assessed by a battery of tests involving fluency tasks, forward and backward digit spans, and immediate and delayed recall, was significantly better in the later cohort (P<0.001).
Dementia incidence
Two additional studies have reported a decrease in the incidence of dementia. In the Rotterdam Study (13), a decline in dementia incidence was observed during a 20-yr period. Among the 1990 cohort of 25,696 person-years of follow-up, 286 people developed dementia, whereas in the 2000 cohort of 8,384 person-years of follow-up, 49 developed dementia, with an incidence rate ratio (IRR) of 0.75 (95% CI, 0.56-1.02). Although the IRR was not statistically significant, the reduction in risk was consistent across age- and gender-specific strata. In addition, a significant decline in mortality rates (rate ratio, 0.63; 95% CI, 0.52-0.77) indicated a decrease in dementia incidence, considering the competing risk of vascular risk factors for both dementia and mortality. The diagnostic criteria used in the two cohorts were the same. The authors further suggested that an increased awareness of dementia by physicians, with an increased case identification over the years, would have resulted in an underestimation of the difference in the incidence rates between the two cohorts. Moreover, brain imaging showed a higher total brain volume and fewer white matter lesions over time, indicating less brain atrophy and cerebral small vessel disease.
In Sweden, trends in the prevalence of dementia were assessed over 20 yr in two population-based surveys in the Kungsholmen area of central Stockholm (14). The DSM-III-R was used to diagnose dementia in both surveys. Among the study participants 75 yr and older, the dementia prevalence was stable at 17.5% during 1987-1989 and 17.9% in 2001-2004, controlling for age, sex, and education (OR, 1.17; 95% CI, 0.95-1.46). Mortality, however, decreased during this period (hazard ratio, 0.71; 95% CI, 0.57-0.88). Although the prevalence of dementia was stable between the late 1980s and the early 2000s, the increased survival during the interval suggested a decrease in the incidence of dementia.
What is causing the decline?
Notwithstanding potential sources of bias in these studies, such as sample selection, attrition, and methods of case identification and diagnosis, and the need for further verification of the findings, there appears to be accumulating evidence of a declining prevalence or incidence of dementia in the US and several European countries. The cause for the decline in dementia prevalence has been attributed to the reduction and control of risk factors. Examples include an increased level of education in older people and intellectual stimulation (7, 9, 10, 11, 12, 13), improved general living, work environment, and social welfare (12, 14), enhanced healthy behaviors such as avoidance of smoking, increased participation in physical and social activities, and nutrition (8, 10, 14), a low burden of infectious diseases (12), control of vascular risk factors such as diabetes mellitus and cardiovascular diseases (8, 10, 11, 13, 14), a decline in stroke rates and consequent decline in post-stroke dementias (7, 13), and an increased use of prophylactic medications such as statins, nootropics, estrogen, and anti-inflammatory and anti-oxidative agents (7, 9, 13).
PROSPECTS FOR DEMENTIA PREVENTION
The impact of dementia prevention
Because no effective treatment for dementia is currently available, prevention is key to control its projected rise in prevalence worldwide. Preventive measures that delay the onset of dementia would be effective in reducing the number of future dementia cases. Alternatively, therapeutic interventions delaying the progression of the disease would reduce the proportion of late-stage or severe dementia.
In the US, the number with Alzheimer's disease was estimated to be 2.32 million in 1997, and estimated to increase to 8.64 million in the next 50 yr (15). Delaying the onset of dementia by 5 yr is expected to reduce the number of new cases by 4 million. A two-year delay would reduce the number by 1.94 million, and delaying the onset even by one year would reduce it by 770,000 incident cases.
The potential impact of dementia prevention is even greater on a global scale. In 2006, the prevalence of Alzheimer's disease was estimated to be 26.6 million worldwide and predicted to grow to 106.8 million by 2050 (16). If the onset of dementia could be delayed by 2 yr, there would be 22.8 million fewer cases. Even a year's delay would decrease the prevalence by 11.8 million. In contrast, delaying the progression of dementia by one year would actually increase the prevalence by 2.8 million. However, a combination of a year's delay in both the onset and progression would result in a decrease of 9.2 million cases, with 8.7 million fewer late-stage dementia cases.
Dementia epidemic in Korea: imminent or avoidable?
Because cognitive decline and dementia are attributed to many modifiable lifestyle and health-related factors, the changing trend in the major risk factors of dementia may foretell the future prevalence of dementia. In Korea, however, the reported trends in the risk factors do not support an optimistic forecast. According to the Korea National Health and Nutrition Examination Survey, in adults aged 65 yr and older, the prevalence of hypertension in 2005 was 52.4% in men and 59.0% in women, an increase from 47.0% for men and 57.0% for women in 1998 (17). Type 2 diabetes also demonstrated an increased prevalence in both men (13.2% to 16.2%) and women (11.4% to 16.0%) during this period. Those overweight or obese showed an increase from 11.2% to 28.1% in men and 33.3% to 36.6% in women. The percentage of current smokers decreased from 51.8% to 36.0% in men, but increased from 14.9% to 18.1% in women. The education level among older people has improved over the years, with the proportion having received no formal education decreasing from 52.9% in 1998 to 31.6% in 2011 (18, 19). However, many older people still suffer from low income and poor living conditions, with 45.1% living in poverty, defined as the proportion of the elderly living in households below 50% of median disposable income (20).
Among adults aged 19 yr and older, the smoking prevalence in men steadily decreased from 67% in 1998 to 45.1% in 2007, but has not changed much since, and was estimated to be 46% in 2011 (21). In women, smoking rates were stable at 6.6% in 1998 and 6.5% in 2011. The prevalence of overweight or obesity between 1998 and 2011 has increased from 29% to 34% among those aged 30 yr or older. Participation in moderate intensity physical activity has declined during 2005-2011, from 71.1% to 50.6% in men and from 65.7% to 42.6% in women. Among the vascular risk factors, the prevalence of hypertension has not changed much in men (31.1% in 1998 to 33.9% in 2011) and women (27.0% in 1998 to 27.8% in 2011). However, the age-adjusted prevalence has shown a 0.2%-0.3% annual decrease. There was also an increase in treatment rates from 16% in 1990 to 61% in 2011, and in control rates from 1% in 1990 to 43% in 2011. The prevalence of hypercholesterolemia, in comparison, has increased from 9.9% in 1998 to 14.5% in 2011. The treatment and control rates for hypercholesterolemia were low at 33% and 26%, respectively, in the two periods.
In light of this trend in the risk factors for dementia, it is unlikely that a decline in the prevalence of dementia in Korea will be evident in the near future. In Japan, several regional studies between 1992 and 2008 have shown an increase in dementia prevalence (22). This has been attributed to an increase in the prevalence of type 2 diabetes and the metabolic syndrome, and a plateau since the late 1990s in the previously declining stroke incidence.
Averting the dementia epidemic: future directions
Despite the dire outlook for an emerging epidemic of dementia, prevention efforts may help to mitigate the projected trend in dementia prevalence. It has been estimated that about half of Alzheimer's disease cases worldwide (17.2 million) are attributable to potentially modifiable risk factors, such as diabetes mellitus, midlife hypertension, midlife obesity, depression, physical inactivity, smoking, and low education (population attributable risk, 50.7%) (23). Reduction in the prevalence of these seven risk factors by 10%-25% would result in 1.1 to 3 million fewer cases worldwide. By applying effective preventive interventions to reduce the risk of dementia, it may be possible to stem the rising tide of the dementia outbreak.
Primary prevention needs to be at the core of the strategy to control dementia. Increasing the level of awareness about dementia and recognizing the importance of prevention by both the public and professionals would be a first step in the right direction. Evidence of the potential benefits of a healthy lifestyle is accumulating, with prospective cohort studies indicating that physical activity, social activity, cognitive activity, avoiding smoking, moderate alcohol intake, maintenance of normal body weight, and healthy dietary patterns and nutrition reduce the risk of cognitive decline and dementia (24, 25). Recent interventional research further supports the beneficial effects of physical activity on cognitive functioning (26). More recently, multicomponent lifestyle interventions, including a combination of exercise, nutrition, cognitive training, and management of vascular risk factors, are being conducted to examine the effects of multiple health behavior change on cognitive impairment and dementia in older adults (27). Also, considering that lifestyle risks are prevalent throughout the lifespan, it is important to adopt prevention strategies that target specific stages of the life course. Improving education and living conditions early in life, reducing midlife vascular risk factors such as obesity and hypertension, and encouraging participation in physical, social, and mental activities in late life may help to maintain cognitive health through different phases of life.
The government and the healthcare system must also be prepared to address this problem. At the national level, policies and programs that support dementia prevention efforts are urgently needed. To this end, the Dementia Management Act, enacted in 2011, is anticipated to help direct resources to dementia prevention projects. Healthcare financing, with its currently disproportionate compensation for administering therapeutic interventions, needs restructuring to incentivize providers to deliver effective health promotion and preventive services. Priority should be assigned to support prevention research and program development that informs policy and practice.
CONCLUSION
The epidemic of dementia is at our doorstep. Fortunately, means are available to counter this threat. The non-communicable disease care paradigms that have been shown to be effective in controlling chronic conditions apply equally to dementia (1). Health promotion programs that emphasize healthy lifestyle behaviors need to be developed, using a life course approach. Reducing vascular risk factors by effective management of chronic conditions in midlife would be important. The public health infrastructure needs to be improved, raising the level of education and living conditions in early as well as in late life, enhancing community-based preventive services, and providing efficient delivery of health care. National initiatives need to be put forward that direct attention to promoting and protecting cognitive health throughout the lifespan. With coordinated efforts by the research community, public and private institutions, and government agencies to develop and implement effective prevention strategies nationwide, curbing the escalating dementia epidemic may not prove to be such an unattainable goal.
ACKNOWLEDGMENTS
A part of this paper has been presented at the Fourth Academic Forum of the National Academy of Medicine of Korea, held on September 26, 2013 in Seoul, Korea.
Footnotes
Funding: This study was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (HI10C2020).
The author has no potential conflicts of interest to disclose.
References
- 1.World Health Organization and Alzheimer's Disease International. Dementia: a public health priority. Geneva: World Health Organization; 2012. [Google Scholar]
- 2.Ministry of Health and Welfare. 2012 study on the prevalence of dementia. Seoul: Ministry of Health and Welfare; 2012. [Google Scholar]
- 3.Statistics Korea. Population projections for Korea: 2010-2060. Daejeon: Statistics Korea; 2012. [accessed on 5 January 2014]. Available at http://kosis.kr/ups/ups_02List01.jsp?kor_id=&pubcode=PJ&type=F. [Google Scholar]
- 4.Alzheimer's Disease International. World Alzheimer report 2010: the global economic impact of dementia. London: Alzheimer's Disease International; 2010. [accessed on 11 October 2013]. Available at http://www.alz.co.uk/research/files/WorldAlzheimerReport2010.pdf. [Google Scholar]
- 5.Ministry of Health and Welfare. Status of older people with dementia in Korea. Seoul: Ministry of Health and Welfare; 2011. [Google Scholar]
- 6.Alzheimer's Disease International. World Alzheimer report 2009. London: Alzheimer's Disease International; 2009. [accessed on 23 October 2013]. Available at http://www.alz.co.uk/research/files/WorldAlzheimerReport.pdf. [Google Scholar]
- 7.Manton KC, Gu XL, Ukraintseva SV. Declining prevalence of dementia in the U.S. elderly population. Adv Gerontol. 2005;16:30–37. [PubMed] [Google Scholar]
- 8.Lobo A, Saz P, Marcos G, Dia JL, De-la-Camara C, Ventura T, Montañes JA, Lobo-Escolar A, Aznar S ZARADEMP Workgroup. Prevalence of dementia in a southern European population in two different time periods: the ZARADEMP Project. Acta Psychiatr Scand. 2007;116:299–307. doi: 10.1111/j.1600-0447.2007.01006.x. [DOI] [PubMed] [Google Scholar]
- 9.Langa KM, Larson EB, Karlawish JH, Cutler DM, Kabeto MU, Kim SY, Rosen AB. Trends in the prevalence and mortality of cognitive impairment in the United States: is there evidence of a compression of cognitive morbidity. Alzheimers Dement. 2008;4:134–144. doi: 10.1016/j.jalz.2008.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rocca WA, Petersen RC, Knopman DS, Hebert LE, Evans DA, Hall KS, Gao S, Unverzagt FW, Langa KM, Larson EB, et al. Trends in the incidence and prevalence of Alzheimer's disease, dementia, and cognitive impairment in the United States. Alzheimers Dement. 2011;7:80–93. doi: 10.1016/j.jalz.2010.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Matthews FE, Arthur A, Barnes LE, Bond J, Jagger C, Robinson L, Brayne C Medical Research Council Cognitive Function and Ageing Collaboration. A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: results of the Cognitive Function and Ageing Study I and II. Lancet. 2013;382:1405–1412. doi: 10.1016/S0140-6736(13)61570-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Christensen K, Thinggaard M, Oksuzyan A, Steenstrup T, Andersen-Ranberg K, Jeune B, McGue M, Vaupel JW. Physical and cognitive functioning of people older than 90 years: a comparison of two Danish cohorts born 10 years apart. Lancet. 2013;382:1507–1513. doi: 10.1016/S0140-6736(13)60777-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schrijvers EM, Verhaaren BF, Koudstaal PJ, Hofman A, Ikram MA, Breteler MM. Is dementia incidence declining? trends in dementia incidence since 1990 in the Rotterdam Study. Neurology. 2012;78:1456–1463. doi: 10.1212/WNL.0b013e3182553be6. [DOI] [PubMed] [Google Scholar]
- 14.Qiu C, von Strauss E, Bäckman L, Winblad B, Fratiglioni L. Twenty-year changes in dementia occurrence suggest decreasing incidence in central Stockholm, Sweden. Neurology. 2013;80:1888–1894. doi: 10.1212/WNL.0b013e318292a2f9. [DOI] [PubMed] [Google Scholar]
- 15.Brookmeyer R, Gray S, Kawas C. Projections of Alzheimer's disease in the United States and the public health impact of delaying disease onset. Am J Public Health. 1998;88:1337–1342. doi: 10.2105/ajph.88.9.1337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM. Forecasting the global burden of Alzheimer's disease. Alzheimers Dement. 2007;3:186–191. doi: 10.1016/j.jalz.2007.04.381. [DOI] [PubMed] [Google Scholar]
- 17.Jang SN, Kim DH. Trends in the health status of older Koreans. J Am Geriatr Soc. 2010;58:592–598. doi: 10.1111/j.1532-5415.2010.02744.x. [DOI] [PubMed] [Google Scholar]
- 18.Chung KH, Cho AJ, Oh YH, Byun JK, Byun YC, Moon HS. 1998 survey on the Living Status and Welfare Needs of Older People. Seoul: Korea Institute of Health and Social Affairs; 1998. [Google Scholar]
- 19.Chung KH, Oh YH, Lee YK, Sohn CK, Lee SY, Lee JH, Kwon JD, Kim SB, Lee SJ, Lee YS, et al. 2011 survey on the Living Status of Older People. Seoul: Korea Institute of Health and Social Affairs; 2012. [accessed on 12 December 2013]. Available at https://www.kihasa.re.kr/html/jsp/publication/policy/list.jsp. [Google Scholar]
- 20.Yeo YJ, Kim MG, Kwon MI, Choi OK, Choi JY. Old-age poverty in Korea and how should the government reduce it. Seoul: Korea Institute for Health and Social Affairs; 2012. [accessed on 11 January 2014]. Available at https://www.kihasa.re.kr/html/jsp/publication/research/list.jsp?key=title&ryear_value=2014&query=%BA%F3%B0%EF. [Google Scholar]
- 21.Kim HC, Oh SM. Noncommunicable diseases: current status of major modifiable risk factors in Korea. J Prev Med Public Health. 2013;46:165–172. doi: 10.3961/jpmph.2013.46.4.165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dodge HH, Buracchio TJ, Fisher GG, Kiyohara Y, Meguro K, Tanizaki Y, Kaye JA. Trends in the prevalence of dementia in Japan. Int J Alzheimers Dis. 2012;2012:956354. doi: 10.1155/2012/956354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Barnes DE, Yaffe K. The projected effect of risk factor reduction on Alzheimer's disease prevalence. Lancet Neurol. 2011;10:819–828. doi: 10.1016/S1474-4422(11)70072-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lee Y, Back JH, Kim J, Kim SH, Na DL, Cheong HK, Hong CH, Kim YG. Systematic review of health behavioral risks and cognitive health in older adults. Int Psychogeriatr. 2010;22:174–187. doi: 10.1017/S1041610209991189. [DOI] [PubMed] [Google Scholar]
- 25.Lee Y, Na DL, Cheong HK, Hong CH, Back JH, Kim J, Kim SH, Kim YG. Lifestyle recommendations for dementia prevention: PASCAL. J Korean Geriatr Soc. 2009;13:61–68. [Google Scholar]
- 26.Lövdén M, Xu W, Wang HX. Lifestyle change and the prevention of cognitive decline and dementia: what is the evidence? Curr Opin Psychiatry. 2013;26:239–243. doi: 10.1097/YCO.0b013e32835f4135. [DOI] [PubMed] [Google Scholar]
- 27.Andrieu S, Aboderin I, Baeyens JP, Beard J, Benetos A, Berrut G, Brainin M, Cha HB, Chen LK, Du P, et al. IAGG workshop: health promotion program on prevention of late onset dementia. J Nutr Health Aging. 2011;15:562–575. doi: 10.1007/s12603-011-0142-1. [DOI] [PubMed] [Google Scholar]