

Abstract
Objective
The objective of this study was to compare the incidence of ventricular shunt placement for shunt-dependent hydrocephalus (SDHC) after clipping versus coiling of ruptured aneurysms.
Materials and Methods
A retrospective review was conducted in 215 patients with aneurysmal subarachnoid hemorrhage (SAH) who underwent surgical clipping or endovascular coiling during the period from May 2008 to December 2011. Relevant clinical and radiographic data were analyzed with regard to the incidence of hydrocephalus and ventriculo-peritoneal shunt (VPS). Patients treated with clipping were assigned to Group A, while those treated with coiling were assigned to Group B.
Results
Of 215 patients (157 clipping, 58 coiling), no significant difference in the incidence of final VPS was observed between treatment modalities (15.3% vs. 10.3%) (p = 0.35). Independent risk factors for VPS for treatment of chronic hydrocephalus were as follows: (1) older than 65 years, (2) poorer Hunt-Hess grade IV and V, (3) Fisher grade III and IV, and (4) particularly initial presence of an intraventricular hemorrhage.
Conclusion
In this study comparing two modalities for treatment of aneurysm, there was no difference in the incidence of chronic hydrocephalus requiring VPS. A significantly higher rate of shunt dependency was observed for age older than 65 years, poor initial neurological status, and thick SAH with presence of initial intraventricular hemorrhage. By understanding these factors related to development of SDHC and results, it is expected that management of aneurysmal SAH will result in a better prognosis.
Keywords: Acute hydrocephalus, Chronic hydrocephalus, Subarachnoid hemorrhage, Lumbar drain
INTRODUCTION
Chronic hydrocephalus after occlusion of ruptured aneurysmal subarachnoid hemorrhage (SAH) has been reported to range from 6 to 67%.16) The location of the aneurysm, initial mental status, and presence of initial intraventricular hemorrhage (IVH) are risk factors for development of chronic hydrocephalus.11),19),21),22),26) In addition, the amount of hemorrhage in the subarachnoid space and ventricular system has a strong association with development of hydrocephalus.4),5),7),12)
Acute hydrocephalus develops through obstructive mechanisms when blood clot and products disrupt the cerebrospinal fluid (CSF) pathway. In contrast, chronic hydrocephalus may occur through a different mechanism where the adhesion obstructs the CSF circulation.2),3),6),8),10),15),18),26)
Due to advances in endovascular techniques, comparison of the incidence of shunt-dependent hydrocephalus (SDHC) after clipping versus coiling of ruptured aneurysms is very important. Their relative effectiveness of these procedures has yet to be clearly determined in the literature. Results of one study showed a lower incidence of shunt-dependent hydrocephalus in the surgical treatment group.7) In another study, no difference was observed between the clipping group and the coiling group.12)
Therefore, our objective is to analyze the incidence of SDHC between the surgical clipping and endovascular coiling groups. We also evaluate the variables affecting ventriculo-peritoneal shunt (VPS) after clipping or coiling of ruptured aneurysmal SAH.
MATERIALS AND METHODS
Patients
A total of 215 patients with aneurysmal SAH who underwent surgical clipping or endovascular coil embolization during the period from May 2008 to December 2011 were included in the current study. Relevant clinical and radiographic data regarding the incidence of hydrocephalus and VPS were analyzed. Patients treated with surgical clipping were assigned to Group A, while those treated with endovascular coiling were assigned to Group B.
Patients were initially diagnosed with SAH by brain computed tomography (CT) scan. CT angiography or digital subtraction angiography (DSA) was performed in order to confirm the ruptured aneurysm. The clinical characteristics of the patients were obtained from their medical records and imaging studies.
Treatment modality
The treatment modality for the ruptured aneurysmal SAH was determined by a vascular neurosurgeon. The patient's clinical status, location of the aneurysm, and the angioarchitecture of the aneurysm were factors used in determination of the treatment modality. The indications for endovascular coil embolization were dependent upon the surgeon's discretion; surgical difficulty causing potential complications, patients' refusal of craniotomy, elderly patients, or poor medical condition.
Acute hydrocephalus was defined as development of ventricle enlargement on the basis of the third ventricle width and periventricular low density on CT scan within 72 hours of the aneurismal rupture, and as a clinical manifestation such as mental deterioration, memory impairment, gait disturbance, and urinary incontinence. Patients presenting with clinical deterioration with radiologic evidence of acute hydrocephalus underwent immediate external ventricular drainage (EVD). Other patients who had radiologic evidence of acute hydrocephalus, but did not present with any clinical deterioration, underwent lumbar drainage (LD). In patients who underwent EVD, drainage was maintained for at least seven days after the ruptured aneurysmal SAH. Before removal of the EVD, the drainage was clamped for 24 hours and if the patient showed no neurological deterioration, a control brain CT was performed. If the control CT did not show any change of ventricle size, the EVD was removed. When the SAH was resolved in a follow-up CT scan, the LD was removed. Before removal of the lumbar drainage, the same protocol was performed with the patients who had EVD. If there was any neurological deterioration or if the control CT results demonstrated ventricle enlargement after clamping the drainage, patients underwent ventriculo-peritoneal shunt (VPS) insertion at least four weeks after SAH.
SDHC was defined as clinical symptoms of hydrocephalus, including gait disturbance, urinary incontinence, and dementia with radiologic evidence of enlarged ventricles requiring VPS.
Statistical analysis
A two-sample t-test and a chi-square test of independence were used for comparison between the therapeutic groups (Group A and Group B). In this study, a probability value of less than 0.05 was considered statistically significant.
Univariate logistic regression model was used for analysis of the risk factors for shunt-dependent hydrocephalus.
In comparison of the surgical clipping group and the endovascular coiling group, we analyzed the following factors: 1) age, 2) sex, 3) initial Hunt & Hess grade, 4) initial Fisher grade, 5) presence of initial IVH, 6) presence of acute hydrocephalus, and 7) location of the aneurysm (Anterior circulation: internal carotid artery, posterior communicating artery, middle cerebral artery, anterior cerebral artery, or anterior communicating artery, posterior circulation: vertebral artery, basilar artery, posterior cerebral artery, posterior-inferior cerebellar artery, anterior-inferior cerebellar artery, or superior cerebellar artery). The patients' data were analyzed according to each treatment modality (the clipping group versus the coiling group), and the risk factors were analyzed for each subgroup.
RESULTS
The mean age of the patients was 56.5 years (range 27-79 years). The female to male ratio was 1.9:1. Surgical clipping by fronto-temporal craniotomy or posterior fossa craniotomy was performed in 157 patients. Most patients underwent surgery by the pterional approach. If necessary, evacuation of intraparenchymal hematoma and fenestration of lamina terminalis were performed during the surgical clipping. Endovascular coil embolization with or without stent insertion was performed in 58 patients with ruptured aneurysmal SAH. The patient demographics and characteristics of the ruptured aneurysmal SAH are shown in Table 1.
Table 1.
Patient demographics and characteristics in both treatment groups
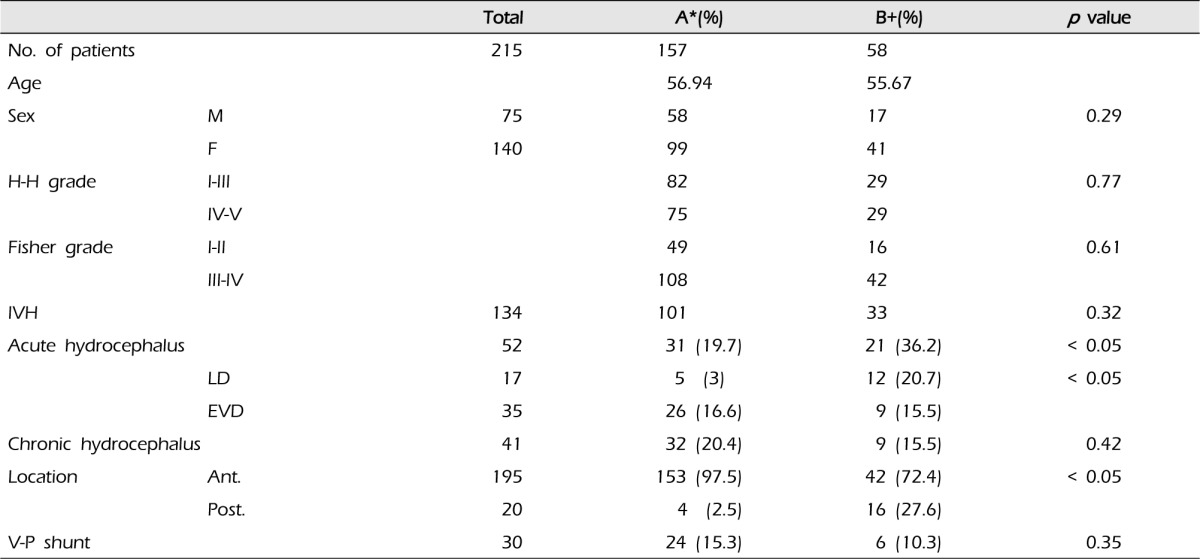
*Group A, Patients treated with clipping were assigned to; +Group B, Patients treated with coiling were assigned to; Two-sample t-test and a Chi-square test were used.
No = number; M = male; F = female; H-H = Hunt-Hess; IVH = intraventricular hemorrhage; LD = lumbar drainage; EVD = external ventricular drainage; Ant = anterior; Post = posterior; V-P = ventriculo-peritoneal
Shunt-dependent hydrocephalus according to the treatment modality (clipping group versus coiling group)
Thirty patients (14.0% of the total patients) underwent ventriculo-peritoneal shunt insertion for treatment of chronic hydrocephalus. According to the two-sample t-test, the incidence of shunt-dependent hydrocephalus was 15.3% (24 of 157 patients) in the surgical clipping group and 10.3% (six of 58 patients) in the endovascular coiling group. No significant difference in the incidence of final VPS was observed between treatment modalities (p = 0.35) (Table 2).
Table 2.
Relating factors of shunt dependency in aneurysmal SAH patients
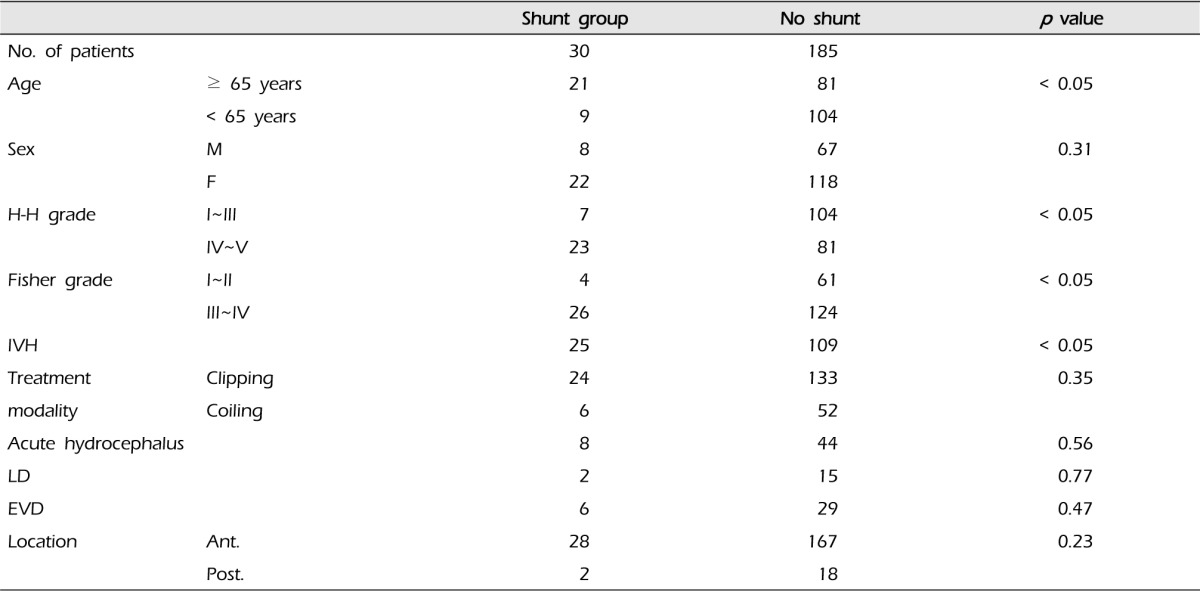
Two-sample t-test and a Chi-square test were used.
SAH = subarachnoid hemorrhage; M = male; F = female; H-H = Hunt-Hess; IVH = intraventricular hemorrhage; LD = lumbar drainage; EVD = external ventricular drainage; Ant = anterior; Post = posterior
Age, sex, H-H grade, Fisher grade, and presence of initial IVH were similar factors between the two groups. The number of patients having acute hydrocephalus and the number of posterior circulation aneurysms were factors that were more frequent in the coiling group.
Risk factors for shunt-dependent hydrocephalus after ruptured aneurysmal SAH
According to results of univariate analysis, older age (≥ 65 years), poor H-H grade (grade IV and V) and Fisher grade (grade III and IV) and presence of initial IVH were risk factors for development of SDHC (p < 0.05) (Table 3). Of 30 patients who underwent VPS, 23 (76.7%) patients presented with a poor H-H grade and 26 (86.7%) patients presented with Fisher grade III and IV. Twenty five (83.3%) of 30 patients initially had IVH on the brain CT scan (Table 2).
Table 3.
Factors associated with shunt-dependent hydrocephalus

Univariatelogistic regression model was used.
CI = confidence interval; IVH = intraventricular hemorrhage; H-H = Hunt-Hess
LD or EVD for acute hydrocephalus
LD was performed in 3% (five of 157 patients) of patients in the surgical clipping group and 20.7% (12 of 58 patients) of patients in the endovascular coiling group. Due to the difference in the location of the aneurysm between the two groups, LD was performed more in the coiling group. In the LD group, development of shunt-dependent hydrocephalus finally occurred in only two of 17 patients.
EVD was performed in 16.6% (26 of 157 patients) of patients in the surgical clipping group and 15.5% (nine of 58 patients) of patients in the endovascular coiling group. In the EVD group, development of shunt-dependent hydrocephalus finally occurred in 17.1% of patients (six of 35 patients).
DISCUSSION
Development of acute or chronic hydrocephalus after SAH can result in neurological deterioration, one of the representative complications of aneurysmal SAH after occlusion of a ruptured aneurysm.1)
During clipping surgery for ruptured aneurysmal SAH, both mechanical clot removal and lamina terminalis fenestration are possible.12) It might improve CSF dynamics and prevent progression of chronic hydrocephalus.
On the other hand, removal of the SAH is not possible during an endovascular coiling procedure. Several studies have suggested that the incidence of SDHC is higher for endovascular coiling than for surgical clipping. Dorai et al. and Varelas et al. reported a higher incidence of SDHC in the coiling group than in the clipping group.7),25) During surgical clipping, irrigation and early evacuation of SAH are possible and it may result in more rapid clearance of the blood and decreases the incidence of SDHC. However, they did not consider the initial lumbar drainage, which might lower the incidence of hydrocephalus. Therefore, the advantage of the lumbar drainage was underestimated.4) For this reason, findings of their study showed a higher incidence of SDHC in the coiling group than in the clipping group.
However, according to the results of this study, compared to surgical clipping, the endovascular coiling procedure is not a risk factor for development of SDHC. Some studies reported similar results in that no significant difference in the incidence of SDHC was observed between the clipping group and the coiling group.4),5),12)
The treatment modality for the ruptured aneurysmal SAH is not a risk factor for development of SDHC (clipping: 15.3%, coiling: 10.3%, p = 0.35). However, according to the initial neurological status and presence of the initial IVH, there were some differences in the incidence of SDHC (Table 2). A much more significant association with acute hydrocephalus was observed for the endovascular coiling group. In contrast, the anterior circulation aneurysm was found more frequently in the clipping group than in the coiling group. Due to the difference in the aneurysm location between the two groups, the initial LD procedure was performed more in the coiling group.
The advantage of continuous LD in lowering the incidence of hydrocephalus has been reported in the literature.5),9),14),15),16),17),20),23) Initial lumbar drainage in patients with ruptured aneurysmal SAH promotes circulation of CSF from the ventricles through the subarachnoid space, and it can wash out the bloody CSF from the spinal cistern. Drainage of CSF from the ventricles may actually promote circulation of CSF within the subarachnoid space; this is the role of lumbar drainage in aneurysmal SAH patients. Thus, it may lower the incidence of SDHC. In comparison of our study with previous studies, the incidence of SDHC in coiled patients was much lower than in previous studies (Table 4). Removal of the SAH is not possible during an endovascular coiling procedure; however, the LD might lower the incidence of SDHC. Due to the different protocol, assessment of statistically significant correlations between LD and incidence of SDHC was not possible.
Table 4.
Comparison of incidence of shunt-dependent hydrocephalus with other studies

Two-sample t-test and a Chi-square test were used.
In the current study, we identified several risk factors associated with development of SDHC in patients after SAH. According to results of univariate analysis, older age (≥ 65 years), poor H-H grade IV and V, poor Fisher grade III, and IV and presence of initial IVH were all significant predictors of chronic hydrocephalus (Table 3). Factors associated with development of SDHC identified in many studies may vary from study to study. However, age, female sex, location of aneurysm, poor neurological status, presence of initial IVH, and the amount of hemorrhage in the subarachnoid space have all generally been associated with a higher incidence of SDHC.4)
Our study has some limitations. This study is a retrospective study; therefore, selection bias was inevitable. In addition, the treatment modality was dependent upon the surgeon's discretion. The number of patients in each group was not similar, such that there were 157 patients in the clipping group and 58 patients inthe coiling group. In addition, the location of the aneurysms was not evenly distributed in either group. This discrepancy is due to the fact that in our institution, the majority of ruptured aneurismal SAH is still being treated by surgical clipping. Thus, a prospective, multicenter, and well stratified protocol will be needed for comparison of the incidence of ventriculo-peritoneal shunt placement for shunt-dependent hydrocephalus (SDHC) after clipping versus coiling of ruptured aneurysmal SAH.
CONCLUSION
In this study, treatment modality showed no statistical significance with regard to the incidence of SDHC. A significantly higher rate of shunt dependency was observed for age older than 65 years, poor initial neurological status, and thick SAH with presence of initial IVH. By understanding these factors related to development of SDHC, it is expected that management of aneurysmal SAH will result in a better prognosis. However, a randomized and prospective study of treatment modality with or without the use of lumbar drainage will be able to overcome the limitations of our study.
Footnotes
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
References
- 1.Auer LM, Mokry M. Disturbed cerebrospinal fluid circulation after subarachnoid hemorrhage and acute aneurysm surgery. Neurosurgery. 1990 May;26(5):804–808. doi: 10.1097/00006123-199005000-00012. discussion 808-9. [DOI] [PubMed] [Google Scholar]
- 2.Blasberg R, Johnson D, Fenstermacher J. Absorption resistance of cerebrospinal fluid after subarachnoid hemorrhage in the monkey, effects of heparin. Neurosurgery. 1981 Dec;9(6):686–691. doi: 10.1227/00006123-198112000-00012. [DOI] [PubMed] [Google Scholar]
- 3.Brydon HL, Bayston R, Hayward R, Harkness W. The effect of protein and blood cells on the flow-pressure characteristics of shunts. Neurosurgery. 1996 Mar;38(3):498–504. doi: 10.1097/00006123-199603000-00016. discussion 505. [DOI] [PubMed] [Google Scholar]
- 4.de Oliveira JG, Beck J, Setzer M, Gerlach R, Vatter H, Seifert V, et al. Risk of shunt-dependent hydrocephalus after occlusion of ruptured intracranial aneurysms by surgical clipping or endovascular coiling: a single-institution series and meta-analysis. Neurosurgery. 2007 Nov;61(5):924–933. doi: 10.1227/01.neu.0000303188.72425.24. discussion 933-4. [DOI] [PubMed] [Google Scholar]
- 5.Dehdashti AR, Rilliet B, Rufenacht DA, de Tribolet N. Shunt-dependent hydrocephalus after rupture of intracranial aneurysms: a prospective study of the influence of treatment modality. J Neurosurg. 2004 Sep;101(3):402–407. doi: 10.3171/jns.2004.101.3.0402. [DOI] [PubMed] [Google Scholar]
- 6.Donauer E, Reif J, al-Khalaf B, Mengedoht EF, Faubert C. Intraventricular haemorrhage caused by aneurysms and angiomas. Acta Neurochir (Wien) 1993;122(1-2):23–31. doi: 10.1007/BF01446982. [DOI] [PubMed] [Google Scholar]
- 7.Dorai Z, Hynan LS, Kopitnik TA, Samson D. Factors related to hydrocephalus after aneurysmal subarachnoid hemorrhage. Neurosurgery. 2003 Apr;52(4):763–769. doi: 10.1227/01.neu.0000053222.74852.2d. discussion 769-71. [DOI] [PubMed] [Google Scholar]
- 8.Ellington E, Margolis G. Block of arachnoid villus by subarachnoid hemorrhage. J Neurosurg. 1969 Jun;30(6):651–657. doi: 10.3171/jns.1969.30.6.0651. [DOI] [PubMed] [Google Scholar]
- 9.Fulop B, Deak G, Mencser Z, Kuncz A, Barzo P. [Factors affecting the development of chronic hydrocephalus following subarachnoid hemorrhage, with special emphasis on the role of ventricular and lumbar drainage] Ideggyogy Sz. 2009 Jul;62(7-8):255–261. Hungarian. [PubMed] [Google Scholar]
- 10.Ginsberg LE, Moody DM. Meningiomas: imaging. In: Wilkins RH, Rengachary SS, editors. Neurosurgery. ed 2. Vol 1. New York: McGraw-Hill; 1996. pp. 855–872. [Google Scholar]
- 11.Graff-Radford NR, Torner J, Adams HP, Jr, Kassell NF. Factors associated with hydrocephalus after subarachnoid hemorrhage. A report of the Cooperative Aneurysm Study. Arch Neurol. 1989 Jul;46(7):744–752. doi: 10.1001/archneur.1989.00520430038014. [DOI] [PubMed] [Google Scholar]
- 12.Gruber A, Reinprecht A, Bavinzski G, Czech T, Richling B. Chronic shunt-dependent hydrocephalus after early surgical and early endovascular treatment of ruptured intracranial aneurysms. Neurosurgery. 1999 Mar;44(3):503–509. doi: 10.1097/00006123-199903000-00039. discussion 509-12. [DOI] [PubMed] [Google Scholar]
- 13.Hasan D, Tanghe HL. Distribution of cisternal blood in patients with acute hydrocephalus after subarachnoid hemorrhage. Ann Neurol. 1992 Apr;31(4):374–378. doi: 10.1002/ana.410310405. [DOI] [PubMed] [Google Scholar]
- 14.Hasan D, Vermeulen M, Wijdicks EF, Hijdra A, van Gijn J. Management problems in acute hydrocephalus after subarachnoid hemorrhage. Stroke. 1989 Jun;20(6):747–753. doi: 10.1161/01.str.20.6.747. [DOI] [PubMed] [Google Scholar]
- 15.Hoekema D, Schmidt RH, Ross I. Lumbar drainage for subarachnoid hemorrhage: technical considerations and safety analysis. Neurocrit Care. 2007;7(1):3–9. doi: 10.1007/s12028-007-0047-3. [DOI] [PubMed] [Google Scholar]
- 16.Kasuya H, Shimizu T, Kagawa M. The effect of continuous drainage of cerebrospinal fluid in patients with subarachnoid hemorrhage: a retrospective analysis of 108 patients. Neurosurgery. 1991 Jan;28(1):56–59. doi: 10.1097/00006123-199101000-00009. [DOI] [PubMed] [Google Scholar]
- 17.Kasuya H, Shimizu T, Okada T, Takahashi K, Summerville T, KitamuraK [A study of continuous cerebrospinal fluid drainage in patients with subarachnoid hemorrhage] No Shinkei Geka. 1988;16(5 Suppl):475–481. Japanese. [PubMed] [Google Scholar]
- 18.Kibler RF, Couch RS, Crompton MR. Hydrocephalus in the adult following spontaneous subarachnoid hemorrhage. Brain. 1961 Mar;84:45–61. doi: 10.1093/brain/84.1.45. [DOI] [PubMed] [Google Scholar]
- 19.Kwon JH, Sung SK, Song YJ, Choi HJ, Huh JT, Kim HD. Predisposing factors related to shunt-dependent chronic hydrocephalus after aneurysmal subarachnoid hemorrhage. J Korean Neurosurg Soc. 2008 Apr;43(4):177–181. doi: 10.3340/jkns.2008.43.4.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Macdonald RL. Lumbar drainage after subarachnoid hemorrhage: does it reduce vasospasm and delayed hydrocephalus? Neurocrit Care. 2007;7(1):1–2. doi: 10.1007/s12028-007-0046-4. [DOI] [PubMed] [Google Scholar]
- 21.Pietilä TA, Heimberger KC, Palleske H, Brock M. Influence of aneurysm location on the development of chronic hydrocephalus following SAH. Acta Neurochir (Wien) 1995;137(1-2):70–73. doi: 10.1007/BF02188784. [DOI] [PubMed] [Google Scholar]
- 22.Spallone A, Gagliardi FM. Hydrocephalus following aneurysmal SAH. Zentralbl Neurochir. 1983;44(2):141–150. [PubMed] [Google Scholar]
- 23.Vale FL, Bradley EL, Fisher WS., 3rd The relationship of subarachnoid hemorrhage and the need for postoperative shunting. J Neurosurg. 1997 Mar;86(3):462–466. doi: 10.3171/jns.1997.86.3.0462. [DOI] [PubMed] [Google Scholar]
- 24.van Gijn J, Hijdra A, Wijdicks EF, Vermeulen M, van Crevel H. Acute hydrocephalus after aneurysmal subarachnoid hemorrhage. J Neurosurg. 1985 Sep;63(3):355–362. doi: 10.3171/jns.1985.63.3.0355. [DOI] [PubMed] [Google Scholar]
- 25.Varelas P, Helms A, Sinson G, Spanaki M, Hacein-Bey L. Clipping or coiling of ruptured cerebral aneurysms and shunt-dependent hydrocephalus. Neurocrit Care. 2006;4(3):223–228. doi: 10.1385/NCC:4:3:223. [DOI] [PubMed] [Google Scholar]
- 26.Vermeij FH, Hasan D, Vermeulen M, Tanghe HL, van Gijn J. Predictive factors for deterioration from hydrocephalus after subarachnoid hemorrhage. Neurology. 1994 Oct;44(10):1851–1855. doi: 10.1212/wnl.44.10.1851. [DOI] [PubMed] [Google Scholar]