

Abstract
Backround: Local anesthetic infiltration applied on the wound site or abdominal wall may be used for relieving postoperative pain after delivery by caesarean section. The aim of this study was to compare the analgesic efficiency of ultrasound (USG)-guided transversus abdominis plane (TAP) block with local anesthetic infiltration on a wound site.
Methods: This study was designed as a prospective randomized trial, and consisted of 70 pregnant women of American Society of Anesthesiologists (ASA) class I-II. Patients were randomized into Group I (wound site infiltration, n=35) and Group T (TAP block, n=35). Spinal anaesthesia was administered to all patients. In Group I, wound site infiltration was applied by the surgical team. In Group T, a USG-guided bilateral TAP block was applied. Patients’ numeric pain scale (NPS) levels at 2, 6, 12 and 24th hours, after the operation (NPS0) and during mobilization were assessed. Postoperative complications, time to first analgesic request and patient satisfaction were recorded.
Results: The NPS0 values of Group T were found to higher and time to first analgesic request longer than those of Group I. The NPS values of Group I at 2, 6, 12, and 24th hours were found to be statistically significantly higher than those of Group T.
Conclusions: According to our results, USG-guided TAP block might be superior to infiltration anaesthesia for postoperative pain management of patients who have had caesarean section and it provided longer-lasting and more efficient analgesia.
Keywords: Ultrasound, transversus abdominis plane block, infiltration anaesthesia, cesarean section
Introduction
Long acting local anesthetics administered to both sides of the wound site or on/under the skin after surgery have been demonstrated to be effective for postoperative analgesia1,2. It has been reported that, in addition to general or regional anaesthesia, local anesthetic infiltration and abdominal wall blocks are also useful for postoperative analgesia in cases of delivery by caesarean section3.
Transversus abdominis plane (TAP) block is a newly defined block that covers the nerves of the abdominal front wall. It was developed for postoperative pain control after gynecological and abdominal surgeries. Transversus abdominis plane block provides effective analgesia as part of a multimodal analgesic regimen for surgical procedures such as open appendectomy, laparoscopic cholecystectomy, hysterectomy, caesarean section, and large intestine resection performed by midline abdominal incision4,5. Our aim was to compare the efficiency of ultrasound (USG)-guided TAP block with wound site infiltration anaesthesia. Our primary endpoints were pain scores at 0, 2, 6, 12 and 24 hours after surgery and patient satisfaction and our secondary endpoints were postoperative complications of the TAP block and wound infiltration approaches for postoperative analgesia and postoperative first analgesic application time.
Methods
After obtaining the approval of the ethics committee and the informed consent of the patients, a prospective randomized, double blinded study was undertaken of patients over 18 years old scheduled to caesarean section in Bagcılar Training and Research Hospital. Seventy pregnant women of American Society of Anesthesiologists (ASA) class I-II were involved in the study, which was completed in a 4-month period.
Elective cases with an eight-hour fast were included in the study; emergency cases were excluded. Patients with spinal anaesthesia contraindications (e.g., coagulopathy, infection at puncture site) and those not wanting spinal anaesthesia were also excluded.
Before initiation, peripheral vascular access was obtained with a 16 or 18-gauge (G) intravenous cannula in all patients and preoperatively 8 mL kg-1 h-1 NaCl 0.9% was infused. General anaesthesia conditions, 0.50 mg atropine sulfate and 10 mg ephedrine were prepared for all patients. Patients’ standard monitoring was applied when they were taken to the operating table. Blood pressure (mmHg), heart rate (HR, beat min-1), and peripheral oxygen saturation (SpO2) values were tracked by noninvasive methods.
Patients were randomized into groups (Group I: Wound site infiltration, n=35 or Group T: TAP block, n=35) with the help of a computer by an anaesthesia nurse according to their arrival time. An experienced anesthesiologist, expert in TAP block, performed all spinal and TAP blocks on all patients; the spinal technique was performed with the patient in the sitting position. Using a midline approach, the intrathecal space was accessed by traversing the L3–L4 interval, with a 26-G Quincke needle (Exel Int, Los Angeles, CA). After confirmation of clear cerebrospinal fluid flow, 10 mg of hyperbaric bupivacaine (Heavy Marcaine 0.5%; Astra Zeneca, London, UK) plus fentanyl 20 μg were injected intrathecally. Only patients with successful spinal anaesthesia were included in the study.
In Group T, after the surgical procedure was acomplished, sterile skin cleaning was performed with patients lying on their backs, and the linear probe (5-10 mHz) of the USG device (SDU-450 XL, Kyoto, Japan) was prepared under sterile conditions. The probe was placed subcostally between the coastal margin and the iliac crest in the lateral abdominal wall, and the external oblique, internal oblique, and transversus abdominis muscles were identified. In the in-plane technique, a 100 mm 20-G peripheric blockage needle (B. Braun, Melsungen, Germany) was advanced, and local anesthetic medicine was administered over the transversus abdominis muscle. Forty mL (20 mL+20 mL, bilaterally) 100-mg levobupivacaine of 0.25% concentration was applied in Group T patients. All local anesthetics were prepared by the same co-investigator and the same co-investigator assisted during the whole TAP block procedure.
After the completion of the surgical procedure, in total 40 mL (20 ml for each wound site) 100-mg levobupivacaine of 0.25% concentration was used for subcutaneous wound site infiltration of the patients in Group I.
Intraoperative complications (nausea, vomiting, hypotension and bradycardia), postoperative complications (nausea, vomiting, hypotension, bradycardia and headache), need for analgesic, first postoperative analgesic administration time were recorded. Patient satisfaction was determined by asking the patients orally to provide a number between zero and ten (0: not satisfied, 10: satisfied a lot), and the number was recorded. Patient satisfaction evaluation was performed 24 hour after the the block.
Patient pain was evaluated by Numeric Pain Score (NPS), a scale of one to ten. The patients were asked to provide a number, with ten being the most violent pain they had ever had, and zero being no sensation of pain. In Group I NPS after local anaesthetic infiltration and in Group T NPS after TAP block was considered as NPS0 (zero). Patients were evaluated at the 2, 6, 12, 24th hours and at the first mobilization by a co-investigator, who was blind to the used method and asked for their pain scores and the same co-investigator recorded all pain scores. All patients were routinely mobilized 8 hours after the end of the operation. If the patient suffered from pain (NPS>3) at any hour, intramuscular diclofenac sodium 75 mg was adminestered and if this was not efficient, 50 mg of tramadol were also given intravenously.
The sample sizes were calculated with the assumption of a possible at least of 35% difference between the two groups. Therefore 35 patients were allocated into each group in order to obtain an alpha error of 5% and statistical power of 80%.
Statistical Analysis
Complementary statistical methods (mean, standard deviation, median, interquartile range) were used to evaluate the data. The following tests were conducted: Freidman test for repetitive measurement of variable groups not showing normal distribution; Dunn’s multi-comparison test for comparisons of subgroups; Mann-Whitney U test for comparisons of binary groups; independent t test for comparison of binary groups of variables showing normal distribution; and chi square test for comparisons of qualitative data. Results were considered statistically significant when p value was under 0.05.
Results
All applied TAP blocks were successful. No statistically significant differences were observed in age (p=0.341), body weight (p=0.271), or pregnancy frequency (p=0.912) between the groups (Table 1).
Table 1. Age, body weight and number of pregnancy in Group I (wound site infiltration, n=35) and Group T (TAP block, n=35).

Presented as Mean ± Standard Deviation.
No statistically significant differences were observed in ASA scores (p=0.077), allergy history (p=1), or incidence of complications (p=0.060) between the groups. In both groups, intraoperative complications were hypotension and bradycardia. No postoperative complications were observed in any of the patients (Table 2).
Table 2. ASA score, allergy history and intraoperative complications in Group I (wound site infiltration, n=35) and Group T (TAP block, n=35).
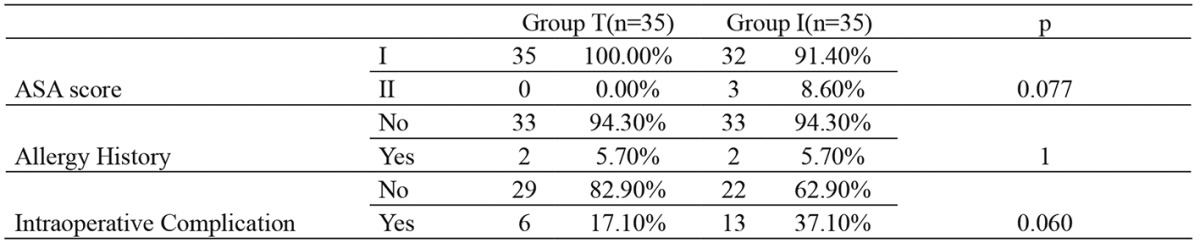
ASA: American Society of Anesthesiology.
The NPS0 values of Group T were found to be significantly higher than those of Group I (p=0.012). The NPS values of Group I at 2, 6, 12 and 24th hours were found to be statistically and clinically significant higher than those of Group T (p=0.005, p=0.003, p=0.0001, p=0.0001). No statistically significant differences between the groups were observed in NPS values during the first mobilization (p=0.123) (Table 3).
Table 3. Numeric Pain Scale in Group I (wound site infiltration, n=35) and Group T (TAP block, n=35).
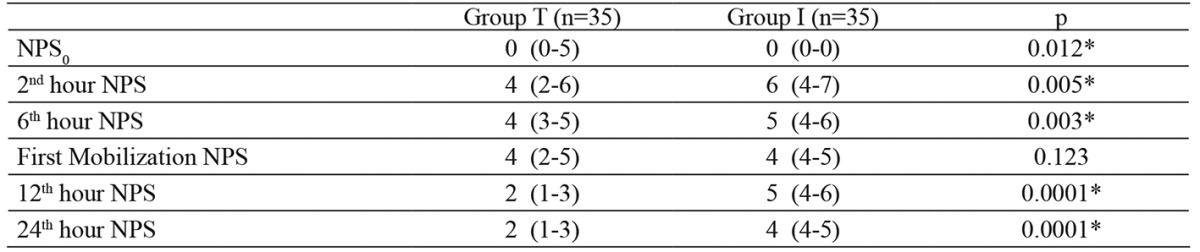
NPS: Numeric Pain Scale, * p<0.05.
The first analgesic administration of Group T (p=0.003) was found to be significantly later than that in Group I. No statistically significant difference was observed between the groups in patient satisfaction means (p=0.081) (Table 4).
Table 4. Postoperative first analgesic application time and patient satisfaction in groups.

Presented as Mean ± Standard Deviation, *pp<0.05.
Discussion
Bamigboye et al3 compared wound site infiltration with a placebo in patients who had caesarean sections with regional anaesthesia and reported that NPS at first hour with wound site infiltration was lower. It has also been reported that wound site infiltration applied as a single dose for pain relief after caesarean section is an active, reliable, and simple method for the first four hours postpartum6. Similarly, in our study, NPS scores (NPS0) after surgery were lower in Group I than in Group T. We are concluding that the difference between the two groups was due to rapid application of wound site administration in contrary to USG guided TAP block, which was more time consuming.
McDonnell et al7 compared a placebo with TAP block and reported that TAP block provided superior analgesia until 48 hours. In addition, it has been reported that TAP block not only reduced postoperative opioid need but also extended first analgesia application time8. We did not use a control group, as both TAP block and infiltration anaesthesia had already proved their superiority over placebo. Our study is the first study to compare TAP block with infiltration anaesthesia after spinal anaesthesia in deliveries with caesarean section, and our primary goal was to compare patient pain scores and patient satisfaction. In our study, no analgesic was administered to seven patients in Group T and five patients in Group I in the first 24 hours. However, the first analgesia administration time was longer in Group T than in Group I. In both groups, anti-inflammatory medicine administration was sufficient. No opioid was needed for any patients.
Belavy et al9 demonstrated that morphine consumption is lower when USG-guided TAP block is used as a companent of a multimodal regimen after spinal anaesthesia. In their retrospective study on patients with or without TAP after caesarean section, Patel et al10 found that oral narcotic tablet use was low, 24-48 hours postoperatively, in the TAP group. In some newly conducted studies, it has been reported that total morphine need is lower in TAP patient groups and that side effects, such as sedation related to opioid use, postoperative nausea, and vomiting, are also low and that patient satisfaction is beter4,8. Scharine11 reported that a long and effective analgesia is obtained by TAP block, and that lower pain score, earlier oral nutrition, and earlier mobilization are seen, and duration of hospital stay is shortened, as when no narcotic analgesic is used. In their study, Tan et al12 applied USG-guided TAP block after general anaesthesia in caesarean section operations, and they found that morphine need is lowered and mother satisfaction is increased. In our study, there were no differences between groups in terms of patient satisfaction. We believe the reason for this result is that both methods we used provide more effective analgesia than placebo.
Ganta et al13 compared patients to whom they applied wound site infiltration and ilioinguinal block after caesarean section with a control group, and they did not find a statistically significant difference. In a study similar to our study, on/under skin local anesthetic administration and USG–guided TAP blocks in total hysterectomy patients were compared with a control group. Pain scores of the group with TAP block were found to be lower than those of the infiltration group in the 6 and 24th hours, and it was reported that TAP block was more effective than surface wound site infiltration in postoperative pain management14. In our study on caesarean section patients, the pain scores in the TAP block group were lower at 2, 6, 12 and 24 hours postoperatively. However, there were no differences in pain scores during their first mobilization.
Conclusion
According to our results, USG-guided TAP block could be considered. superior to infiltration anaesthesia for the postoperative pain management of patients who have had caesarean section under spinal anaesthesia, and it provides longer-lasting and more efficient analgesia than infiltration anaesthesia.
Conflicts of interest
None of the authors have any conflicts of interest to declare.
Acknowledgement
The study has been reported in abstract form in the TARK, 2012, Cyprus.
References
- 1.Baaj JM, Alsatli RA, Majaj HA, Babay ZA, Thallaj AK. Efficacy of ultrasound-guided transversus abdominis plane (TAP) block for postcesarean section delivery analgesia--a double-blind, placebo-controlled, randomized study. Middle East J Anesthesiol. 2010;20:821–826. [PubMed] [Google Scholar]
- 2.Bensghir M, Elwali A, Miller C, Azendour H, Drissi M, Bakkali H, et al. [Effects of skin infiltration with ropivacaine 0,75% on postoperative pain after caesarean section] Gynecol Obstet Fertil. 2008;36:516–520. doi: 10.1016/j.gyobfe.2008.03.007. [DOI] [PubMed] [Google Scholar]
- 3.Bamigboye AA, Hofmeyr GJ. Caesarean section wound infiltration with local anaesthesia for postoperative pain relief - any benefit? S Afr Med J. 2010;100:313–319. doi: 10.7196/samj.3716. [DOI] [PubMed] [Google Scholar]
- 4.Petersen PL, Mathiesen O, Torup H, Dahl JB. The transversus abdominis plane block: a valuable option for postoperative analgesia? A topical review. Acta Anaesthesiol Scand. 2010;54:529–535. doi: 10.1111/j.1399-6576.2010.02215.x. [DOI] [PubMed] [Google Scholar]
- 5.Abdallah FW, Halpern SH, Margarido CB. Transversus abdominis plane block for postoperative analgesia after Caesarean delivery performed under spinal anaesthesia? A systematic review and meta-analysis. Br J Anaesth. 2012;109:679–687. doi: 10.1093/bja/aes279. [DOI] [PubMed] [Google Scholar]
- 6.Ducarme G, Sillou S, Wernet A, Davitian C, Poujade O, Ceccaldi PF, et al. [Single-shot ropivacaine wound infiltration during cesarean section for postoperative pain relief] Gynecol Obstet Fertil. 2012;40:10–13. doi: 10.1016/j.gyobfe.2011.07.035. [DOI] [PubMed] [Google Scholar]
- 7.McDonnell JG, Curley G, Carney J, Benton A, Costello J, Maharaj CH, et al. The analgesic efficacy of transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg. 2008;106:186–191. doi: 10.1213/01.ane.0000290294.64090.f3. [DOI] [PubMed] [Google Scholar]
- 8.Siddiqui MR, Sajid MS, Uncles DR, Cheek L, Baig MK. A meta-analysis on the clinical effectiveness of transversus abdominis plane block. J Clin Anesth. 2011;23:7–14. doi: 10.1016/j.jclinane.2010.05.008. [DOI] [PubMed] [Google Scholar]
- 9.Belavy D, Cowlishaw PJ, Howes M, Phillips F. Ultrasound-guided transversus abdominis plane block for analgesia after Caesarean delivery. Br J Anaesth. 2009;103:726–730. doi: 10.1093/bja/aep235. [DOI] [PubMed] [Google Scholar]
- 10.Patel SA, Gotkin J, Huang R, Darling C, Pates JA, Dolinsky B. Transversus abdominis plane block for postoperative analgesia after cesarean delivery. J Matern Fetal Neonatal Med. 2012;25:2270–2273. doi: 10.3109/14767058.2012.685789. [DOI] [PubMed] [Google Scholar]
- 11.Scharine JD. Bilateral transversus abdominis plane nerve blocks for analgesia following cesarean delivery: report of 2 cases. AANA J. 2009;77:98–102. [PubMed] [Google Scholar]
- 12.Tan TT, Teoh WH, Woo DC, Ocampo CE, Shah MK, Sia AT. A randomised trial of the analgesic efficacy of ultrasound-guided transversus abdominis plane block after caesarean delivery under general anaesthesia. Eur J Anaesthesiol. 2012;29:88–94. doi: 10.1097/EJA.0b013e32834f015f. [DOI] [PubMed] [Google Scholar]
- 13.Ganta R, Samra SK, Maddineni VR, Furness G. Comparison of the effectiveness of bilateral ilioinguinal nerve block and wound infiltration for postoperative analgesia after caesarean section. Br J Anaesth. 1994;72:229–230. doi: 10.1093/bja/72.2.229. [DOI] [PubMed] [Google Scholar]
- 14.Atim A, Bilgin F, Kilickaya O, Purtuloglu T, Alanbay I, Orhan ME, et al. The efficacy of ultrasound-guided transversus abdominis plane block in patients undergoing hysterectomy. Anaesth Intensive Care. 2011;39:630–634. doi: 10.1177/0310057X1103900415. [DOI] [PubMed] [Google Scholar]