

Sir,
Pseudo-Kaposi's sarcoma is considered an acquired benign reactive vascular proliferation that clinically resembles Kaposi's sarcoma.[1] It can appear in various vascular conditions such as Stewart-Bluefarb syndrome[2] and chronic venous insufficiency of the lower extremities called acroangiodermatitis of Mali,[3] and limb anomalies. There are reported cases of pseudo-Kaposi's sarcoma of the hand associated with acquired iatrogenic arteriovenous fistula for hemodialysis.[4] This study reports the case of pseudo-Kaposi's sarcoma of the hand that healed after changing the position of the AV-shunt for hemodialysis.
A 66-year-old man was first evaluated for diabetes at the age of 56 in 1998. End-stage renal disease probably secondary to diabetes developed in 2000. Subsequently, hemodialysis was required, which led to creation of an AV-shunt (side-to-side radial artery-to-cephalic vein anastomosis) on his left wrist in 2003.
In 2009, edematous, crusted, violaceous, and pigmented plaques developed on his left fourth and fifth fingers [Figure 1a] associated with slight intermittent pain. Further examination revealed a pulsatile, non tender, aneurismal dilation of the AV-shunt on the radial aspect of the left distal forearm [Figure 1b black arrow)]. A skin biopsy specimen from the dorsum of the fourth finger showed hyperkeratosis, irregular acanthosis, prominent proliferation of small dilated vessels in the upper and mid dermis, and extravasated erythrocytes [Figure 1c] without vascular slits and atypical endothelial cells. Immunohistochemical analysis showed CD34-positive endothelial cells, but CD34-negative perivascular cells [Figure 1d]. Some vessels had CD31-positive [Figure 1e] and D2-40-positive cells [Figure 1f]. Four months later, the initial AV-shunt was obstructed, and a new AV-shunt was created around the proximal part of the wrist about 10 cm away from the initial site [Figure 1g (white arrow)]. After 1 year, edema and crusts on the fingers disappeared [Figure 1h]. Three years later, discoloration on the fingers completely improved [Figure 1j].
Figure 1.
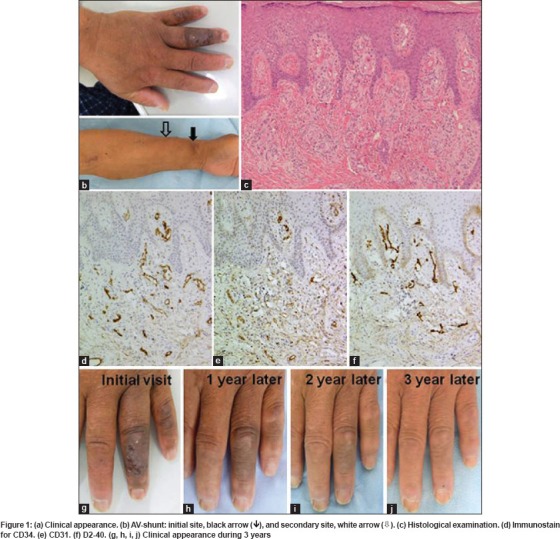
In most cases of pseudo-Kaposi's sarcoma, surgical intervention is not feasible, because the congenital malformation variety consists of multiple small distal lesions. Compression stockings as supportive measures may limit venous stasis and local wound care for ulcers. Various medical treatments, e.g. oral erythromycin,[4] have been tried with favorable results but options are limited. In our case, the resolution was probably due to the obstruction of the initial AV-shunt. The new AV-shunt did not cause recurrence of the lesions. Changing the site of the AV-shunt may be optional.
Immunohistochemical staining with CD34 has been performed in sections of pseudo-Kaposi's sarcoma to distinguish between pseudo-Kaposi's sarcoma and Kaposi's sarcoma because only plump endothelial cells are positive in the former, while perivascular and endothelial cells are positive in the latter.[5] In our study, in addition to CD34 staining, immunohistochemical staining with CD31 and D2-40 demonstrated vessels with D2-40-positive and CD31-positive cells. To our knowledge, there are no reports about immunohistochemical analysis using the specific antibody for lymphatic vessels in pseudo-Kaposi's sarcoma. This study indicates that pseudo-Kaposi's sarcoma could be the cutaneous-reactive lymphangiomatosis induced by vascular abnormality and lymphedema.
References
- 1.George M, Carr RA, Gee BC. Acroangiodermatitis of Mali. Clin Exp Dermatol. 2010;35:94–6. doi: 10.1111/j.1365-2230.2009.03730.x. [DOI] [PubMed] [Google Scholar]
- 2.Agrawal S, Rizal A, Agrawal CS, Anshu A. Pseudo-Kaposi's sarcoma (Bluefarb-Stewart type) Int J Dermatol. 2005;44:136–8. doi: 10.1111/j.1365-4632.2004.02481.x. [DOI] [PubMed] [Google Scholar]
- 3.Zutt M, Emmert S, Moussa I, Haas E, Mitteldorf C, Bertsch HP, et al. Acroangiodermatitis Mali resulting from arteriovenous malformation: Report of a case of Stewart-Bluefarb syndrome. Clin Exp Dermatol. 2008;33:22–5. doi: 10.1111/j.1365-2230.2007.02541.x. [DOI] [PubMed] [Google Scholar]
- 4.Goldblum OM, Kraus E, Bronner AK. Pseudo-Kaposi's sarcoma of the hand associated with an acquired, iatrogenic arteriovenous fistula. Arch Dermatol. 1985;121:1038–40. [PubMed] [Google Scholar]
- 5.Kanitakis J, Narvaez D, Claudy A. Expression of the CD34 antigen distinguishes Kaposi's sarcoma from pseudo-Kaposi's sarcoma (acroangiodermatitis) Br J Dermatol. 1996;134:44–6. [PubMed] [Google Scholar]