

Abstract
Background and Purpose
Allogeneic hematopoietic stem cell transplantation (HSCT) is the only curative treatment for sickle cell anemia (SCA). We report our experience with transplantation in children with the Black African variant of SCA and the effects of transplant on erythroid compartment in bone marrow (BM).
Patients and methods
Twenty-seven consecutive patients who underwent BM transplantation from HLA-identical donors following a myeloablative conditioning regimen were included. Using both CD71 and FSC parameters, we obtained three erythroid populations: EryA–C. Ery A (CD71high FSChigh) are basophilic; Ery B (CD71high FSClow) are late basophilic and polychromatic; and Ery C (CD71low FSClow) are orthochromatic erythroblasts and reticulocytes. To analyze the effect of transplantation on intramedullary apoptosis, we studied Fas (CD95+) and caspase-3 expression in erythroblast subpopulations.
Results
All patients experienced sustained engraftment, and all surviving patients remained free of SCA-related events after transplantation. The erythroid population showed expansion in the BM at baseline. After transplant, levels decreased, especially of Ery C, in parallel to reduced Fas expression and an initial caspase 3 increase in erythroid population, similar to reported later steps of “normal” erythroid maturation.
Conclusions
The results suggest a good chance of cure for children with SCA, with an excellent survival rate. We also observed “normalization” of erythroid populations in parallel with a decreased intramedullary apoptosis rate, suggesting normal erythroid maturation in ex-SCA patients after HSCT.
Introduction
Sickle cell disease is a group of genetic conditions in which pathology results from the inheritance of the sickle cell gene variant either homozygously or as a double heterozygote with another interacting gene. The spectrum of resulting conditions is influenced by the geography of individual hemoglobin genes, but in most populations, the commonest genotype at birth is homozygous sickle cell (SS) disease. Since this genotype involves a greater mortality, the relative proportion of sickle cell genotypes is influenced by age as well as by the geographical distribution of individual genes.1
The sickle cell trait is widespread throughout Africa. Frequencies are low (<1%–2%) in the north and south of the continent but high with variable frequencies throughout much of equatorial Africa. SCA is characterized by a cascade of events that begin with the polymerization of hemoglobin S and the sickling of red blood cells. Following these events is occlusion of small and larger vessels because of the adherence of the sickled cells to the vascular endothelium, which leads to pain crises, stroke, acute chest syndrome, and multi-organ failure as the most frequent complications.2 In patients with the Black African variant, painful crises, chest syndrome, and stroke are more frequent and appear earlier in life. The causes of death are strongly influenced by the prevalence of malaria and other infections, and almost certainly by the availability and sophistication of medical and other services. In sub-Saharan Africa, survival is markedly shortened, and median survival may be as short as 5 years.
Hematopoietic stem cell transplantation (HSCT) is the only radical cure for this genetic disorder,3 and to date, several hundred patients have undergone gene-identical HSCT.4–9 In accordance with data recently published,25 our experiences confirm that it is possible to offer a good chance of cure to children with SCA, and we thus have made the following recommendation: “HSCT should be considered the standard of care for SCA children with a human leukocyte antigen-identical donor, before complications result from the sickling of red blood cells.”
Less well established is the potential contribution of ineffective erythropoiesis to the pathophysiology of this hemoglobinopathy. As in thalassemia patients, an expansion of erythroid precursors is observed in SCA patients at the bone marrow (BM) level but is less severe than in thalassemia.10–11 Normal homeostasis of the erythropoietic system requires an appropriate balance between the rate of erythroid cell production and red blood cell destruction. Growing evidence indicates that apoptotic mechanisms play a relevant role in the control of erythropoiesis under physiologic and pathologic conditions.10 Death receptors of the TNF receptor superfamilies (Fas-Ligand (Fas-L), TNF-α, TRAIL) activate the extrinsic apoptotic pathway. Fas and Fas-L are expressed in cultured erythroblasts, but there are controversies regarding the level and differentiation stage at which they are expressed. Some studies suggest the existence of a negative regulatory feedback operating at low erythropoietin (Epo) levels in a paracrine pathway. In this system, Fas-L–expressing mature erythroblasts display cytotoxicity against immature erythroblasts expressing Fas.12,13 Epo can partially protect immature erythroid cells from Fas-mediated apoptosis; thus, Fas and Fas-L are major regulators of erythropoiesis.
Both proteins are downregulated in BM or spleen in proerythroblast and basophilic cells in β-thalassemic mice compared to control mice in vivo. This downregulation of Fas/Fas-L expression might be a marker of erythropoietic stress and explain, at least in part, erythroid expansion in thalassemia.14
We hypothesized that Fas might contribute to the cell death of SS erythroid precursors at the BM level, but that transplant may be corrective. Here we report our experience with transplantation in a group of pediatric patients with Black African variant SCA, who received transplantations from HLA-identical siblings. We analyzed the effect of transplant on erythropoiesis and intramedullary apoptosis, studying Fas (CD95+) and caspase-3 expression in erythroblast subpopulations before and after transplant. We also used this opportunity to directly compare the differentiation and survival of SCA and donor (AA or AS trait carrier)-derived erythropoiesis in vivo.
Patients and Methods
This study included 27 consecutive SCA patients who underwent BM transplantation from HLA-identical sibling donors between January 2010 and June 2013. Twenty-seven patients with the Black African SCA variant were treated with a modification of our Protocol 26, which was in use for Class 3 thalassemia patients15 (here identified as Protocol 28). The institutional review board approved the treatment protocol, and all parents of patients provided written informed consent in accordance with the Declaration of Helsinki.
Patient characteristics
The median patient age was 10 years (range 2–17 years), and the median donor age was 11 years (range 1–26 years). Patient characteristics at the time of transplantation are summarized in Table 1. All patients showed good performance status (Lansky/Karnofsky 100) before transplantation. No patient had a splenectomy before transplantation, and only two received chronic blood transfusions; the serum ferritin level before transplantation was 278 ± 231 ng/mL (mean ± SD). Before transplantation, 11 patients had recurrent, painful, vaso-occlusive crisis; nine patients had recurrent painful crisis in association with acute chest syndrome; three patients experienced ischemic stroke and recurrent vaso-occlusive crisis; two patients experienced ischemic stroke; one patient exhibited leukocytosis, and one patient exhibited priapism.
Table 1.
Characteristics of patients (all Nigerian) harboring the Black African variant of SCA
| UPN. | Age/Sex | HbS (%) | HbF (%) | Donor HbS (%) | Frequent VOC | Acute chest syndrome | Arterial ischemic stroke | No. Tx |
|---|---|---|---|---|---|---|---|---|
| 166 | 14/M | 76 | 22 | 30 | yes | yes | Yes | 14 |
| 191 | 6/F | 70 | 27 | 41 | yes | yes | No | 0 |
| 192 | 9F | 75 | 28 | 37 | yes | yes | No | 0 |
| 195 | 11/F | 71 | 27 | 0 | yes | yes | Yes | 3 |
| 199 | 15/F | 86 | 10 | 36 | yes | yes | no | 3 |
| 201 | 17/M | 89 | 7 | 0 | yes | no | no | 0 |
| 202 | 3/M | 85 | 11 | 35 | yes | no | no | 1 |
| 204 | 12/M | 92 | 3 | 0 | yes | no | no | 0 |
| 205 | 5/M | 79 | 17 | 0 | yes | no | no | 0 |
| 206 | 7/F | 83 | 14 | 0 | yes | no | no | 0 |
| 207 | 13/M | 88 | 8 | 41 | yes | yes | no | 3 |
| 210 | 3/M | 73 | 24 | 37 | yes | no | yes | 0 |
| 213 | 16/M | 91 | 5 | 0 | yes | no | no | 0 |
| 215 | 2/M | 87 | 10 | 40 | no | no | no | 0 |
| 216 | 14/F | 92 | 4 | 0 | yes | yes | no | 2 |
| 219 | 15/M | 91 | 5 | 28 | yes | no | no | 15 |
| 221 | 4/F | 83 | 15 | 31 | yes | yes | no | 0 |
| 222 | 16/M | 91 | 5 | 0 | yes | no | no | 1 |
| 224 | 5/F | 61 | 3 | 35.8 | yes | yes | no | 0 |
| 229 | 17/M | 82 | 14 | 0 | yes | yes | no | 2 |
| 231 | 5/M | 88 | 7.4 | 37 | no | no | yes | 0 |
| 234 | 15/F | 94 | 1.9 | 42.1 | yes | yes | no | 2 |
| 235 | 8/F | 77 | na | 0 | no | no | yes | 2 |
| 236 | 17/M | 63 | 9.8 | 0 | no | no | no | 2 |
| 237 | 10/F | 85 | 12.3 | 41.3 | yes | no | no | 0 |
| 239 | 13/F | 73 | 3.7 | 39.4 | yes | no | no | 1 |
| 240 | 12/F | 80 | 16.9 | 42.5 | yes | no | no | 1 |
HbS, hemoglobin S; HbF, hemoglobin F; VOC, vaso-occlusive crisis; No. Tx, number of red blood cell transfusions received before transplant; na, not available.
HLA typing at the molecular level was performed, and all donors for both groups were fully matched.
Transplantation procedure
Patients received fludarabine (30 mg/m2/day) for 5 days and a conditioning regimen including targeted intravenous busulfan (14 mg/kg total dose) and cyclophosphamide (200 mg/kg total dose). All patients received cyclosporine A, low-dose methylprednisolone, and a short course of methotrexate as GVHD prophylaxis. Among the patients, six had cyclosporine A-related neurotoxicity with seizures. All patients received valproic acid (Depakin; Sanofi-Aventis) at a dose of 30 mg/kg/day in 3 divided doses starting at 24 hours before the first busulfan administration. Many risk factors for the development of CSA-related neurotoxicity have been investigated in our patients, including arterial hypertension, fluid overload, hypercholesterolemia, hypomagnesaemia and pre-existing brain disease. In the screening examinations of these patients the brain magnetic resonance imaging (MRI) showed gliosis in 11/27 stroke free Black African SCA patients (manuscript in preparation). The brain MRI finding, usually associated to CSA neurotoxicity, was posterior reversible leukoencephalopathy syndrome (PRES), typically distributed in the posterior regions of the white matter of the brain. We cannot rule out the pre-existing brain disease in these patients might predispose to seizures during CSA treatment. In general, the prognosis of CSA neurotoxicity has been good and posterior leukoencephalopathy usually resolved completely with dose reduction or drug withdrawal. As alternative GVHD prophylaxis, we opted for tacrolimus. This calcineurin inhibitor, although similar to CSA in mechanism and metabolism, did not produce neurological side effects in these patients.
Children with Black African variant SCA were prone to invasive infections caused by S. pneumonia, H. influenzae and Plasmodium falciparum (in malarial areas). Malaria is more endemic in Black African areas and therefore malaria is more common in Black SCA patients. In Africa, malaria contributes substantially to the early mortality of patients with SCA. For these reasons we preferred in this population fludarabine-based preparative protocols, well tolerated, with less immunosuppression and minimal toxicity.
All patients received BM from HLA-identical sibling donors 36 h after the final dose of cyclophosphamide, and all donors with sickle cell trait received hyperhydration and blood transfusion before the multiple marrow aspirations. The median number of total nucleated cells infused was 4.08 × 108/kg (range 1.7 × 108/kg to 10.0 × 108/kg), and the median number of CD34 cells was 5.8 × 108/kg (range 1.2 × 106/kg to 11.2 × 106/kg).
The diagnosis and degree of acute and chronic GVHD were assessed according to standard criteria.16,17 All patients were given prophylactic broad-spectrum antibiotics and antifungal drugs until the neutrophil level exceeded 1.0 × 109/L, and also received acyclovir as herpes virus prophylaxis and trimethoprim/sulfamethoxazole as Pneumocystis jiroveci prophylaxis. Patients were monitored weekly for the presence of Epstein-Barr virus, cytomegalovirus (CMV), adenovirus, and BK virus in the blood and/or urine using sensitive reverse transcriptase polymerase chain reaction (PCR), from the beginning of transplant preparation until at least 100 days post-transplant.
Assessment of chimerism
The first chimerism analysis was performed on BM samples obtained 20 days after transplant to determine the percentage of donor/recipient DNA using PCR-based analysis of short tandem repeats. Subsequently, at 60, 90, 180, and 365 days post-transplant, lineage-specific chimerism analysis was performed by PCR using fluorescent primers flanking a single informative short tandem repeat (AmpFLSTR Profiler Plus; Applera, CA, USA) previously identified to be polymorphic between the patient and donor.
Cytometric assay for erythroid cell precursors
We previously developed a flow cytometric assay to identify stage-specific erythroblasts directly in hematopoietic tissue (BM) based on their expression of the transferrin receptor (CD71), which declines with erythroblast maturation.18 However, the decline in CD71 appeared to be gradual, without the formation of well-resolved subpopulations. In this study, we distinguished well-resolved erythroblast subpopulations by considering, in addition to CD71, the forward scatter (FSC) parameter. FSC is a function of cell size and has been used previously to assess erythroblast maturation independently of cell surface marker expression. When the cells were analyzed using both CD71 and FSC parameters, they consistently resolved into three principal subpopulations, which we labeled Ery A, Ery B, and Ery C erythroblasts. Ery A (CD71high FSChigh) are basophilic; Ery B (CD71high FSClow) are late basophilic and polychromatic; and Ery C (CD71low FSClow) are orthochromatic erythroblasts and reticulocytes.11,14
Bone marrow specimens of patients and donors were obtained to evaluate Fas and caspase 3 expression in erythroblasts: anti-CD95 PE, anti-CD71 FITC, and anti-CD45 PercP Cy5.5 were mixed in a tube. A volume of 10 μL of these MoAb cocktails (BD, Becton Dickinson, San Diego, CA, USA) was combined with 100 μL of bone marrow mononuclear cells for 10 minutes at room temperature, then lysed with BD Pharm Lyse 1× for 20 minutes at room temperature and washed with 2% phosphate-buffered saline plus bovine serum albumin. Samples were analyzed with BD FACS Canto II and the software, BD FACSDiva.
Statistical analysis
The probabilities of survival, SCA-free survival, rejection, and mortality were calculated using Kaplan–Meier curves.19
Non-parametric statistics was used (Mann-Whitney, Wilcoxon test) for unpaired and paired comparisons between the parameters analysed in patients and healthy individuals. A p-value less than 0.05 was considered significant. Statistical analyses were performed by using Stat View 5.0 software (SAS Institute, Cary, NC, USA).
Results
Clinical assessment post-transplant
The median time to neutrophil recovery (absolute neutrophil count ≥ 500 × 109/L on 3 consecutive days) was 16 days (range 11– 23 days). Platelet recovery ≥20 ×109/L was observed at a median of 17 days (range, 11–22 days) after allo-HSCT. In terms of platelet transfusion needs, the median number of platelet units transfused in the first 100 days after HSCT was 15 U (range, 0–53 U) but it increased when complications as severe acute GVHD or sepsis appeared. In our cohort of patients we observed a lower rate of platelet transfusion and faster platelet recovery kinetics after HSCT, but also highlighted the negative effect of severe acute GVHD as a risk factor for increased need for platelet transfusions.
At 2 months after transplantation 3 patients had donor chimerism between 95% and 98%, and all the remaining patients had full donor chimerism. At the last control, all patients experienced sustained engraftment with 100% donor chimerism. All patients and donors except one had positive serology for CMV before transplantation. Asymptomatic CMV reactivation occurred in 26 of 27 patients. All patients were provided pre-emptive antiviral therapy, and none developed CMV disease.
Seven patients developed grade 2 acute GVHD of the skin, and five patients developed grade 3–4 GVHD, principally after 30 days post transplant. All patients responded promptly to the steroid treatment administered to control acute GVHD (1–2 mg/kg/day prednisone). At present, all patients except one are off immunosuppressive medication. Chronic GVHD was observed in four patient: one patient developed bronchiolitis obliterans, and one patient had severe chronic GVHD with intestinal and hepatic involvement until death, as a result of multi-organ failure at day +190 post-transplantation. Cumulative incidence of grade 3–4 acute GVHD was 18%. Cumulative incidence of persistent severe chronic GVHD was 14%.
One patient died at 77 days post-transplantation from complications of severe GVHD of the gut. One patients died from multiorgan failure at 190 days post-transplantation. He had no steroid responsive grade 4 acute GVHD of the gut and developed sepsis, which led to multiorgan failure and death. One patient died from complications of bronchiolitis obliterans at 445 days post-transplantation.
After transplantation, no patients experienced complications typical of SCA, such as pain, stroke, or acute chest syndrome. The probabilities of survival, SCA-free survival, and transplant-related mortality after transplant were 89%, 89%, and 11%, respectively.
Expression of Fas and caspase-3 on erythroid population at the BM level
We observed an expansion of the BM erythroid population at baseline, probably as an essential process needed to maintain a constant red cell production in SCA patients (Fig. 1). Average percentages of CD71+CD45− were 4.6 ± 3.7% in normal AA donors, 7 ± 2.8% in AS trait carrier donors, 18.7 ± 14.6% in SCA patients at baseline, and 8.1 ± 5.6% in SCA patients at 60 days after transplant. After HSCT, decreased levels were observed in all three erythroid subpopulations (average 40 ± 20% vs. 45.3 ± 16.7% at baseline for Ery A; 38.4 ± 20.5% vs. 46.2 ± 16.4% at baseline for Ery B), especially for Ery C (2 ± 5% vs. 13.2 ± 25.4% at baseline; p= 0.0028) (Fig. 2) in parallel to a reduction in Fas expression (Fig. 3) in the BM (average CD95+CD34+, 3.7 ± 1.7% in normal AA donors; 4.9 ± 3.3% in AS trait carrier donors; 9.6 ± 7.3% in SCA patients at baseline, p= 0.004 vs. healthy controls; and 7.3 ± 4% at 60 days after transplant, p= 0.007 vs. healthy controls) and specifically in the erythroid compartment (average CD95+CD71+CD45−, 1.6 ± 1.9% in normal AA donors; 1.8 ± 3.2% in AS trait carrier donors; 2.9 ± 2.9% in SCA patients at baseline; and 2 ± 2.7% at 60 days after transplant) (Fig. 3). After transplant, a tendency to a normalization of erythropoiesis has been observed in our patients, with a reduction of Fas expression on three erythroid population but especially on more mature erythroid precursors Ery C (Fig. 4).
Figure 1.

Flow cytometric analysis of bone marrow cells. (A, B) Bone marrow cells labelled with antibodies against CD71 and CD45. (A) Plot of CD71+CD45− versus FCS in SCA patients at baseline. (B) Plot of CD71+CD45− versus FCS in SCA patients at 60 days post-transplant (TMO). (C) Comparison of the percentages of erythroid precursors (CD71+CD45−) at the bone marrow level in normal donors (white bar), in AS trait carrier donors (dashed bar), in SCA patients at baseline (gray bar), and after 60 days post-transplant (black bar). The results are expressed as mean ± SD.
Figure 2.

Flow cytometric analysis of erythroid subpopulations at the bone marrow level. (A, B) Primary bone marrow cells were simultaneously stained with CD71+CD45−. We distinguished erythroblast subpopulations (Ery A, Ery B, and Ery C) by considering, in addition to CD71, the forward scatter (FSC) parameter in the gated erythroid population. Ery A is CD71high FSChigh, Ery B is CD71high FSClow, and Ery C is CD71low FSClow. (A) Erythroid subpopulation in SCA patients at baseline. (B) Erythroid subpopulation in SCA patients 60 days post-transplant. (C–E) Comparison of percentages of Ery A, Ery B, and Ery C in SCA patients at baseline (gray bar), in SCA patients 60 days post-transplant (black bar) vs. normal donors (white bar) and AS trait carrier donors (dashed bar). The results are expressed as mean ± SD; * p= 0.0028.
Figure 3.
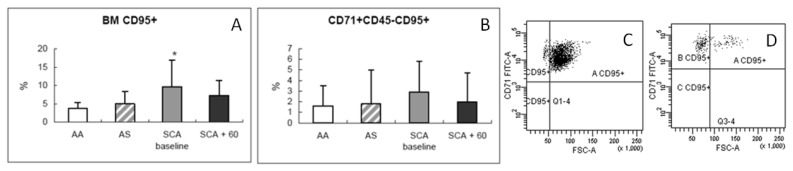
(A, B) Comparison of percentages (mean ± SD) of Fas expression at the bone marrow level (BM CD95+) and on erythroid populations (CD95+CD71+45−) in normal donors (white bar), in AS trait carrier donors (dashed bar), in SCA patients at baseline (gray bar), and after 60 days post-transplant (black bar). (C, D) Flow cytometric analysis of erythroid subpopulations (Ery A, Ery B, and Ery C) for CD95+ expression in SCA patients at baseline (C) and after 60 days post-transplant (D); * p= 0.004.
Figure 4.

(A, B, C) Comparison of percentages (mean ± SD) of Fas expression on erythroid subpopulations (A: Fas expression on Ery A; B: Fas expression on Ery B; C: Fas expression on Ery C) in SCA patients at baseline (gray bar), and after 60 days post-transplant (black bar).
An initial increase in caspase 3 was observed after HSCT, as has been reported for later steps of “normal” erythroid cell maturation. Average percentages of caspase 3+CD71+CD45− were 1.8 ± 1.8% in normal AA donors, 2.7 ± 2.2% in AS trait carriers donors, 2 ± 1.5% in SCA patients at baseline, and 3.7 ± 4.3% in SCA patients at 60 days after transplant (Fig. 5).
Figure 5.

(A) Comparison of the percentages (mean ± SD) of erythroid precursors expressing caspase 3 (casp. 3+CD71+CD45−) at the bone marrow level in normal donors (white bar), in AS trait carrier donors (dashed bar), in SCA patients at baseline (gray bar), and after 60 days post-transplant (black bar). (B, C) Flow cytometric analysis of erythroid compartment for caspase 3 expression in SCA patients at baseline (B) and after 60 days post-transplant (C).
Discussion
The morbidity and mortality associated with SCA are much more frequent and severe than those associated with thalassemia. The Black African SCA variant manifests a severe phenotype when compared to the non-Black African SCA. It is possible that in patients with Black African SCA, a hyperplasia of the erythroid lineage exists at baseline, probably to maintain a constant production of erythroid precursors. The high level of polymerization of the sickle hemoglobin in host RBCs, as well as in host early and basophilic normoblasts, might also determine mechanical defects that, in turn, increase host cell susceptibility to clearance and loss.
The presence of ineffective erythropoiesis in SCA is supported by previous studies, which have identified structural abnormalities in SS erythroid precursor cells, thus indirectly indicating the increased susceptibility of these cells to clearance and loss. Blouin et al. examined erythropoiesis in the SCA mouse model and found significant morphological alteration in erythroid lineage late precursors (polychromatophilic normoblasts) within the marrow.20 These morphological studies identified a high level of hemoglobin polymers that were associated with increased cell fragmentation occurring during medullary transendothelial migration of reticulocytes. Older ultrastructural studies of BM aspirates derived from SCA patients identified reticulocytes that contain bundles of hemoglobin S polymers in the absence of intentional deoxygenation, as well as sickling of nucleated erythroblasts and extensive marrow erythrophagocytosis.21,22
Hasegawa et al. also found in an in vitro system that cultured nucleated erythroid precursors can undergo sickling under deoxygenating conditions 23. Recently, our group observed the presence of sickled erythrocytes at the BM level in SCA patients, in the absence of systemic symptoms, as well in AS trait carriers. This condition could be induced by the cellular stress of the biopsy procedure or alternatively represents a specific status of the BM of SCA patients, both the homozygous (SS) and heterozygous (AS) status (manuscript in preparation).
Apoptosis is an important mechanism by which ineffective erythroblasts are cleared within the intramedullary space, and our data suggest that Fas might contribute to the cell death of host erythroid precursors in SCA. If accelerated apoptosis is not compensated by enhanced erythropoiesis, however, clinically relevant anemia develops. Our studies suggest that significant abnormalities in SS erythroid precursors exist within the intramedullary space and that cells prone to sickling may be selectively destroyed prior to release from the erythropoietic compartment.
With HSCT, it is possible to give more than 90% chance of cure for children with SCA, with excellent survival rate and return to normal life. We agree with the recommendations of the Haematologica’ s authors.25 The young patients with symptomatic SCA, who have an HLA-matched sibling donor, should be transplanted as early as possible before sickling complications appear. The vast majority of our patients are not regularly transfused/chelated, or highly sensitized due to receiving RBC transfusions without the use of leukodepletion filters. Despite the recognized benefits of transfusion therapy, it is not without the risks of iron overload, alloimmunization, and delayed hemolytic transfusion reactions. Alloimmunization to RBC antigens is a major complication associated with RBC transfusions in patients with SCA. Alloantibodies and autoantibodies complicate RBC cross-matching, delay provision of transfusions, and increase the labor and cost of providing compatible RBC units. For these reasons and since patients had an HLA-identical sibling donor, these patients had indications for hematopoietic stem cell transplant.
After HSCT, we observed a “normalization” of erythroid populations, in parallel with a decreased intramedullary apoptosis rate, suggesting normal erythroid maturation in ex-SCA patients. In fact in the basal state, the erythropoietic system continuously produces excess numbers of early erythroblast, which become apoptotic through Fas-mediated signaling. The principal advantage of a homeostatic mechanism that relies on negative autoregulation of cell numbers is that it would self-correct for small perturbations, maintaining a relatively constant erythroblast population size in the basal state. The major expression of Fas at the early stage of erythroblast maturation has been observed at baseline in our patients, contributing to a negative autoregulation of cell number. After transplant, a tendency to a normalization of erythropoiesis has been observed in our patients, with a reduction of Fas expression on three erythroid population but especially on more mature erythroid precursors Ery C. A progressive maturation advantage for homozygous hemoglobin A (AA) or heterozygous hemoglobin S/hemoglobin A (SA) donor erythroid precursor cells resulted in a greater donor contribution to overall erythropoiesis following stem cell transplantation and improvement of clinical manifestations.
Conclusions
This study suggests a good chance of cure for children with SCA, with HLA-identical transplant. We also observed “normalization” of erythroid populations in parallel with a decreased intramedullary apoptosis rate, suggesting normal erythroid maturation in ex-SCA patients after HSCT. HSCT should be considered the standard of care for SCA children with human leukocyte antigen-identical donor before complications result from the sickling of red blood cells.
Footnotes
Competing interests: The authors have declared that no competing interests exist.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Author Contributions. A. I. designed the research, analyzed data, and wrote the paper. P. S., M. M., J. G., K. P., C. G., G. D., C. A., M. R., D. A. and A. R. followed the clinical aspects of the patients. D. F. performed cytofluorimetric analyses. M. A. and M. T. performed HLA typing and the assessment of chimerism. G. L. supervised the research and contributed to the writing of the paper. All authors approved the final manuscript.
References
- 1.Serejeant GR. The natural history of Sickle cell disease. Cold Spring Harbor Perspectives in Medicine. 2013;3:1–11. doi: 10.1101/cshperspect.a011783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Roseff SD. Sickle cell disease: a review. Immunohematology. 2009;25:67–74. [PubMed] [Google Scholar]
- 3.Lucarelli G, Gaziev J, Isgrò A, Sodani P, Paciaroni K, Alfieri C, De Angelis G, Marziali M, Simone MD, Gallucci C, Roveda A, Saltarelli F, Torelli F, Andreani M. Allogeneic cellular gene therapy in hemoglobinopathies: evaluation of hematopoietic stem cell transplantation in Sickle Cell Anemia. Bone Marrow Transplantation. 2012;47(2):227–30. doi: 10.1038/bmt.2011.79. [DOI] [PubMed] [Google Scholar]
- 4.
- 5.Giardini C. Bone marrow transplantation in sickle cell disorders in Pesaro. Bone Marrow Transplantation. 1997;19:106–9. [PubMed] [Google Scholar]
- 6.Walters MC, Patience M, Leisenring W, Eckman JR, Scott JP, Mentzer WC, Davies SC, Ohene-Frempong K, Bernaudin F, Matthews DC, Storb R, Sullivan KM. Bone marrow transplantation for sickle cell disease. The New England Journal of Medicine. 1996;335:369–76. doi: 10.1056/NEJM199608083350601. [DOI] [PubMed] [Google Scholar]
- 7.Vermylen C, Cornu G, Ferster A, Brichard B, Ninane J, Ferrant A, Zenebergh A, Maes P, Dhooge C, Benoit Y, Beguin Y, Dresse MF, Sariban E. Haematopoietic stem cell transplantation for sickle cell anaemia: the first 50 patients transplanted in Belgium. Bone Marrow Transplantation. 1998;22:1–6. doi: 10.1038/sj.bmt.1701291. (1998) [DOI] [PubMed] [Google Scholar]
- 8.Bernaudin F, Socie G, Kuentz M, Chevret S, Duval M, Bertrand Y, Vannier JP, Yakouben K, Thuret I, Bordigoni P, Fischer A, Lutz P, Stephan JL, Dhedin N, Plouvier E, Margueritte G, Bories D, Verlhac S, Esperou H, Coic L, Vernant JP, Gluckman E SFGM-TC. Long-term results of related myeloablative stem-cell transplantation to cure sickle cell disease. Blood. 2007;110:2749–56. doi: 10.1182/blood-2007-03-079665. [DOI] [PubMed] [Google Scholar]
- 9.Majumdar S. Outcome of hematopoietic cell transplantation in children with sickle cell disease, a single center’s experience. Bone Marrow Transplantation. 2009:1–6. doi: 10.1038/bmt.2009.244. [DOI] [PubMed] [Google Scholar]
- 10.Lucarelli G, Isgrò A, Sodani P, Gaziev J. Hematopoietic Stem cell Transplantation in Thalassemia and Sickle Cell anemia. Cold Spring Harbor Perspectives in Medicine. 2012;2:a011825. doi: 10.1101/cshperspect.a011825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ribeil JA, Arlet JB, Dussiot M, Moura IC, Courtois G, Hermine O. Ineffective Erythropoiesis in??-Thalassemia. The Scientific World Journal. 2013. pp. 1–11. [DOI] [PMC free article] [PubMed]
- 12.Wu CJ, Krishnamurti L, Kutok JL, Biernacki M, Rogers S, Zhang W, Antin JH, Ritz J. Evidence for ineffective erythropoiesis in severe sickle cell disease. Blood. 2005;106:3639–3645. doi: 10.1182/blood-2005-04-1376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.De Maria R, Testa U, Luchetti L, Zeuner A, Stassi G, Pelosi E, Riccioni R, Felli N, Samoggia P, Peschle C. Apoptotic role of Fas/Fas ligand system in the regulation of erythropoiesis. Blood. 1999;93:796–803. [PubMed] [Google Scholar]
- 14.Koulnis M, Liu Y, Hallstrom K, Socolovsky M. Negative autoregulation by fas stabilizes adult erythropoiesis and accelerates its stress response. PLoS ONE. 2011;6:1–14. doi: 10.1371/journal.pone.0021192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Liu Y, Pop R, Sadegh C, Brugnara C, Haase VH, Socolovsky M. Suppression of Fas-FasL coexpression by erythropoietin mediates erythroblast expansion during the erythropoietic stress response in vivo. Blood. 2006;108:123–133. doi: 10.1182/blood-2005-11-4458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sodani P, Gaziev D, Polchi P, Erer B, Giardini C, Angelucci E, Baronciani D, Andreani M, Manna M, Nesci S, Lucarelli B, Clift RA, Lucarelli G. New approach for bone marrow transplantation in patients with class 3 thalassemia aged younger than 17 years. Blood. 2004;104:1201–1203. doi: 10.1182/blood-2003-08-2800. [DOI] [PubMed] [Google Scholar]
- 17.Glucksberg H, Storb R, Fefer A, Buckner CD, Neiman PE, Clift RA, Lerner KG, Thomas ED. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HLA-matched sibling donors. Transplantation. 1974;18(4):295–304. doi: 10.1097/00007890-197410000-00001. [DOI] [PubMed] [Google Scholar]
- 18.Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR, Lee SJ, Martin P, Chien J, Przepiorka D, Couriel D, Cowen EW, Dinndorf P, Farrell A, Hartzman R, Henslee-Downey J, Jacobsohn D, McDonald G, Mittleman B, Rizzo JD, Robinson M, Schubert M, Schultz K, Shulman H, Turner M, Vogelsang G, Flowers ME. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biology of Blood and Marrow Transplantation. 2005;11(12):945–956. doi: 10.1016/j.bbmt.2005.09.004. (2005) [DOI] [PubMed] [Google Scholar]
- 19.Chen K, Liu J, Heck S, Chasis JA, An X, Mohandas N. Resolving the distinct stages in erythroid differentiation based on dynamic changes in membrane protein expression during erythropoiesis. Proceedings of the National Academy of Sciences of the United States of America. 2009;106(41):17413–17418. doi: 10.1073/pnas.0909296106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kaplan EL, Meier P. Non parametric estimation from incomplete observations. Journal of the American Statistical Association. 1958;53:457–481. doi: 10.1080/01621459.1958.10501452. [DOI] [Google Scholar]
- 21.Blouin MJ, De Paepe ME, Trudel M. Altered hematopoiesis in murine sickle cell disease. Blood. 1999;94:1451–1459. [PubMed] [Google Scholar]
- 22.Grasso JA, Sullivan AL, Sullivan LW. Ultrastructural studies of the bone marrow in sicle cell anaemia, I: the structure of sickled erythrocytes and reticulocytes and their phagocytic destruction. British Journal of Haematology. 1975;31:135–148. doi: 10.1111/j.1365-2141.1975.tb00844.x. [DOI] [PubMed] [Google Scholar]
- 23.Grasso JA, Sullivan AL, Sullivan LW. Ultrastructural studies of the bone marrow in sickle cell anaemia, II: the morphology of erythropoietic cells and their response to deoxygenation in vitro. British Journal of Haematology. 1975;31:381–389. doi: 10.1111/j.1365-2141.1975.tb00869.x. [DOI] [PubMed] [Google Scholar]
- 24.Hasegawa S, Rodgers GP, Dwyer N, Noguchi CT, Blanchette-Mackie EJ, Uyesaka N, Schechter AN, Fibach E. Sickling of nucleated erythroid precursors from patients with sickle cell anemia. Experimental Hematology. 1998;26:314–319. [PubMed] [Google Scholar]
- 25.Isgrò A, Marziali M, Sodani P, Gaziev J, Erer B, Polchi P, Paciaroni K, Roveda A, De Angelis G, Gallucci C, Alfieri C, Simone MD, Zinno F, Isacchi G, Adorno G, Lanti A, Leti W, Aiuti F, Fraboni D, Andreani M, Lucarelli G. Immunohematologic reconstitution in pediatric patients after T cell-depleted HLA-haploidentical stem cell transplantation for thalassemia. Biology of Blood and Marrow Transplantation. 2010;16(11):1557–66. doi: 10.1016/j.bbmt.2010.05.003. [DOI] [PubMed] [Google Scholar]
- 26.Angelucci E, Matthes-Martin S, Baronciani D, Bernaudin F, Bonanomi S, Cappellini MD, Dalle JH, Di Bartolomeo P, de Heredia CD, Dickerhoff R, Giardini C, Gluckman E, Hussein AA, Kamani N, Minkov M, Locatelli F, Rocha V, Sedlacek P, Smiers F, Thuret I, Yaniv I, Cavazzana M, Peters C EBMT Inborn Error and EBMT Paediatric Working Parties. Hematopoietic stem cell transplantation in thalassemia major and sickle cell disease: indications and management recommendations from an international expert panel. Haematologica. 2014;99(5):811–20. doi: 10.3324/haematol.2013.099747. [DOI] [PMC free article] [PubMed] [Google Scholar]