

Abstract
Objectives
Herpes simplex virus type 2 (HSV-2) is a common sexually transmitted disease, but there is limited data on its epidemiology among urban populations. The urban Emergency Department (ED) is a potential venue for surveillance as it predominantly serves an inner city minority population. We evaluate the seroprevalence and factors associated with HSV-2 infection among patients attending the Johns Hopkins Hospital Adult Emergency Department (JHH ED).
Methods
An identity unlinked-serosurvey was conducted between 6/2007 and 9/2007 in the JHH ED; sera were tested by the Focus HerpeSelect ELISA. Prevalence risk ratios (PRR) were used to determine factors associated with HSV-2 infection.
Results
Of 3,408 serum samples, 1,853 (54.4%) were seropositive for HSV-2. Females (adjPRR = 1.47, 95% CI 1.38–1.56), non-Hispanic blacks (adjPRR = 2.03, 95% CI 1.82–2.27), single (adjPRR = 1.15, 95% CI 1.07–1.25), divorced (adjPRR = 1.28, 95% CI 1.15–1.41), and unemployed patients (adjPRR = 1.13, 95% CI 1.05–1.21) had significantly higher rates of HSV-2 infection. Though certain zip codes had significantly higher seroprevalence of HSV-2, this effect was completely attenuated when controlling for age and gender.
Conclusions
Seroprevalence of HSV-2 in the JHH ED was higher than U.S. national estimates; however, factors associated with HSV-2 infection were similar. The high seroprevalence of HSV-2 in this urban ED highlights the need for targeted testing and treatment. Cross-sectional serosurveys in the urban ED may help to examine the epidemiology of HSV-2.
Introduction
Herpes simplex virus type 2 (HSV-2) is one of the most common sexually transmitted infections worldwide. HSV-2 is primarily characterized by painful genital lesions and is a major cause of genital ulcer disease [1]. Observational studies suggest HSV-2 is associated with a three-fold increase in human immunodeficiency virus (HIV) acquisition [2]. HSV-2 can easily be transmitted by close contact between sexual partners. Although perinatal transmission is less common, it can be deadly to the fetus if it occurs [3], [4]. HSV-2 infection is often subclinical [5], and previous studies have shown that up to 87.4% of HSV-2 infected individuals in the United States are unaware of their infection [6], [7]. Thus, HSV-2 prevalence can only be monitored by serological surveillance.
The National Health and Nutrition Examination Survey (NHANES) has been the major serological study for the general population. In 2005–2010, NHANES reported that the seroprevalence of HSV-2 in the United States was 15.7% [8]. Modeled after NHANES, the 2004 New York City (NYC) Health and Nutrition Examination Survey (HANES) reported a higher HSV-2 seroprevalence (27.9%) [9]. Both studies indicated that being female, non-Hispanic black, and socioeconomically disadvantaged were factors associated with HSV-2 infection [6], [8], [9]. Aside from NYC HANES, recent data on HSV-2 seroprevalence and associated factors in urban settings is limited.
The urban Emergency Department (ED) is a potential venue for surveillance of HSV-2. The Johns Hopkins Hospital Adult Emergency Department (JHH ED) primarily sees a high proportion of individuals from the surrounding predominantly minority community, many of whom have poor access to healthcare and often use the ED for primary healthcare [10]–[12]. This patient population can be used to establish specific demographics associated with HSV-2 infection in disadvantaged urban settings. Urban ED surveillance has previously been beneficial in monitoring the prevalence of sexually transmitted infections such as HIV, chlamydia, and gonorrhea [10], [11], [13], [14]. Including HSV-2 serology in this well-defined surveillance method may help to characterize its epidemiology among urban populations. The purpose of this study was to describe the seroprevalence and associated factors of HSV-2 infection in the JHH ED in Baltimore City, Maryland.
Methods
Ethics Statement
The study was conducted according to the ethical standards set forth by the institutional review board of the Johns Hopkins University and the Helsinki Declaration of the World Medical Association. As the study was an identity unlinked serosurvey, the need to obtain consent was waived. No participants were recruited or followed-up during the course of this study. All laboratory testing was performed on the remnants of blood samples obtained for patient care.
Study Population and Laboratory Testing
An identity-unlinked serosurvey was conducted from 6/2007 to 9/2007 in the JHH ED in Baltimore City, Maryland. The protocol for the study was the same as previously described [10]. In brief, eligible patients were ≥18 years of age, required blood drawn for a medical reason, and had matched chart review data. For patients who attended the JHH ED multiple times within the study period, only one serum sample was included for testing. Patients who listed their home as a non-US location were excluded from the study population. Serological HSV-2 infection status was determined by the Focus HerpeSelect-2 enzyme-linked immunosorbent assay (Focus Technologies, Cypress, California, U.S.) per kit protocol.
Statistical Analysis
Zip code boundary data from 2007 was obtained from the Maryland Department of Planning, and only zip codes with ≥40 patients were included in the analyses. For HSV-2 seroprevalence, exact 95% confidence intervals (CIs) were assessed from a binomial distribution. Prevalence risk ratios (PRRs) of HSV-2 seroprevalence were estimated using a Poisson regression model. Adjusted PRRs (adjPRRs) were estimated using a multivariate regression model for all factors shown to have an association (p<0.1) in the univariate analysis. In all statistical analyses, p<0.05 determined significant differences. Data analyses for the study were performed in STATA V.11.2 (StataCorp, College Station, Texas, U.S.).
Results
Study Population
The study population included 3,408 unique samples (median age = 45.3 years, interquartile range 33.2–56.8). The majority of samples came from females (54.0%), non-Hispanic blacks (67.4%), the unemployed (57.8%), unmarried individuals (75.6%), and Baltimore City residents (78.5%). Almost one-third of the patients sampled did not have any form of health insurance (32.0%). All results are available in Table S1.
Seroprevalence of HSV-2
In the study population, 1,853 (54.4%) were seropositive for HSV-2. Seroprevalence was highest among females (63.6%), patients older than 25 years of age (57.9%), non-Hispanic blacks (66.3%), divorced (66.3%) or widowed (66.2%) patients, the unemployed (58.3%), patients on Medicare (55.5%), and Baltimore City residents (59.4%) (Table 1).
Table 1. Factors associated with HSV-2 infection in the JHH ED (n = 3,408).
| n | Prevalence (95% CI) | PRR (95% CI) | adjPRR (95% CI)1 | |
| Gender | ||||
| Male | 1,568 | 43.5% (41.0–46.0) | 1.00 | 1.00 |
| Female | 1,840 | 63.6% (61.4–65.8) | 1.46 (1.37–1.56)* | 1.47 (1.38–1.56)* |
| Age | ||||
| 18–24 | 386 | 26.4% (22.1–31.1) | 1.00 | 1.00 |
| 25–34 | 560 | 49.3% (45.1–53.5) | 1.87 (1.55–2.25)* | 2.07 (1.73–2.48)* |
| 35–44 | 729 | 62.1% (58.5–65.7) | 2.35 (1.97–2.80)* | 2.57 (2.16–3.05)* |
| 45–54 | 769 | 61.9% (58.4–65.3) | 2.34 (1.97–2.79)* | 2.55 (2.15–3.03)* |
| 55–64 | 467 | 59.3% (54.7–63.8) | 2.24 (1.87–2.69)* | 2.53 (2.11–3.02)* |
| >65 | 497 | 54.1% (49.6–58.6) | 2.05 (1.70–2.46)* | 2.30 (1.90–2.80)* |
| Race | ||||
| Non-Hispanic whites | 918 | 29.1% (26.2–32.1) | 1.00 | 1.00 |
| Non-Hispanic blacks | 2,297 | 66.3% (64.3–68.2) | 2.28 (2.05–2.53)* | 2.03 (1.82–2.27)* |
| Other | 193 | 33.2% (26.6–40.3) | 1.14 (0.91–1.43) | 1.20 (0.96–1.50) |
| Marital Status | ||||
| Married | 813 | 45.5% (42.0–49.0) | 1.00 | 1.00 |
| Single | 2,086 | 55.1% (52.9–57.2) | 1.21 (1.11–1.32)* | 1.15 (1.07–1.25)* |
| Divorced | 297 | 66.3% (60.6–71.7) | 1.46 (1.30–1.63)* | 1.28 (1.15–1.41)* |
| Widowed | 195 | 66.2% (59.0–72.8) | 1.45 (1.28–1.65)* | 1.13 (1.01–1.27)† |
| Employment Status | ||||
| Employed | 910 | 47.1% (43.9–50.4) | 1.00 | 1.00 |
| Unemployed | 1,969 | 58.3% (56.0–60.4) | 1.24 (1.14–1.34)* | 1.13 (1.05–1.21)* |
| Retired | 295 | 54.6% (48.7–60.4) | 1.16 (1.02–1.31)† | 1.15 (1.00–1.32)† |
| Other | 144 | 55.6% (47.1–63.8) | 1.18 (1.00–1.39) | 1.13 (0.97–1.31) |
| Insurance | ||||
| Insured | 1,624 | 53.7% (51.2–56.1) | 1.00 | - |
| Uninsured | 1,092 | 54.9% (51.8–57.8) | 1.02 (0.95–1.10) | - |
| Medicare | 647 | 55.5% (51.6–59.4) | 1.03 (0.95–1.12) | - |
| Residence | ||||
| Baltimore City | 2,675 | 59.4% (57.6–61.3) | 1.00 | 1.00 |
| Other Maryland | 549 | 36.8% (32.7–41.0) | 0.62 (0.55–0.69)* | 0.85 (0.77–0.95)* |
| Other State | 184 | 33.2% (26.4–40.5) | 0.56 (0.45–0.69)* | 0.83 (0.67–1.03) |
| Overall | 3,408 | 54.4% (52.7–56.1) | - | - |
*p<0.01.
p<0.05.
Adjusted for gender, age, race, marital status, employment status, and residence.
The highest seroprevalence of HSV-2 was seen in non-Hispanic black females (Figure 1). Those 18–24 years of age had a seroprevalence of 41.3% (74/179). Seroprevalence plateaued in non-Hispanic black females ≥35 years of age at 82.8% (736/889). Among non-Hispanic black males, the seroprevalence was at least 20% less than that of the non-Hispanic black females for all age groups, plateauing for patients ≥35 years of age at 61.4% (477/777). The seroprevalence of non-Hispanic white females increased to a maximum of 49.3% (35/71) among patients 35–44 years of age, followed by a significant decrease in seroprevalence of 35.2% (81/230) in those ≥45 years of age. Non-Hispanic white males followed the same trend as non-Hispanic white females, but peaked at 33.7% (34/101) among patients 45–54 years of age, with a significant decrease in seroprevalence of 20.9% (34/163) in those ≥55 years of age.
Figure 1. HSV-2 seroprevalence in the JHH ED stratified by age, gender, and race.

Data are shown for 3,215 non-Hispanic black and non-Hispanic white patients that attended the JHH Adult ED in Baltimore City. Blue lines indicate non-Hispanic blacks and grey lines indicate non-Hispanic whites. Circles and squares denote females and males, respectively. Bars display 95% confidence intervals.
The seroprevalence of HSV-2 varied significantly by zip code. When identified as residing within Baltimore City, the seroprevalence ranged from a high of 73.9% (85/115, 95% CI 64.9%–81.7%) in zip code 21217 to a low of 45.3% (101/223, 95% CI 38.6%–52.1%) in zip code 21224 (Figure 2). The seroprevalence of HSV-2 was lower for patients who were non-Maryland residents (32.6%, 61/187, 95% CI 26.0%–40.0%). Relative to the zip code where the JHH ED is located (21205), two zip codes (21224 and 21222), and patients who lived outside of Maryland had significantly lower seroprevalence of HSV-2. However, the effect was completely attenuated after controlling for age and gender, apart from those living outside of Maryland.
Figure 2. HSV-2 seroprevalence in the JHH ED by Baltimore City zip code.
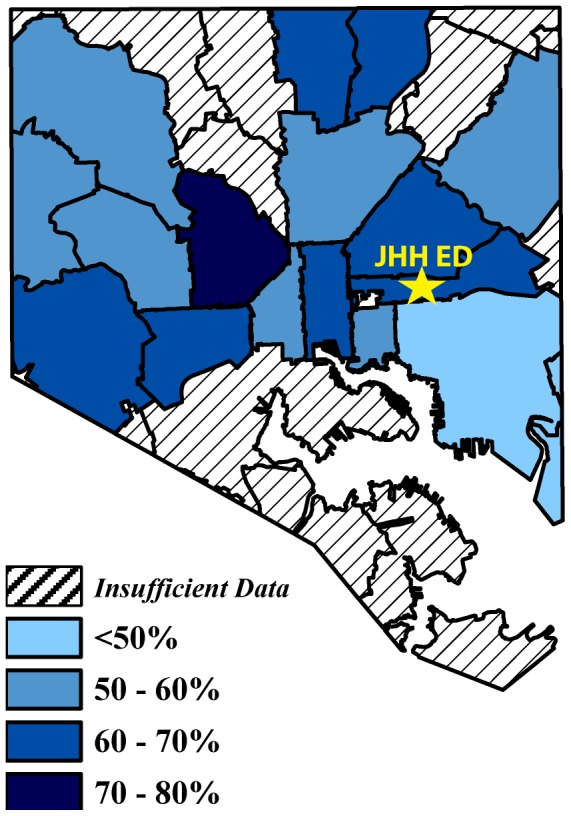
Only zip codes that had ≥40 patient visits to the JHH ED are included in the map as a function of HSV-2 seroprevelance. The map was constructed using 2007 zip code boundary data obtained from the Maryland Department of Planning. The star indicates the JHH ED in zipcode 21205.
Factors Associated with HSV-2 Infection
In the univariate analyses, gender, age, race, employment status, marital status, and residency were significantly associated with HSV-2 prevalence (Table 1). All associated factors remained stable in predicting risk in the multivariate model. Females (adjPRR = 1.47, 95% CI 1.38–1.56), non-Hispanic blacks (adjPRR = 2.03, 95% CI 1.82–2.27), single (adjPRR = 1.15, 95% CI 1.07–1.25), divorced (adjPRR = 1.28, 95% CI 1.15–1.41), and unemployed patients (adjPRR = 1.13, 95% CI 1.05–1.21) were at a significantly higher risk for HSV-2 infection. There was no association between insurance status and HSV-2 seroprevalence (Table 1).
Discussion
This is the first reported study that examines seroprevalence and associated risk factors of HSV-2 in patients attending an inner city ED. The results of this study indicate a high seroprevalence (54.4%) of HSV-2 in the JHH ED, a likely reflection of Baltimore City ED patients. The findings of higher seroprevalence among females, non-Hispanic blacks, patients ≥25 years of age, unmarried, and unemployed patients are similar to previous studies in urban and general populations [8], [9], [15]–[17].
Due to the chronic nature of HSV-2 infection and results of previous studies, it was expected that older patients would have the highest seroprevalence [8]. The largest difference in seroprevalence among age groups was observed between those 18–24 years of age and those 25–34 years of age. Between every age group ≥35 years, overall seroprevalence did not differ. These results may be explained by an increase in HSV-2 incidence in the 20 s age group and a decrease in HSV-2 incidence in the mid-30 s age, as previously reported from a population-based birth cohort study [15]. Nevertheless, the high seroprevalence seen across all ages suggests the need for HSV-2 prevention education to decrease acquisition and transmission.
Although a disparity in HSV-2 seroprevalence between non-Hispanic blacks and non-Hispanic whites is well established [6], [18], the high prevalence among non-Hispanic blacks in the current study is concerning. In older aged non-Hispanic whites, there was a decrease in HSV-2 prevalence, but in non-Hispanic blacks, high seroprevalence persisted (see Figure 1). Most alarming is that 82.8% of non-Hispanic black females ≥35 years of age were seropositive. Inner city non-Hispanic black females are significantly at-risk for HSV-2 infection and would certainly benefit from an HSV-2 vaccine.
The findings from this study support previous studies that suggested a higher seroprevalence in urban settings compared to the general population [9], [16], [17]. Not only is the overall seroprevalence in this study population higher than national estimates from NHANES [8], it is higher than the overall seroprevalence reported in New York City [9] and among military recruits [17]. The majority of patients that used the JHH ED were non-Hispanic blacks, which may explain the higher overall prevalence than previous studies. However, even the seroprevalence among the non-Hispanic black female population and non-Hispanic black male population in this study is respectively higher than the seroprevalence found in NYC HANES, NHANES and military recruits [6], [9], [17]. While surveillance of the general population is necessary, continued surveillance of high-risk populations is also important as results greatly differ.
Increasing the diagnosis of HSV-2 in the urban ED may help to expand care, prevent future outbreaks in seropositive patients, and subsequently reduce transmission [19]–[22]. Although the current guidelines from the U.S. Preventative Services Task Force recommend against routine serologic screening for HSV-2 [23], an algorithm for targeted HSV-2 testing may benefit high-risk populations. This study highlights certain factors associated with HSV-2 infection in an urban ED, but future studies should evaluate additional risk factors that have not been examined in this setting. For instance, substance abuse and sexual risk, including sexual orientation, age of sexual debut, and number of lifetime partners are key risk factors for HSV-2 infection in the general population [7], [8], [24].
This study has limitations. As with any serosurvey, errors of misclassification in serological testing are possible. Multiple studies have demonstrated the Focus HerpeSelect-2 assay to have 96–100% sensitivity and 97–100% specificity compared to HSV-2 western blotting, and this assay is currently used for HSV-2 research diagnostics [25]. However, in men attending STD clinics in Baltimore, Maryland the assay only had 82.6% sensitivity and 97.1% specificity, which suggests that our study may contain false-negative results [26]. Additionally, the prevalence among the youngest (<20 years of age) non-Hispanic black females and males were 21% (9/43) and 5% (2/44), respectively. This provides assurance that the results seen in the current study are not due to a high false positive rate of the assay. Also, only patients who had their blood drawn were included in the study population, thus these data may not be generalizable to the entire ED patient population. However, a previous JHH ED serosurvey reported that the ED patient population without blood drawn was demographically similar to the study population [10]. Finally, due to the cross-sectional nature of this study, temporal changes in HSV-2 epidemiology cannot be assessed without future studies of the same design.
Overall, the JHH ED has the highest seroprevalence of HSV-2 ever reported from a single unselected population screening site in the U.S. Although differences in seroprevalence existed across groups, this study highlights a high seroprevalence of HSV-2 across all demographics. Enhanced public health interventions to prevent and control HSV-2 infection in high prevalence populations like this ED are severely needed. The current study also demonstrates that the ED may be a key setting to monitor the epidemiology of HSV-2.
Supporting Information
Data used in analysis. Variables coded as follows: ID, subject identifier; Insured_0Yes_1No_2Medicare, 0 = insured 1 = not insured 2 = Medicare; Baltimore_Resident, 1 = yes 2 = no; MD_Resident 1 = yes 2 = no; ZipCode, resident zip code for subjects where the frequency was more than 40 individuals from that area; Gender_0F_1M, 0 = female 1 = male; Age, age in years; Race_0W_1B_2Other, 0 = non-Hispanic white 1 = non-Hispanic black 2 = other; Marital _ Status _0 Married_1Single_2 Divorced_3 Widowed, 0 = married 1 = not married 2 = divorced 3 = widowed; Employed_ 0Yes_1No_2 Retired_3Other, 0 = employed 1 = not employed 2 = retired 3 = other; HSV2_EIA_results, 0 = HSV-2 serologically negative 1 = HSV-2 serologically positive.
(XLSX)
Acknowledgments
The authors acknowledge the medical students and nurses who assisted in the study.
Data Availability
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper and its Supporting Information files.
Funding Statement
The work was supported in part by the Division of Intramural Research and Dr. Hsieh is supported in part by an NIH Award, 5K01AI100681 from NIAID. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Corey L, Handsfield HH (2000) Genital herpes and public health: addressing a global problem. JAMA 283: 791–794. [DOI] [PubMed] [Google Scholar]
- 2. Tobian AA, Quinn TC (2009) Herpes simplex virus type 2 and syphilis infections with HIV: an evolving synergy in transmission and prevention. Curr Opin HIV AIDS 4: 294–299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Brown ZA, Selke S, Zeh J, Kopelman J, Maslow A, et al. (1997) The acquisition of herpes simplex virus during pregnancy. N Engl J Med 337: 509–515. [DOI] [PubMed] [Google Scholar]
- 4. Corey L, Wald A (2009) Maternal and neonatal herpes simplex virus infections. N Engl J Med 361: 1376–1385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Wald A, Zeh J, Selke S, Ashley RL, Corey L (1995) Virologic characteristics of subclinical and symptomatic genital herpes infections. N Engl J Med 333: 770–775. [DOI] [PubMed] [Google Scholar]
- 6. Fanfair RN, Zaidi A, Taylor LD, Xu F, Gottlieb S, et al. (2013) Trends in seroprevalence of herpes simplex virus type 2 among non-Hispanic blacks and non-Hispanic whites aged 14 to 49 years–United States, 1988 to 2010. Sex Transm Dis 40: 860–864. [DOI] [PubMed] [Google Scholar]
- 7. Fleming DT, McQuillan GM, Johnson RE, Nahmias AJ, Aral SO, et al. (1997) Herpes simplex virus type 2 in the United States, 1976 to 1994. N Engl J Med 337: 1105–1111. [DOI] [PubMed] [Google Scholar]
- 8. Bradley H, Markowitz LE, Gibson T, McQuillan GM (2014) Seroprevalence of herpes simplex virus types 1 and 2–United States, 1999-2010. J Infect Dis 209: 325–333. [DOI] [PubMed] [Google Scholar]
- 9. Schillinger JA, McKinney CM, Garg R, Gwynn RC, White K, et al. (2008) Seroprevalence of herpes simplex virus type 2 and characteristics associated with undiagnosed infection: New York City, 2004. Sex Transm Dis 35: 599–606. [DOI] [PubMed] [Google Scholar]
- 10. Kelen GD, Fritz S, Qaqish B, Brookmeyer R, Baker JL, et al. (1988) Unrecognized human immunodeficiency virus infection in emergency department patients. N Engl J Med 318: 1645–1650. [DOI] [PubMed] [Google Scholar]
- 11. Kelen GD, Hexter DA, Hansen KN, Tang N, Pretorius S, et al. (1995) Trends in human immunodeficiency virus (HIV) infection among a patient population of an inner-city emergency department: implications for emergency department-based screening programs for HIV infection. Clin Infect Dis 21: 867–875. [DOI] [PubMed] [Google Scholar]
- 12. Kelen GD, DiGiovanna T, Bisson L, Kalainov D, Sivertson KT, et al. (1989) Human immunodeficiency virus infection in emergency department patients. Epidemiology, clinical presentations, and risk to health care workers: the Johns Hopkins experience. JAMA 262: 516–522. [DOI] [PubMed] [Google Scholar]
- 13.Jenkins WD, Nessa LL, Clark T (2013) Cross-sectional study of pharyngeal and genital chlamydia and gonorrhoea infections in emergency department patients. Sex Transm Infect. [DOI] [PubMed]
- 14. Mehta SD, Rompalo A, Rothman RE, Londner MS, Zenilman JM (2003) Generalizability of STD screening in urban emergency departments: comparison of results from inner city and urban sites in Baltimore, Maryland. Sex Transm Dis 30: 143–148. [DOI] [PubMed] [Google Scholar]
- 15.Dickson N, Righarts A, van Roode T, Paul C, Taylor J, et al.. (2013) HSV-2 incidence by sex over four age periods to age 38 in a birth cohort. Sex Transm Infect. [DOI] [PubMed]
- 16. Siegel D, Golden E, Washington AE, Morse SA, Fullilove MT, et al. (1992) Prevalence and correlates of herpes simplex infections. The population-based AIDS in Multiethnic Neighborhoods Study. JAMA 268: 1702–1708. [PubMed] [Google Scholar]
- 17. Page WF, Chubb M, Feng X, Fan LY, Li Y, et al. (2012) National estimates of seroincidence and seroprevalence for herpes simplex virus type 1 and type 2 among US military adults aged 18 to 29 years. Sex Transm Dis 39: 241–250. [DOI] [PubMed] [Google Scholar]
- 18. Bernstein DI, Bellamy AR, Hook EW 3rd, Levin MJ, Wald A, et al. (2013) Epidemiology, clinical presentation, and antibody response to primary infection with herpes simplex virus type 1 and type 2 in young women. Clin Infect Dis 56: 344–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Wald A, Zeh J, Barnum G, Davis LG, Corey L (1996) Suppression of subclinical shedding of herpes simplex virus type 2 with acyclovir. Ann Intern Med 124: 8–15. [DOI] [PubMed] [Google Scholar]
- 20. Gupta R, Wald A, Krantz E, Selke S, Warren T, et al. (2004) Valacyclovir and acyclovir for suppression of shedding of herpes simplex virus in the genital tract. J Infect Dis 190: 1374–1381. [DOI] [PubMed] [Google Scholar]
- 21. Corey L, Ashley R, Valaciclovir HSVTSG (2004) Prevention of herpes simplex virus type 2 transmission with antiviral therapy. Herpes 11 Suppl 3170A–174A. [PubMed] [Google Scholar]
- 22. Corey L, Wald A, Patel R, Sacks SL, Tyring SK, et al. (2004) Once-daily valacyclovir to reduce the risk of transmission of genital herpes. N Engl J Med 350: 11–20. [DOI] [PubMed] [Google Scholar]
- 23.Force USPST (2005) Screening for genital herpes: recommendation statement.
- 24. Xu F, Sternberg MR, Kottiri BJ, McQuillan GM, Lee FK, et al. (2006) Trends in herpes simplex virus type 1 and type 2 seroprevalence in the United States. JAMA 296: 964–973. [DOI] [PubMed] [Google Scholar]
- 25. Wald A, Ashley-Morrow R (2002) Serological testing for herpes simplex virus (HSV)-1 and HSV-2 infection. Clin Infect Dis 35: S173–182. [DOI] [PubMed] [Google Scholar]
- 26. Summerton J, Riedesel M, Laeyendecker O, Gaydos C, Maldeis NE, et al. (2007) Effect of sexually transmitted disease (STD) coinfections on performance of three commercially available immunosorbent assays used for detection of herpes simplex virus type 2-specific antibody in men attending Baltimore, Maryland, STD clinics. Clin Vaccine Immunol 14: 1545–1549. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data used in analysis. Variables coded as follows: ID, subject identifier; Insured_0Yes_1No_2Medicare, 0 = insured 1 = not insured 2 = Medicare; Baltimore_Resident, 1 = yes 2 = no; MD_Resident 1 = yes 2 = no; ZipCode, resident zip code for subjects where the frequency was more than 40 individuals from that area; Gender_0F_1M, 0 = female 1 = male; Age, age in years; Race_0W_1B_2Other, 0 = non-Hispanic white 1 = non-Hispanic black 2 = other; Marital _ Status _0 Married_1Single_2 Divorced_3 Widowed, 0 = married 1 = not married 2 = divorced 3 = widowed; Employed_ 0Yes_1No_2 Retired_3Other, 0 = employed 1 = not employed 2 = retired 3 = other; HSV2_EIA_results, 0 = HSV-2 serologically negative 1 = HSV-2 serologically positive.
(XLSX)
Data Availability Statement
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper and its Supporting Information files.