

Abstract
Purpose:
To evaluate the concordance of estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 (HER2) statuses between ultrasound (US)-guided 14-gauge core needle biopsy (CNB) and surgery and to analyze whether the clinicopathological and imaging features including those from mammography and ultrasonography can predict the concordance in breast cancer patients.
Methods:
The concordance of receptor status between CNB and surgery was assessed for 55 breast cancers in 55 women who underwent CNB before treatment. The clinicopathological and imaging features and the concordance rates were compared between the non-neoadjuvant chemotherapy (non-NAC) group and the NAC group according to the initial treatment. The concordance rates were analyzed according to the clinicopathological and imaging features, by using the chi-square or Fisher exact test and McNemar test for the categorical and the independent t-test for continuous variables.
Results:
Among 55 women, 22 women (40%) were part of the non-NAC group and 33 women (60%) were part of the NAC group. The concordance rates were 0.86-1.00 in the non-NAC group and 0.76-0.88 in the NAC group. In all three receptors, the difference in the concordance rate between the two groups was not significant. In the NAC group, the absence of axillary lymph node metastasis (1.00, P=0.02) and visibility of cancer on mammography (0.93, P=0.04) showed the higher concordance of the HER2 status.
Conclusion:
Concordance of the receptor status between surgery and US-guided 14-gauge CNB was feasible in breast cancer patients. The absence of axillary lymph node metastasis after NAC and the visibility of cancer on mammography prior to NAC may be helpful for predicting the concordance of HER2 in breast cancer patients.
Keywords: Breast neoplasms; Receptors, estrogen; Receptors, progesterone; HER-2 protein; Biopsy, large-core needle
Introduction
Breast cancer is not a single disease entity but rather a group of heterogeneous diseases with various morphologies, clinical courses, and responses to treatment. An immunohistochemical profile based on the extent of the expression of the estrogen receptor (ER), the progesterone receptor (PR), and the human epidermal growth factor receptor 2 (HER2) is the most frequently used molecular marker, and identifies subgroups of breast cancer patients with different outcomes and responsiveness to systemic therapies [1]. Immunohistochemistry can provide prognostic and predictive information for specific therapies. For example, negative hormone receptor status or HER2 overexpression is associated with worse prognosis and tumors expressing hormone receptors or HER2 response to endocrine therapy or trastuzumab therapy, respectively [2].
Percutaneous core needle biopsy (CNB) is almost as accurate as open excision biopsy and is now accepted as a reliable alternative to surgical biopsy for the diagnosis of breast lesions [3]. Regarding the growing demand for prognostic and predictive information, in particular, the determination of hormone receptors and HER2 status for the treatment planning of neoadjuvant chemotherapy (NAC), CNB provides enough material to allow early determination of the receptor status. In cases achieving a pathologically complete response after NAC, a CNB specimen may be the only tissue available for the consideration of postsurgical care [4].
However, the concordance of the receptor status between CNB and the surgical specimen is of concern, particularly in patients with NAC. There have been several studies regarding the concordance of the receptor status between CNB and the subsequent surgical excision [4-9]. However, the data were from CNB performed using various needle gauges, biopsy methods, and imaging techniques used for guidance. The increase in the number of breast cancer patients being treated with NAC with the subsequent achievement of a pathologically complete remission requires an accurate assessment of biomarkers in the CNB material. Therefore, evaluating the predictive clinical and imaging factors including mammography and ultrasound (US) features for the concordance of the receptor status would be of clinical value. To the best of our knowledge, there are no studies concerning the imaging findings including those of mammography and ultrasonography that are predictive of the concordance of the receptor status.
The purpose of this study was to evaluate the concordance of ER, PR, and HER2 status between US-guided 14-gauge CNB and surgery and to analyze whether the clinicopathological and imaging findings including those of the mammography and ultrasonography can predict the concordance in breast cancer patients.
Materials and Methods
This retrospective study was conducted with the approval of the institutional review board and a waiver of patient informed consent.
Case Selection
From January 2008 to the end of June 2012, 753 consecutive breast mass surgeries were performed at our institution. After a review of the pathological results, we identified 408 invasive breast cancers. Among these lesions, 353 cancers that had an unknown receptor status at histopathology in CNB (n=265) and surgery (n=88) were excluded from the study. Therefore, a total of 55 invasive breast cancers in 55 women who had a known receptor status at histopathology in US-guided 14-gauge CNB and surgery were enrolled in this study.
Clinicopathological Studies
The patients’ medical records were reviewed for their clinical and histopathological findings. The clinical findings included patient age, clinical symptoms (i.e., palpable mass or nipple discharge), and the history of NAC prior to the surgery. Pathological reports of excisional biopsies, breast-conserving surgery, or mastectomy specimens were reviewed to determine tumor type, tumor stage, histological grade, and the presence of axillary lymph node metastasis. Further, the pathologic result after US-guided CNB was obtained. For surgical biopsy and CNB, the assigned receptor status of ER, PR, and HER2 was noted.
To determine the receptor status, an immunohistochemical analysis was performed. Formalin-fixed, paraffin-embedded tissue sections were immunohistochemically stained with appropriate antibodies for ER (Novocastra, Newcastle upon Tyne, UK), PR (Novocastra), and HER2 (Ventana Medical Systems, Tucson, AZ, USA). ER and PR were determined by nuclear staining graded from 0 to 8 by using the Allred score [10]. The results were categorized as positive when the total score, expressed as the sum of the proportion score and the immunointensity score, was 3 or more. With respect to the HER2 evaluation, membranous staining was graded as follows: score 0, 1+, 2+, and 3+ [4]. The HER2 status was deemed to be positive at the score of 3+ and negative at the score of 0 or 1+. Tumors scored at 2+ were sent for fluorescence in situ hybridization testing performed using the PathVysion HER2 DNA Probe Kit (Abbott-Vysis, Des Plaines, IL, USA) to determine the amplification if the ratio of the HER2 gene signal to the chromosome 17 signal was more than 2, which is classified as positive. Fluorescence in situ hybridization was done in about 24% (13/55) of the cases. Histological diagnoses were made by a single pathologist with 27 years of experience in breast histologic evaluation.
Imaging Acquisition and Biopsy
Mammograms were performed with dedicated digital mammography units (Senographe 2000D, GE Healthcare, Milwaukee, WI; Selenia Full Field Digital Mammography System, Lorad/Hologic, Danbury, CT, USA). Standard craniocaudal and mediolateral oblique views were routinely obtained, and additional mammographic views were obtained as needed.
US examination and US-guided CNBs were performed before surgery or NAC, with high-resolution US units with 7.5-12-MHz or 4-15-MHz linear-array transducers (iU22, Philips Healthcare, Bothell, WA, USA; SuperSonic Imagine, Aix-en-Provence, France). The final assessment categorization of each US examination was analyzed prospectively by one of six radiologists with 3-12 years of experience in breast ultrasonography who performed the examination according to the American College of Radiology Breast Image Reporting and Data Systems (BI-RADS) [11]. US-guided CNBs were performed with a 14-gauge dual-action semiautomatic core biopsy needle (Stericut with coaxial; TSK Laboratory, Tochigi, Japan) by one of six radiologists with 3-12 years of experience in breast biopsy under US guidance. Our standard protocol was that at least four core samples per lesion were obtained.
Image Evaluation
Each image was reviewed retrospectively in consensus by two radiologists who were specialized in breast imaging with 2 and 7 years of experience, respectively, without knowledge of the clinicopathological findings other than invasive breast cancers. The images evaluated of the patients who underwent NAC were the ones taken prior to NAC. On mammograms, which were available for 53 of the 55 patients, mammographic visibility of the cancer and the presence of calcification associated with the cancer were evaluated. On the ultrasonogram, the lesion size and the following sonographic features were determined according to the BI-RADS: shape, margin, orientation, boundary, echo pattern, posterior acoustic feature, and ductal change. The prospectively assigned US BI-RADS final assessment categories were documented.
Data and Statistical Analysis
The clinicopathological and imaging features were compared between the non-NAC group and the NAC group. The pathologic findings including histologic diagnosis and receptor status of the CNB were compared with those of the subsequent surgery. The concordance of the ER, PR, and HER2 status between CNB and surgical excision was analyzed according to the clinicopathological and imaging features and compared between the non-NAC group and the NAC group. Statistical comparisons were performed using the chi-square or Fisher exact tests and McNemar test for categorical data, and the independent t-test for continuous data.
Statistical analysis was performed with PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA). Differences were considered to be statistically significant at P<0.05.
Results
The patients were divided into two groups: the non-NAC group and the NAC group. The non-NAC group was the group of patients who did not receive NAC prior to the surgery. The NAC group included patients who underwent NAC prior to the surgery. Among 55 patients, 33 patients (60.0%) belonged to the NAC group and 22 patients (40.0%) to the non-NAC group. Mastectomy was performed for 46 patients, and breast-conserving surgery was performed for 9 patients. In the NAC group, 19 patients were administered 3-6 cycles of doxorubicin and paclitaxel; 5 with 3-6 cycles of cyclophosphamide, doxorubicin, and fluorouracil; 4 with 4-5 cycles of doxorubicin and cyclophosphamide; 1 with 4 cycles of doxorubicin and cyclophosphamide and subsequently 12 cycles of paclitaxel; 1 with 3 cycles of capecitabine and paclitaxel combined; 1 with 6 cycles of trastuzumab and paclitaxel combined; and 2 with trastuzumab. All treatments were carried out in 3-week cycles except those for the 19 patients receiving doxorubicin and paclitaxel; they followed 2-week cycles.
The clinicopathological features are summarized in Table 1. Among the 45 symptomatic patients, there were 41 patients who presented with a palpable lesion and 4 with nipple discharge. There was no significant difference in any of the variables between the non-NAC group and the NAC group. Table 2 presents the imaging findings of the non-NAC group and the NAC group. Although the mean sonographic lesion size in the NAC group showed a trend of being larger than that in the non-NAC group, there was no significant difference between the two groups (P=0.36). On the ultrasonogram, all cancers were hypoechoic and assessed as BI-RADS category 4b or more. No significant difference was found in mammography and US features between the non-NAC group and the NAC group.
Table 1.
Clinicopathological features of the surgery and NAC group
| Variable | All patients | Non-NAC groupa) | NAC groupb) | P-value |
|---|---|---|---|---|
| Age (yr), mean±SD (range) | 48.1±11.9 (27-82) | 52.0±13.5 (36-82) | 45.5±10.1 (27-66) | 0.05 |
| Symptom | ||||
| Present | 45 (81.8) | 16 (72.7) | 29 (87.9) | 0.18 |
| Absent | 10 (18.2) | 6 (27.3) | 4 (12.1) | |
| Histologic gradec) | 0.74 | |||
| I | 3 (6.1) | 2 (9.1) | 1 (3.7) | |
| II | 26 (53.1) | 15(50.0) | 11 (55.6) | |
| III | 20 (40.8) | 11 (40.9) | 9 (40.7) | |
| T stage | 0.41 | |||
| 1 | 24 (43.6) | 12 (54.5) | 12 (36.4) | |
| 2 | 25 (45.5) | 8 (36.4) | 17 (51.5) | |
| 3 | 6 (10.9) | 2 (9.1) | 4 (12.1) | |
| Axillary LN metastasisd) | 0.15 | |||
| Present | 26 (47.3) | 13 (59.1) | 13 (39.4) | |
| Absent | 29 (52.7) | 9 (40.9) | 20 (60.6) | |
| Cancer type | >0.99 | |||
| Ductal | 51 (92.7) | 20 (91.0) | 31 (94.0) | |
| Lobular | 2 (3.6) | 1 (4.5) | 1 (3.0) | |
| Others | 2 (3.6) | 1 (4.5) | 1 (3.0) |
Values are presented as number (%).
NAC, neoadjuvant chemotherapy; LN, lymph node.
Non-NAC group was the group of patients who went through surgery without prior NAC.
NAC group was the group of patients who went through NAC prior to surgery.
Available for only 49 cases.
Available for only 54 cases.
Table 2.
Mammography and ultrasound features of the surgery and neoadjuvant chemotherapy (NAC) group
| Variable | All patients | Non-NAC group a) | NAC groupb) | P-value |
|---|---|---|---|---|
| Mammography feature | ||||
| Visibility on mammography c) | >0.99 | |||
| Not visible | 5 (9.4) | 2 (9.5) | 3 (9.4) | |
| Visible | 48 (90.6) | 19 (90.5) | 29 (90.6) | |
| Calcification c) | 0.39 | |||
| Present | 34 (64.2) | 12 (57.1) | 22 (68.8) | |
| Absent | 19 (35.8) | 9 (42.9) | 10 (31.2) | |
| Ultrasound feature | ||||
| Mean lesion diameter (mm) | 28.3±18.4 (6-100) | 25.5±17.3 (6-70) | 30.2±19.1 (9-100) | 0.36 |
| Shape | 0.49 | |||
| Oval | 28 (50.9) | 13 (59.1) | 15 (45.5) | |
| Round | 2 (3.6) | 0 (0) | 2 (6.1) | |
| Irregular | 25 (45.5) | 9 (40.9) | 16 (48.4) | |
| Margin | 0.21 | |||
| Circumscribed | 1 (1.8) | 0 (0) | 1 (3.0) | |
| Ill-defined | 21 (38.2) | 6 (27.3) | 15 (45.5) | |
| Spiculated | 33 (60.0) | 16 (72.7) | 17 (51.5) | |
| Orientation | 0.90 | |||
| Parallel | 42 (76.4) | 17 (77.3) | 25 (75.8) | |
| Nonparallel | 13 (23.6) | 5 (22.7) | 8 (24.2) | |
| Boundary | 0.63 | |||
| Abrupt interface | 17 (30.9) | 6 (27.3) | 11 (33.3) | |
| Echogenic halo | 38 (69.1) | 16 (72.7) | 22 (66.7) | |
| Posterior feature | 0.20 | |||
| None | 39 (70.9) | 18 (81.8) | 21 (63.6) | |
| Enhancement | 12 (21.8) | 4 (18.2) | 8 (24.2) | |
| Shadowing | 4 (7.3) | 0 (0) | 4 (12.1) | |
| Ductal dilatation | 0.64 | |||
| Present | 4 (7.3) | 1 (4.5) | 3 (9.1) | |
| Absent | 51 (92.7) | 21 (95.5) | 30 (90.9) | |
| Ultrasound category | 0.67 | |||
| 4b | 1(1.8) | 1 (4.6) | 0 (0) | |
| 4c | 8 (14.6) | 3 (13.6) | 5 (15.2) | |
| 5 | 46 (83.6) | 18 (81.8) | 28 (84.8) |
Values are presented as number (%).
Non-NAC group was the group of patients who went through surgery without prior NAC.
NAC group was the group of patients who went through NAC prior to surgery.
Available for only 53 lesions.
In all lesions, the histological cancer type in CNB was correlated exactly with that in the surgical excision. The final diagnosis was as follows: invasive ductal carcinoma (n=51, 92.8%), invasive lobular carcinoma (n=2, 3.6%), metaplastic carcinoma (n=1, 1.8%), and mucinous carcinoma (n=1, 1.8%). Regarding the receptor status after surgery, ER was expressed in 31 patients (56.4%), PR in 23 patients (41.8%), and HER2 in 20 patients (36.4%). In the non- NAC group and the NAC group, the hormonal receptors of the surgical specimen were expressed in 63.6% (14/22) and 51.5% (17/33) for ER (P=0.38), 50.0% (11/22) and 36.4% (12/33) for PR (P=0.32), and 31.8% (7/22) and 39.4% (13/33) for HER2 (P=0.57), respectively.
Table 3 summarizes the receptor status and the concordance rate between CNB and surgery. The concordance rate for ER, PR, and HER2 was 1.00, 0.86, and 0.86 in the non-NAC group and 0.88, 0.76, and 0.88 in the NAC group, respectively. Each receptor status was not significantly different between CNB and surgery in all groups. Among the three receptors, there was no significant difference in the concordance rate for each group. Further, the concordance rate of each receptor status was not significantly different between the non-NAC group and the NAC group (P=0.14 for ER, P=0.50 for PR, and P>0.99 for HER2).
Table 3.
Comparison of receptor status between core needle biopsy and surgery
| Receptor status | Surgery | P-valuea) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Core needle biopsy | ER | PR | HER2 | |||||||
| + | - | + | - | + | - | |||||
| All patients | 0.14 | |||||||||
| + | 27 | 0 | 20 | 8 | 17 | 4 | ||||
| - | 4 | 24 | 3 | 24 | 3 | 31 | ||||
| P-valueb) | 0.13 | 0.23 | >0.99 | |||||||
| Concordance rate (%) | 93 | 80 | 87 | |||||||
| Non-NAC groupc) | 0.23 | |||||||||
| + | 14 | 0 | 11 | 3 | 5 | 1 | ||||
| - | 0 | 8 | 0 | 8 | 2 | 14 | ||||
| P-valueb) | >0.99 | 0.25 | >0.99 | |||||||
| Concordance rate (%) | 100 | 86 | 86 | |||||||
| NAC groupd) | 0.30 | |||||||||
| + | 13 | 0 | 9 | 5 | 12 | 3 | ||||
| - | 4 | 16 | 3 | 16 | 1 | 17 | ||||
| P-valueb) | 0.13 | 0.73 | 0.63 | |||||||
| Concordance rate (%) | 88 | 76 | 88 | |||||||
ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; NAC, neoadjuvant chemotherapy.
P-values indicate a comparison among the three receptors.
P-values indicate a comparison of the receptor status between core needle biopsy and surgery.
Non-NAC group was the group of patients who went through surgery without prior NAC.
NAC group was the group of patients who went through NAC prior to surgery.
Table 4 summarizes the concordance rate of the receptor status between CNB and surgery on the basis of the clinicopathological findings. In the NAC group, the absence of axillary lymph node metastasis (1.00, P=0.02) showed a significantly higher concordance rate of the HER2 status between CNB and surgery. However, in the case of the ER and PR status as well as the non-NAC group, none of the clinicopathological features showed a significant difference in the concordance rate.
Table 4.
Concordance rate according to clinical and pathological features
| Variable | All patients |
Non-NAC groupa) |
NAC groupb) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| ER | PR | HER2 | ER | PR | HER2 | ER | PR | HER2 | |
| Age (yr) | |||||||||
| <40 | 91.7 (11/12) | 75.0 (9/12) | 91.7 (11/12) | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) | 90.9 (10/11) | 72.7 (8/11) | 90.9 (10/11) |
| ≥40 | 93.0 (40/43) | 79.1 (34/43) | 86.0 (37/43) | 100.0 (21/21) | 85.7 (18/21) | 85.7 (18/21) | 86.4 (19/22) | 72.7 (16/22) | 86.4 (19/22) |
| P-value | >0.99 | 0.712 | >0.99 | NA | >0.99 | >0.99 | >0.99 | >0.99 | >0.99 |
| Symptom | |||||||||
| Present | 72.7 (8/11) | 90.9 (10/11) | 90.9 (10/11) | 100.0 (7/7) | 85.7 (6/7) | 85.7 (6/7) | 75.0 (3/4) | 50.0 (2/4) | 100.0 (4/4) |
| Absent | 79.5 (35/44) | 93.2 (41/44) | 86.4 (38/44) | 100.0 (15/15) | 86.7 (13/15) | 86.7 (13/15) | 89.7 (26/29) | 75.9 (22/29) | 86.2 (25/29) |
| P-value | 0.69 | >0.99 | >0.99 | NA | >0.99 | >0.99 | 0.42 | 0.30 | >0.99 |
| Histologic grade | |||||||||
| I | 100.0 (3/3) | 100.0 (3/3) | 66.7 (2/3) | 100.0 (2/2) | 100.0 (2/2) | 50.0 (1/2) | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) |
| II | 100.0 (26/26) | 76.9 (20/26) | 88.5 (23/26) | 100.0 (11/11) | 81.8 (9/11) | 81.8 (9/11) | 100.0 (15/15) | 73.3 (11/15) | 93.3 (14/15) |
| III | 85.0 (17/20) | 85.0 (17/20) | 95.0 (19/20) | 100.0 (9/9) | 88.9 (8/9) | 100.0 (9/9) | 72.7 (8/11) | 81.8 (9/11) | 90.9 (10/11) |
| P-value | 0.15 | 0.84 | 0.29 | NA | >0.99 | 0.19 | 0.17 | >0.99 | >0.99 |
| T stage | |||||||||
| 1 | 95.8 (23/24) | 75.0 (18/24) | 83.3 (20/24) | 100.0 (12/12) | 83.3 (10/12) | 83.3 (10/12) | 91.7 (11/12) | 66.7 (8/12) | 83.3 (10/12) |
| 2 | 92.0 (23/25) | 80.0 (20/25) | 92.0 (23/25) | 100.0 (8/8) | 87.5 (7/8) | 87.5 (7/8) | 88.2 (15/17) | 76.5 (13/17) | 94.1 (16/17) |
| 3 | 83.3 (5/6) | 83.3 (5/6) | 83.3 (5/6) | 100.0 (2/2) | 100.0 (2/2) | 100.0 (2/2) | 75.0 (3/4) | 75.0 (3/4) | 75.0 (3/4) |
| P-value | 0.56 | 0.87 | 0.63 | 0.811 | 0.811 | 0.675 | 0.838 | 0.478 | |
| Axillary LN metastasis | |||||||||
| Present | 92.3 (24/26) | 80.8 (21/26) | 84.6 (22/26) | 100.0 (13/13) | 84.9 (11/13) | 100.0 (13/13) | 84.6 (11/13) | 76.9 (10/13) | 69.2 (9/13) |
| Absent | 93.1 (27/29) | 75.9 (22/29) | 89.7 (26/29) | 100.0 (9/9) | 88.9 (8/9) | 66.7 (6/9) | 90.0 (18/20) | 70.0 (14/20) | 100.0 (20/20) |
| P-value | >0.99 | 0.66 | 0.696 | NA | >0.99 | 0.06 | >0.99 | >0.99 | 0.02 |
Values are percentages of concordant cases.
NAC, neoadjuvant chemotherapy; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; NA, not applicable; LN, lymph node.
Non-NAC group was the group of patients who went through surgery without prior neoadjuvant chemotherapy.
NAC group was the group of patients who went through neoadjuvant chemotherapy prior to surgery.
Table 5 summarizes the concordance rate of the receptor status between CNB and surgery on the basis of the mammography and US findings. In the NAC group, the visibility of cancer on mammography (0.93, P=0.04) showed a significantly higher concordance rate of the HER2 status between CNB and surgery (Fig. 1). In all patients, the visibility of cancer on mammography showed a significantly higher concordance rate of the HER2 status (0.90, P=0.01) (Figs. 1, 2). However, in the case of the ER and PR status as well as the non-NAC group, none of the imaging features showed a significant difference in the concordance rate.
Table 5.
Concordance rate according to mammography and ultrasound features
| Variable | All patients |
Non-NAC groupa) |
NAC groupb) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| ER | PR | HER2 | ER | PR | HER2 | ER | PR | HER2 | |
| Mammography feature | |||||||||
| Visibility on mammogramc) | |||||||||
| Not visible | 100.0 (5/5) | 80.0 (4/5) | 60.0 (2/5) | 100.0 (2/2) | 50.0 (1/2) | 50.0 (1/2) | 100.0 (3/3) | 100.0 (3/3) | 33.3 (1/3) |
| Visible | 91.7 (44/48) | 79.2 (38/48) | 93.8 (45/48) | 100.0 (19/19) | 89.5 (17/19) | 94.7 (18/19) | 86.2 (25/29) | 72.4 (21/29) | 93.1 (27/29) |
| P-value | >0.99 | >0.99 | 0.01 | NA | 0.27 | 0.19 | >0.99 | 0.56 | 0.04 |
| Calcificationc) | |||||||||
| Present | 88.2 (30/34) | 76.5 (26/34) | 91.2 (31/34) | 100.0 (12/12) | 83.3 (10/12) | 100.0 (12/12) | 81.8 (18/22) | 72.7 (16/22) | 86.4 (19/22) |
| Absent | 100.0 (19/19) | 84.2 (16/19) | 84.2 (16/19) | 100.0 (9/9) | 88.9 (8/9) | 77.8 (7/9) | 100.0 (10/10) | 80.0 (8/10) | 90.0 (9/10) |
| P-value | 0.28 | 0.73 | 0.66 | NA | >0.99 | 0.17 | 0.28 | >0.99 | >0.99 |
| Ultrasound feature | |||||||||
| Shape | |||||||||
| Oval | 92.9 (26/28) | 71.4 (20/28) | 85.7 (24/28) | 100.0 (13/13) | 100.0 (10/13) | 84.6 (11/13) | 86.7 (13/15) | 66.7 (10/15) | 86.7 (13/15) |
| Round | 100.0 (2/2) | 50.0 (1/2) | 100.0 (2/2) | (0/0) | (0/0) | (0/0) | 100.0 (2/2) | 50.0 (1/2) | 100.0 (2/21) |
| Irregular | 92.0 (23/25) | 88.0 (22/25) | 88.0 (22/25) | 100.0 (22/25) | 100.0 (9/9) | 88.9 (8/9) | 87.5 (14/16) | 75.0 (13/16) | 87.5 (14/16) |
| P-value | >0.99 | 0.14 | >0.99 | NA | NA | >0.99 | >0.99 | 0.73 | >0.99 |
| Margin | |||||||||
| Circumscribed | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) | (0/0) | (0/0) | (0/0) | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) |
| Ill-defined | 95.2 (20/21) | 81.0 (17/21) | 90.5 (19/21) | 100.0 (6/6) | 66.7 (4/6) | 83.3 (5/6) | 93.3 (14/15) | 88.2 (13/15) | 93.3 (14/15) |
| Spiculated | 90.9 (30/33) | 75.8 (25/33) | 84.8 (28/33) | 100.0 (16/16) | 93.8 (15/16) | 87.5 (14/16) | 82.4 (14/17) | 58.8 (10/17) | 82.4 (14/17) |
| P-value | >0.99 | 0.80 | 0.73 | NA | 0.17 | >0.99 | 0.65 | 0.15 | 0.65 |
| Orientation | |||||||||
| Parallel | 90.5 (38/42) | 78.6 (33/42) | 85.7 (36/42) | 100.0 (17/17) | 88.2 (15/17) | 88.2 (15/17) | 84.0 (21/25) | 72.0 (18/25) | 84.0 (21/25) |
| Nonparallel | 100.0 (13/13) | 76.9 (10/13) | 92.3 (12/13) | 100.0 (5/5) | 80.0 (4/5) | 80.0 (4/5) | 100.0 (8/8) | 75.0 (6/8) | 100.0 (8/8) |
| P-value | 0.56 | >0.99 | >0.99 | NA | >0.99 | >0.99 | 0.55 | >0.99 | 0.55 |
| Boundary | |||||||||
| Abrupt interface | 94.1 (16/17) | 76.5 (13/17) | 88.2 (15/17) | 100.0 (6/6) | 83.3 (5/6) | 83.3 (5/6) | 90.9 (10/11) | 72.7 (8/11) | 90.9 (10/11) |
| Echogenic halo | 92.1 (35/38) | 78.9 (30/38) | 86.8 (33/38) | 100.0 (16/16) | 87.5 (14/16) | 87.5 (14/16) | 86.4 (19/22) | 72.7 (16/22) | 86.4 (19/22) |
| P-value | >0.99 | >0.99 | >0.99 | NA | >0.99 | >0.99 | >0.99 | >0.99 | >0.99 |
| Posterior feature | |||||||||
| None | 92.3 (36/39) | 82.1 (32/39) | 84.6 (33/39) | 100.0 (18/18) | 88.9 (16/18) | 83.3 (15/18) | 85.7 (18/21) | 76.2 (16/21) | 85.7 (18/21) |
| Enhancement | 91.7 (11/12) | 75.0 (9/12) | 100.0 (12/12) | 100.0 (4/4) | 75.0 (3/4) | 100.0 (4/4) | 87.5 (7/8) | 75.0 (6/8) | 100.0 (8/8) |
| Shadowing | 100.0 (4/4) | 50.0 (2/4) | 75.0 (38/4) | (0/0) | (0/0) | (0/0) | 100.0 (4/4) | 50.0 (2/4) | 75.0 (3/4) |
| P-value | >0.99 | 0.28 | 0.21 | NA | 0.47 | >0.99 | >0.99 | 0.63 | 0.29 |
| Ductal dilatation | |||||||||
| Present | 75.0 (3/4) | 100.0 (4/4) | 100.0 (4/4) | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) | 66.7 (2/3) | 100.0 (3/3) | 100.0 (3/3) |
| Absent | 94.1 (48/51) | 95.1 (39/51) | 86.3 (44/51) | 100.0 (21/21) | 85.7 (18/21) | 85.7 (18/21) | 90.0 (27/30) | 70.0 (21/30) | 86.7 (26/30) |
| P-value | 0.27 | >0.99 | >0.99 | NA | >0.99 | >0.99 | 0.33 | 0.55 | >0.99 |
| Ultrasound category | |||||||||
| 4b | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) | 100.0 (1/1) | (0/0) | (0/0) | (0/0) |
| 4c | 87.5 (7/8) | 75.0 (6/8) | 75.0 (6/8) | 100.0 (3/3) | 66.7 (2/3) | 66.7 (2/3) | 80.0 (4/5) | 80.0 (4/5) | 80.0 (4/5) |
| 5 | 93.5 (43/36) | 78.3 (36/46) | 89.1 (41/46) | 100.0 (18/18) | 88.9 (16/18) | 88.9 (16/18) | 89.3 (25/8) | 72.7 (20/28) | 89.3 (25/28) |
| P-value | 0.52 | >0.99 | 0.37 | NA | 0.47 | 0.47 | 0.50 | >0.99 | 0.50 |
Values are percentages of concordant cases.
NAC, neoadjuvant chemotherapy; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; NA, not applicable.
Non-NAC group was the group of patients who went through surgery without prior neoadjuvant chemotherapy.
NAC group was the group of patients who went through neoadjuvant chemotherapy prior to surgery.
Available for only 53 lesions.
Fig 1. Invasive ductal carcinoma in the left breast of a 66-year-old patient with concordance in the human epidermal growth factor receptor 2 (HER2) status between core needle biopsy (HER2 negative) and the surgical specimen (HER2 negative) after neoadjuvant chemotherapy.
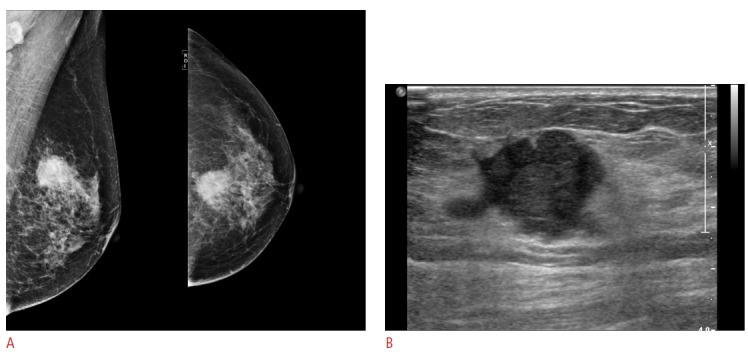
A. Mammography shows a spiculated mass in the left breast. B. Ultrasonogram shows a 19-mm hypoechoic mass in the left breast.
Fig 2. Invasive ductal carcinoma in the left breast of a 55-year-old patient with discordance in the human epidermal growth factor receptor 2 (HER2) status between core needle biopsy (HER2 positive) and the surgical specimen (HER2 negative) after neoadjuvant chemotherapy.
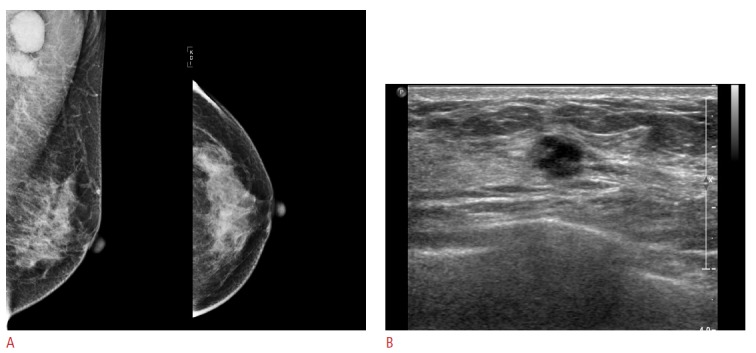
A. Mammography does not show any visible mass in the left breast. B. Ultrasonogram shows an 8-mm microlobulated, hypoechoic mass in the left breast.
Discussion
Receptor status as the immunohistochemical profile has been compared between CNB and surgery, and various concordance rates reported were 61%-99%, 61%-91%, and 64%-96% for ER, PR, and HER2, respectively [4,12-15]. This wide variability of the concordance rates can be explained by the heterogeneity in patient characteristics, biopsy methods, the gauge of the core needle, the number of core samples obtained, methodology, or cutoff value standards [16]. In our study, the CNB specimen obtained by using a constant 14-gauge needle under US guidance was evaluated; the concordance rate (71%-100%) was found to be within the range of the reported rates. With respect to the number of core samples, our standard protocol was that at least four core samples per lesion had to be obtained as recommended by Tamaki et al. [17] while assessing the hormone receptor and HER2 status.
In the non-NAC group of our study, ER showed perfect concordance rate of 100% and PR and HER2 showed a concordance rate of 86% between CNB and surgery, which was compatible with previous reports [12-15]. In other words, the discordance rate of PR and HER2 status was 14%, which cannot be considered negligible since the receptor status determines the therapeutic strategy. This discordance of the receptor status between CNB and surgery might have been explained by the relatively small sample size of the CNB specimen, tumor heterogeneity, and sampling errors [4,16,18]. Although the receptor status of the surgical specimen is assumed to be the gold standard and determines the adjuvant endocrine and anti-HER2 therapy, it was reported that the hormone receptor status in the CNB specimen was more reliable than that in the surgical specimen due to better fixation on the core samples [2,19]. Therefore, when determining the endocrine therapy, the information of both surgery and CNB should be considered. With respect to the high concordance rate, it was recommended that the hormone receptor activity be retested on patients whose hormonal receptors were found to be negative for either CNB or surgery in order to avoid an erroneous omission of a life-saving endocrine therapy [16].
Concordance of the hormone receptor and HER2 status between CNB and surgery is a clinical matter of concern, as the increasing number of breast cancer patients being treated with NAC and subsequently achieving a pathologically complete remission has given rise to the need for an accurate assessment of biomarkers in the CNB material [20]. NAC itself has been thought to change the receptor status of breast cancer. The two possible explanations for this are follows: (1) When NAC targets the chemo-sensitive tumor cells, it leaves behind insensitive tumor cells with a different biology in the residual tumor, and (2) it might change the receptor status and biology of the tumor cells as a survival mechanism of the tumor cells as resistance to the NAC [21]. However, the information on the receptor status is usually obtained from CNB performed before NAC and surgery performed after NAC; therefore, the receptor status conversion after NAC could be the cause of the discordance between CNB and surgery as well as NAC itself. A comparison of the concordance rate between the non-NAC group and the NAC group revealed no significant difference (Table 3). Similarly, Arens et al. [22] performed a study comparing the hormone receptor and HER2 status between the NAC group and the control group, and there were no significant differences in the receptor status conversion. On the basis of these results, we speculated that the receptor status conversion after NAC was more attributable to the discordance between CNB and surgery than to NAC itself. To determine the adjuvant endocrine therapy in the NAC group, it was suggested that endocrine therapy be suitable for patients with tumors that tested positive for the hormone receptor status at least once, that is, either before or after NAC [23]; further, if applicable, a repeat assay of the resected surgical specimen is mandatory [18,24].
In the subset of breast cancer patients who achieve a pathologically complete remission, do not have residual tumor tissue in the excisional biopsy for retesting, and are eligible for adjuvant therapy including endocrine or anti-HER2 therapy, predicting the discordance rate of the receptor status between CNB and surgery could be crucial [5,16]. There have been studies on the factors that affect the discordance rate of the receptor status of CNB and surgery; however, these studies focused on the technical factors associated with CNB or pathologic study [10,19]. In our study, the absence of axillary lymph node metastasis and the visibility on mammography in the NAC group showed higher concordance for HER2. Therefore, on the basis of the axillary lymph node status and mammography, trastuzumab treatment could be carried out with confidence according to the HER2 status of CNB in NAC patients, even in those with pathologically complete remission. Unfortunately, there were no US features predictable demonstrating concordance in our study. Further detailed study on the relationship between the US features and the concordance of the receptor status is recommended. In the future, the outcome of adjuvant therapy based on this strategy should be evaluated to validate our results.
Our study was limited in some ways. Because of the retrospective design, a selection bias may have existed. Further, the patient population included was small. Only 14% of the cancer cases (55/408), the patients who had information on the receptor status in both CNB and surgery, were included during the study period. The receptor status on CNB might have been evaluated in patients who were expected to go on NAC, which could result in no significant difference between the surgery and the NAC group. Moreover, factors for immunohistochemical staining were not evaluated, and ER and PR statuses were determined by nuclear staining graded from 0 to 8 using the Allred score instead of the international standard of 1%. The discordances in the receptor status may have arisen from fixation or technical artifacts [19,21]. Lastly, the NAC protocol was varied according to the patients’ condition, and different regimens were used among the patients.
In conclusion, the concordance of the receptor status between surgery and US-guided 14-gauge CNB was feasible in breast cancer patients. The absence of axillary lymph node metastasis after NAC and the visibility of cancer on mammography prior to NAC may be helpful for predicting the concordance of HER2 in breast cancer patients.
Footnotes
No potential conflict of interest relevant to this article was reported
References
- 1.Montagna E, Bagnardi V, Rotmensz N, Viale G, Cancello G, Mazza M, et al. Immunohistochemically defined subtypes and outcome in occult breast carcinoma with axillary presentation. Breast Cancer Res Treat. 2011;129:867–875. doi: 10.1007/s10549-011-1697-6. [DOI] [PubMed] [Google Scholar]
- 2.Rakha EA, Reis-Filho JS, Ellis IO. Combinatorial biomarker expression in breast cancer. Breast Cancer Res Treat. 2010;120:293–308. doi: 10.1007/s10549-010-0746-x. [DOI] [PubMed] [Google Scholar]
- 3.Bruening W, Fontanarosa J, Tipton K, Treadwell JR, Launders J, Schoelles K. Systematic review: comparative effectiveness of coreneedle and open surgical biopsy to diagnose breast lesions. Ann Intern Med. 2010;152:238–246. doi: 10.7326/0003-4819-152-1-201001050-00190. [DOI] [PubMed] [Google Scholar]
- 4.Arnedos M, Nerurkar A, Osin P, A'Hern R, Smith IE, Dowsett M. Discordance between core needle biopsy (CNB) and excisional biopsy (EB) for estrogen receptor (ER), progesterone receptor (PgR) and HER2 status in early breast cancer (EBC) Ann Oncol. 2009;20:1948–1952. doi: 10.1093/annonc/mdp234. [DOI] [PubMed] [Google Scholar]
- 5.Rakha EA, Ellis IO. An overview of assessment of prognostic and predictive factors in breast cancer needle core biopsy specimens. J Clin Pathol. 2007;60:1300–1306. doi: 10.1136/jcp.2006.045377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Al Sarakbi W, Salhab M, Thomas V, Mokbel K. Is preoperative core biopsy accurate in determining the hormone receptor status in women with invasive breast cancer? Int Semin Surg Oncol. 2005;2:15. doi: 10.1186/1477-7800-2-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Colditz GA, Rosner BA, Chen WY, Holmes MD, Hankinson SE. Risk factors for breast cancer according to estrogen and progesterone receptor status. J Natl Cancer Inst. 2004;96:218–228. doi: 10.1093/jnci/djh025. [DOI] [PubMed] [Google Scholar]
- 8.Moeder CB, Giltnane JM, Harigopal M, Molinaro A, Robinson A, Gelmon K, et al. Quantitative justification of the change from 10% to 30% for human epidermal growth factor receptor 2 scoring in the American Society of Clinical Oncology/College of American Pathologists guidelines: tumor heterogeneity in breast cancer and its implications for tissue microarray based assessment of outcome. J Clin Oncol. 2007;25:5418–5425. doi: 10.1200/JCO.2007.12.8033. [DOI] [PubMed] [Google Scholar]
- 9.Prechtel K, de Waal J, Nerlich A, Holzel D, Weitz J. Percutaneous large core breast biopsy. Pathologe. 2006;27:193–197. doi: 10.1007/s00292-005-0800-3. [DOI] [PubMed] [Google Scholar]
- 10.Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol. 1998;11:155–168. [PubMed] [Google Scholar]
- 11.American College of Radiology . ACR Breast Imaging Reporting and Data System, Breast Imaging Atlas. Reston, VA: American College of Radiology; 2003. pp. 1–84. [Google Scholar]
- 12.Park SY, Kim KS, Lee TG, Park SS, Kim SM, Han W, et al. The accuracy of preoperative core biopsy in determining histologic grade, hormone receptors, and human epidermal growth factor receptor 2 status in invasive breast cancer. Am J Surg. 2009;197:266–269. doi: 10.1016/j.amjsurg.2007.11.024. [DOI] [PubMed] [Google Scholar]
- 13.Cavaliere A, Sidoni A, Scheibel M, Bellezza G, Brachelente G, Vitali R, et al. Biopathologic profile of breast cancer core biopsy: is it always a valid method? Cancer Lett. 2005;218:117–121. doi: 10.1016/j.canlet.2004.07.041. [DOI] [PubMed] [Google Scholar]
- 14.Sutela A, Vanninen R, Sudah M, Berg M, Kiviniemi V, Rummukainen J, et al. Surgical specimen can be replaced by core samples in assessment of ER, PR and HER-2 for invasive breast cancer. Acta Oncol. 2008;47:38–46. doi: 10.1080/02841860701441822. [DOI] [PubMed] [Google Scholar]
- 15.Usami S, Moriya T, Amari M, Suzuki A, Ishida T, Sasano H, et al. Reliability of prognostic factors in breast carcinoma determined by core needle biopsy. Jpn J Clin Oncol. 2007;37:250–255. doi: 10.1093/jjco/hym021. [DOI] [PubMed] [Google Scholar]
- 16.Chen X, Yuan Y, Gu Z, Shen K. Accuracy of estrogen receptor, progesterone receptor, and HER2 status between core needle and open excision biopsy in breast cancer: a meta-analysis. Breast Cancer Res Treat. 2012;134:957–967. doi: 10.1007/s10549-012-1990-z. [DOI] [PubMed] [Google Scholar]
- 17.Tamaki K, Sasano H, Ishida T, Miyashita M, Takeda M, Amari M, et al. Comparison of core needle biopsy (CNB) and surgical specimens for accurate preoperative evaluation of ER, PgR and HER2 status of breast cancer patients. Cancer Sci. 2010;101:2074–2079. doi: 10.1111/j.1349-7006.2010.01630.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.van de Ven S, Smit VT, Dekker TJ, Nortier JW, Kroep JR. Discordances in ER, PR and HER2 receptors after neoadjuvant chemotherapy in breast cancer. Cancer Treat Rev. 2011;37:422–430. doi: 10.1016/j.ctrv.2010.11.006. [DOI] [PubMed] [Google Scholar]
- 19.Mann GB, Fahey VD, Feleppa F, Buchanan MR. Reliance on hormone receptor assays of surgical specimens may compromise outcome in patients with breast cancer. J Clin Oncol. 2005;23:5148–5154. doi: 10.1200/JCO.2005.02.076. [DOI] [PubMed] [Google Scholar]
- 20.D'Alfonso T, Liu YF, Monni S, Rosen PP, Shin SJ. Accurately assessing her-2/neu status in needle core biopsies of breast cancer patients in the era of neoadjuvant therapy: emerging questions and considerations addressed. Am J Surg Pathol. 2010;34:575–581. doi: 10.1097/PAS.0b013e3181d65639. [DOI] [PubMed] [Google Scholar]
- 21.Tacca O, Penault-Llorca F, Abrial C, Mouret-Reynier MA, Raoelfils I, Durando X, et al. Changes in and prognostic value of hormone receptor status in a series of operable breast cancer patients treated with neoadjuvant chemotherapy. Oncologist. 2007;12:636–643. doi: 10.1634/theoncologist.12-6-636. [DOI] [PubMed] [Google Scholar]
- 22.Arens N, Bleyl U, Hildenbrand R. HER2/neu, p53, Ki67, and hormone receptors do not change during neoadjuvant chemotherapy in breast cancer. Virchows Arch. 2005;446:489–496. doi: 10.1007/s00428-005-1244-0. [DOI] [PubMed] [Google Scholar]
- 23.Hirata T, Shimizu C, Yonemori K, Hirakawa A, Kouno T, Tamura K, et al. Change in the hormone receptor status following administration of neoadjuvant chemotherapy and its impact on the long-term outcome in patients with primary breast cancer. Br J Cancer. 2009;101:1529–1536. doi: 10.1038/sj.bjc.6605360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kasami M, Uematsu T, Honda M, Yabuzaki T, Sanuki J, Uchida Y, et al. Comparison of estrogen receptor, progesterone receptor and Her-2 status in breast cancer pre- and post-neoadjuvant chemotherapy. Breast. 2008;17:523–527. doi: 10.1016/j.breast.2008.04.002. [DOI] [PubMed] [Google Scholar]