

Abstract
Background and purpose
There is no consensus regarding the clinical relevance of gender-specific prostheses in total knee arthroplasty (TKA). We summarize the current best evidence in a comparison of clinical and radiographic outcomes between gender-specific prostheses and standard unisex prostheses in female patients.
Methods
We used the PubMed, Embase, Cochrane, Science Citation Index, and Scopus databases. We included randomized controlled trials published up to January 2013 that compared gender-specific prostheses with standard unisex prostheses in female patients who underwent primary TKAs.
Results
6 trials involving 423 patients with 846 knee joints met the inclusion criteria. No statistically significant differences were observed between the 2 designs regarding pain, range of motion (ROM), knee scores, satisfaction, preference, complications, and radiographic results. The gender-specific design (Gender Solutions; Zimmer Inc, Warsaw, Indiana) reduced the prevalence of overhang. However, it had less overall coverage of the femoral condyles compared to the unisex group. In fact, the femoral prosthesis in the standard unisex group matched better than that in the gender-specific group.
Interpretation
Gender-specific prostheses do not appear to confer any benefit in terms of clinician- and patient-reported outcomes for the female knee.
Women account for almost two-thirds of knee arthroplasties (Kurtz et al. 2007). Recently, a possible effect of gender on functional outcomes and implant survivorship has been identified (Vincent et al. 2006, Ritter et al. 2008, Kamath et al. 2010, Parsley et al. 2010, O’Connor 2011). Gender differences in the anatomy of the distal femur are well documented (Conley et al. 2007, Yue et al. 2011a, b, Yan et al. 2012, Zeng et al. 2012). Women tend to have a less prominent anterior condyle (Conley et al. 2007, Fehring et al. 2009), a higher quadriceps angle (Q-angle) (Hsu et al. 1990, Woodland et al. 1992), and a reduced mediolateral to anteroposterior aspect ratio (Chin et al. 2002, Chaichankul et al. 2011). Investigators have found that standard unisex knee prostheses may not equally match the native anatomy in male and female knees (Clarke and Hentz 2008, Yan et al. 2012). A positive association between the femoral component size and the amount of overhang was observed in females, and femoral component overhang (≥ 3 mm) may result in postoperative knee pain or reduced ROM (Hitt et al. 2003, Lo et al. 2003, Mahoney et al. 2010).
The concept of gender-specific knee prostheses was introduced to match these 3 anatomic differences in the female population (Conley et al. 2007). It includes a narrower mediolateral diameter for a given anteroposterior dimension, to match the female knee more closely. Additionally, the anterior flange of the prothesis was modified to include a recessed patellar sulcus and reduced anterior condylar height (to ovoid “overstuffing” during knee flexion) and a lateralized patellar sulcus (to accommodate the increased Q-angle associated with a wider pelvis).
Several randomized controlled trials (RCTs) have failed to establish the superiority of the gender-specific prosthesis over the unisex knee prosthesis in the female knee (Kim et al. 2010a, b, Song et al. 2012a, Thomsen et al. 2012, von Roth et al. 2013). In contrast, other studies have found higher patient satisfaction and better radiographic fit in the gender-specific TKAs than in the standard unisex TKAs (Clarke and Hentz 2008, Parratte et al. 2011, Yue et al. 2014). We therefore performed a systematic review and meta-analysis to compare the clinical and radiographic results of TKA in female patients receiving gender-specific prostheses or standard unisex prostheses.
Material and methods
Our systematic review and meta-analysis was conducted according to the PRISMA guidelines.
Search strategy and eligibility criteria
With the help of a librarian, we performed an electronic search of the current literature up to January 2013 using the PubMed, Embase, Cochrane, Science Citation Index, and Scopus databases. We used the following key words: knee arthroplasty, knee replacement, knee arthroplasties, knee replacements, TKA, TKR, gender, sex, female, gender-specifc, sex-specific, and female-specific. Additional strategies to identify relevant studies included: (1) a manual search of the table of contents of 5 major orthopedic journals (Journal of Bone and Joint Surgery (American and British); Clinical Orthopaedics and Related Research; Journal of Arthroplasty; Knee Surgery, Sports Traumatology, Arthroscopy; and The Knee) from 2005 through December 2012; (2) a literature search of the bibliographies of all the retrieved reports that evaluated clinical outcomes following the use of gender-specific knee prostheses; (3) a review of the titles of meeting abstracts from Orthopaedic Proceedings. No restrictions were placed on the origin or language of the publications.
First, all the articles comparing the outcomes of gender-specific and unisex prostheses were retrieved. In order to be included in the systematic review and meta-analysis, the studies had to meet the following criteria: (1) they had to have been described as a ‘‘randomized controlled trial (RCT)’’ related to primary TKA; (2) the subjects of the study had to have been women with severe knee arthrosis; (3) female-specific knee prostheses had to have been selected; and (4) follow-up had to have been more than 1 year. We excluded case reports, case series, editorials, commentaries, letters to the editor, and reviews, but these were read to identify any potential articles.
Study identification
2 reviewers (TC and CZ) independently screened titles, abstracts, and full-text papers for possible relevance. The reviewers were not blinded as to authors, geographic location, and hospital affiliation. Disagreements between the reviewers were resolved by consensus. If a disagreement remained, a third reviewer resolved the disagreement by consensus after discussing the inclusion and exclusion criteria with the other reviewers.
Data extraction and assessment of methodological quality
For each eligible study, one reviewer (TC) extracted relevant data including country of origin, year of publication, financial support, demographic data (age and body mass index (BMI)), postoperative pain, range of motion (ROM), knee scores (e.g. Knee Society score (KSS), Hospital for Special Surgery score (HSS), or Western Ontario and McMaster Universities osteoarthritis score (WOMAC)), postoperative complications, patient satisfaction and preference, femoral component fit, and radiographic results. These data were then cross-referenced by the second reviewer. If necessary, the original authors were contacted for more information and clarification of data.
2 of the present authors (JW and MC) independently assessed the methodological quality of each included study regarding randomization method, allocation concealment, blinding of patients/assessors, equality of baseline characteristics, adequate description of inclusion/exclusion criteria, similarity of postoperative program, sample size calculation, and the proportion of patients lost during follow-up. The 3 options for the results of quality assessment are as follows: “Yes” indicates a low risk of bias, “Unclear” indicates a moderate risk of bias, and “No” indicates a high risk of bias.
Statistics
Wherever appropriate, the data from the studies were pooled together using Comprehensive Meta-analysis (Biostat Inc., Englewood, New Jersey). Statistical heterogeneity was assessed using I-square statistics. We chose to compare categorical variable data using risk ratio (RR) and continuous variable data using weighed mean difference (WMD) as summary statistic with corresponding 95% confidence intervals (CIs). The results were pooled using fixed-effects model (Mantel-Haenszel test); but when there was significant heterogeneity in results between studies (I2 > 50%), a random-effects model was used (DerSimonian-Laird method).
Results
The literature search identified 314 studies, of which 308 were eliminated by screening the title, reading the abstract, or reading the entire article (Figure 1). 2 comparative studies were excluded from this systematic review because both female and male patients were recruited for evaluation (Clarke and Hentz 2008, Tanavalee et al. 2011). Another comparative study was also excluded due to non-randomized treatment allocation (Lionberger et al. 2012). A prospective study was excluded because it reported intraoperative ROM, not postoperative outcomes (Song et al. 2012b). Finally, 6 RCTs met our eligibility criteria (Kim et al. 2010a, b, Kumar et al. 2012, Singh et al. 2012, Song et al. 2012a, Thomsen et al. 2012). They included 846 knees, in which 423 female patients had simultaneous bilateral TKA with a gender-specific prosthesis in one knee and a standard unisex prosthesis in the contralateral knee. The sample size of the data ranged from 48 to 276 cases with an average age of 64–71 years and a mean follow-up time of 2.1–3.2 years. Of the 6 studies, 3 specifically stated that there had been no financial support from a sponsoring medical company (Kim et al. 2010a, b, Thomsen et al. 2012) and the other 3 did mention whether support had been received (Kumar et al. 2012, Singh et al. 2012, Song et al. 2012a). Of the 6 studies, 3 were conducted in Korea (Kim et al. 2010a, b, Song et al. 2012a), 2 in India (Kumar et al. 2012, Singh et al. 2012), and one in Denmark (Thomsen et al. 2012). 5 papers did not describe the randomization procedures in an adequate way; only 1 study was randomized based on a computer-generated list (Tables 1 and 2).
Figure 1.

Flow diagram of selection process.
Table 1.
Study characteristics
| A | B | C | D | E | F | G | H | I | J | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| a | b | a | b | a | b | |||||||
| Singh (2012) India | 100 | 200 | 100 | 100 | 64 (3) | 68 (6) | 31 (4.9) | 31 (5.3) | GS LPS | LPS-Flex | ROM, KSS,HSS, Pain, Complication | 2.1 (1.6–2.5) |
| Thomsen (2012) Denmark | 24 | 48 | 24 | 24 | 66(49–85) | 2 | 9 (23–42) | GS LPS-Flex | LPS-Flex | ROM, Pain, Satisfaction, Complications Daily well-being, Gait analysis, Radiographic outcomes | 1 | |
| Kim (2012a) | 85 | 170 | 85 | 85 | 70 (7) | 27 (18–39) | GS LPS-Flex | LPS-Flex | ROM, KSS, WOMAC, Pain, Satisfaction, Korea HSS, Preference, Complications, Radiographic outcomes Blood loss | 2.1 (2–2.3) | ||
| Kim (2012b) Korea | 138 | 276 | 138 | 138 | 71 (51–82) | 27.3 (20–34) | GS CR-Flex | CR -Flex | ROM, KSS, WOMAC, Pain, Satisfaction, Preference, Complications, Radiographic outcomes, Blood loss | 3.3 (3.1–3.5) | ||
| Song (2012a) Korea | 46 | 92 | 46 | 46 | 69 (53–82) | 27 (20–31) | GS CR-Flex | CR-Flex | ROM, WOMAC, HSS, Preference, Radiographic outcomes | 2.7 (2–3) | ||
| Kumar (2012) India | 30 | 60 | 30 | 30 | 64 (49–76) | NR | GS CR-Flex | CR -Flex | KSS, HSS, Satisfaction, Radiographic outcomes | 2.5 (2–3.8) | ||
A Author, year, country
B No of patients
C No of knees
D No of gender-specific (GS) total knee arthroplasties
E No of control total knee arthroplasties
F Mean age (SD) or (range)
a GS
b Control
G Mean body mass index (SD) or (range)
a GS
b Control
H Type of prosthesis
a GS
b Control
CR: posterior cruciate-retaining
PS: posterior stabilized
LPS: NexGen Legacy Posterior Stabilized
I Outcome and measures
KSS: Knee Society Score
ROM: range of motion
WOMAC: Western Ontario and McMaster Universities osteoarthritis index
J Follow-up, years
Table 2.
Methodological quality of the studies included
| A | B | C | D | E | F | G | H | I | |
|---|---|---|---|---|---|---|---|---|---|
| a | b | ||||||||
| Singh et al. (2012) | Unclear | Unclear | Unclear | Unclear | Yes | Yes | Yes | No | 0 |
| Thomsen et al. (2012) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 4 |
| Song et al. (2012a) | Unclear | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | 3 |
| Kim et al. (2010a) | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 2 |
| Kim et al. (2010b) | Unclear | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 5 |
A Author
B Adequate sequence generation
C Allocation concealment
D Binding
a Patient
b Assessor
E Baseline comparability
F Inclusion /exclusion criteria
G Similarity of postoperative program
H Sample size calculation
I Loss to follow-up
Range of motion
5 articles reported the active ROM of the knee in the supine position (Kim et al. 2010a, b, Singh et al. 2012, Song et al. 2012a, Thomsen et al. 2012), and only 3 studies provided the active ROM outcome in the weight-wearing position (Kim et al. 2010a, b, Song et al. 2012a). Data pooled with a fixed-effects model showed no statistically significant differences in the active ROM under weight-bearing conditions between the gender-specific and unisex groups (WMD = 0.66, CI: –2.0 to 3.4; p = 0.6). Under non-weight-bearing conditions, the gender-specific knee prostheses did not offer a statistically significant advantage in increasing ROM (WMD = 0.57, CI: –2.4 to 3.5; p = 0.7).
Clinical knee scores
The KSS was used in 4 RCTs (Kim et al.2010a, b, Kumar et al. 2012, Singh et al. 2012), the HSS was used in 4 (Kim et al. 2010a, b, Kumar et al. 2012, Singh et al. 2012), and the WOMAC was used in 3 (Kim et al. 2010a, b, Song et al. 2012a). The KSS was similar between the 2 groups (WMD = –0.45, CI: –1.5 to 0.55; p = 0.4). For the WOMAC score at the final follow-up, the WMD was –0.94 (CI: –3.1 to 1.2; p = 0.4), with little between-study heterogeneity (p = 0.8, I2 = 12%). For the studies reporting the HSS at the final follow-up, the WMD was 0.11 (CI: –1.3 to 1.5; p = 0.9), with little between-study heterogeneity (p = 0.8; I2 = 0%).
Participant preference and satisfaction
Of the 323 patients who had bilateral TKAs with different types of prosthesis (gender-specific or unisex), 273 patients (3 trials) reported on preference (Kim et al. 2010a, b, Song et al. 2012a). 216 patients (79%) had no preference, 27 (10%) preferred the standard prosthesis and 30 (11%) the gender-specific prosthesis. Although more patients preferred the gender-specific prostheses to the unisex prostheses, meta-analysis of these trials did not show any statistically significant difference between the numbers of the patients who preferred one or other type of prosthesis (RR = 1.1, CI: 0.68–1.8; p = 0.7).
Of the 6 bilateral trials, participant satisfaction using a visual analog scale (VAS) questionnaire in bilateral cases was documented in 3 (Kim et al. 2010a, b, Thomsen et al. 2012), involving 247 patients. The mean satisfaction score was similar in both groups (WMD = 0.04, CI: –0.52 to 0.60; p = 0.9). In 1 trial (Kumar et al. 2012), 30 patients reported their overall satisfaction after surgery using the British Orthopaedic Association (BOA) patient satisfaction score. The authors found that there were no statistically significant differences in BOA score between the 2 groups at either of 2 follow-up periods.
Pain
Of the 6 studies, 5 provided data on postoperative pain. 11% (49/446) of the gender-specific knees gave pain, the same proportion (48/446) as in the unisex knees. A visual analog scale (VAS) was used to assess postoperative pain in the study by Thomsen et al. (2012), who found no statistically significant differences between the 2 prosthetic designs at 3 and 12 months postoperatively. 3 of the studies included adopted the KSS and HSS subscales for knee pain (Kim et al. 2010a, b, Singh et al. 2012). At the time of the latest follow-up, the pain scores were similar in both the standard and gender-specific groups.
Fit of the femoral component
Meta-analysis of 4 trials revealed that the gender-specific femoral component did not fit better than the standard femoral component (Kim et al. 2010a, b, Kumar et al. 2012, Thomsen et al. 2012) (RR = 0.45, CI: 0.36–0.56; p < 0.001). Specifically, in the female patients with the unisex prosthesis, the femoral prosthesis was closely matched in 172 knees (56%), overhung in 41 (13%), and undercovered the bone in 94 (31%). In the female patients with the gender-specific prosthesis, 77 knees (25%) had a close fit and 230 knees (75%) had undercoverage.
Complications
Postoperative complications and adverse events were reported in 4 trials (Kim et al. 2010a, b, Singh et al. 2012, Thomsen et al. 2012), but these studies did not document any adverse events related to the knee prostheses. The complication rates were low, and they were comparable in both groups (RR = 1.0, CI: 0.42–2.3; p = 1.0, I2 = 0%) (Figure 2).
Figure 2.
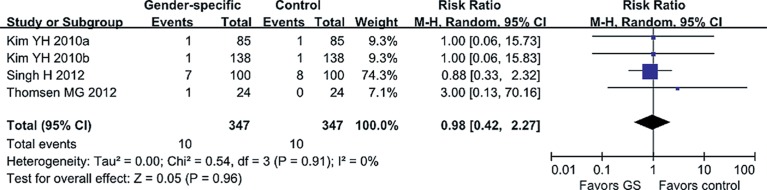
Comparison of the effects of gender-specific prosthesis and standard design on complications after surgery.( ) The weighting given to the trial in the overall pooled estimate, taking into account the number of participants and the amount of between-study variation (heterogeneity). (
) The weighting given to the trial in the overall pooled estimate, taking into account the number of participants and the amount of between-study variation (heterogeneity). ( ) The combined effect size.
) The combined effect size.
Radiographic findings
Of the 6 articles, 5 mentioned radiographic results (Kim et al. 2010a, b, Kumar et al. 2012, Song et al. 2012a, Thomsen et al. 2012). There were no statistically significant differences between the groups regarding radiographic parameters including alignment of the limb (femoro-tibial angle), component positioning, cover of the tibial surface, the level of the joint line, anterior and posterior condylar offset, and patellar tilt angle. None of the knees in either group had a complete radiolucent line wider than 1 mm around any component (Kim et al. 2010a, b, Kumar et al. 2012).
Discussion
We found that the gender-specific design did not provide any clinical advantages over the standard unisex design in the female knee with respect to knee scores, patient preferences, patient satisfaction, and radiographic outcomes.
The strengths of meta-analysis study lie in the large sample size and the inclusion of only RCTs (level I or II evidence). Of the 6 eligible trials, 5 performed simultaneous bilateral TKAs, which allowed comparisons of clinical and radiographic outcomes, satisfaction, and preference in the same patients and detection of subtle differences in prosthesis performance. This method has the advantage that it minimizes potential bias introduced by preoperative patient-related factors such as age, body weight, and pain threshold.
Our study had several potential weaknesses. Firstly, the follow-up period was short. Secondly, our data pertain only to a single implant system (Zimmer Gender Solutions Knee). Additional studies of the femoral prosthesis in other knee systems are needed before our conclusions can be applied to other designs. Thirdly, there is considerable anatomical variation in the knee among different ethnic groups. In our study, 190 of 423 patients (45%) were from the Asian population, whose knees have generally smaller anthropometric measurements than those of Caucasians (Vaidya et al. 2000, Urabe et al. 2008, Chaichankul et al. 2011, Yue et al. 2011a). They require a smaller range of component sizes in TKAs. Thus, the ethnic differences in anthropometric measurements may limit the generalizability of our results to western populations.
The need for gender-specific knee arthroplasties is based on the following assumptions: (1) women have results that are inferior to those of men after TKA, and (2) traditional prosthesis designs have failed to address these differences. A number of clinical studies have refuted the idea that women have worse outcomes than men using traditional total knee designs (MacDonald et al. 2008, Merchant et al. 2008, Ritter et al. 2008, Dalury et al. 2009, Johnson et al. 2011). In fact, some studies have found that women achieve essentially the same results as men, or even better (Merchant et al. 2008, Parsley et al. 2010, O’Connor 2011). A systematic review by Merchant et al. (2008) found no evidence for anatomical differences between men’s and women’s knees that would justify a female-specific design. The average anatomical differences between male and female knees can be explained by the smaller height and size of women on average, not by their gender (Merchant et al. 2008). A recent study showed that the shape of the knee is not only dependent on gender, but also on the morphotype of the patient (Bellemans et al. 2010). Prosthesis design should take inter-individual variations in knee joint anatomy into account (Dargel et al. 2011, Gillespie et al. 2011). However, these anatomical differences may be so small that have no clinical effect, which would agree with the findings of the present study.
Tanavalee et al. (2011) intraoperatively evaluated the overhang of the cutting block on the posteromedial edge of the femoral condyle. They found that the overall percentage of gender-specific prosthesis selection was higher in female patients than in male patients. This phenomenon frequently occurs in medium-sized to large-sized female patients. The medial or lateral overhang of unisex prostheses was worse in female knees than in male knees (Clarke and Hentz 2008, Guy et al. 2012). Yan et al. (2012) reported a higher prevalence of prosthetic overhang in women with standard unisex knee prostheses. Consistent with these findings, our meta-analysis showed that gender-specific design reduced medial or lateral overhang in female patients whereas there was a higher prevalence of underhang than with unisex prostheses. Although a previous study confirmed that femoral component overhang may create postoperative pain due to soft tissue irritation and soft tissue imbalance (Mahoney and Kinsey 2010), our results suggest that the difference in condylar cover does not affect pain scores and knee function. Based on these contradictory results, the question remains whether the modifications made to the gender-specific design are extensive enough to closely match femoral anatomy in female patients and offer any clinical advantages. Notably, the higher incidence of underhang in the gender-specific group, which exposed more cancellous bone than with the NexGen standard prostheses, could be a source of higher perioperative blood loss and may induce increased ostolysis from wear debris with longer follow-up (Hitt et al. 2003, Kim et al. 2010 a, b).
Overstuffing of the patellofemoral compartment may be associated with pain and reduced ROM. The use of a standard TKA could possibly lead to overstuffing because of a less prominent anterior condyle in the female knee. Despite the fact that reduced height of the anterior flange and the deeper trochlear groove would help to prevent overstuffing of the patellofemoral joint and improve patellar tracking in the gender-specific design, we found similar postoperative pain and ROM when comparing the 2 knee prostheses.
Improvement in clinical outcomes following knee arthroplasty is usually measured by score scales, which are associated with a ceiling effect and poor ability to discriminate between high-functioning arthroplasty patients (Senden et al. 2011, Na et al. 2012). More sensitive outcome scores are needed. Gait analysis could provide more objective parameters, such as measurements of sagittal plane kinematics and kinetics (Börjesson et al. 2005, Catani et al. 2012).
A recent gait analysis study suggested that there was no difference between the 2 knee prosthesis designs in terms of kinematic, kinetic, and temporo-spatial parameters (Thomsen et al. 2012). Given the inadequate correlations between knee scores and gait parameters, further gait analysis studies monitoring the functional benefit of design in TKAs are needed (Liebensteiner et al. 2008).
In conclusion, gender-specific changes to knee prostheses do not translate into improved outcomes. Furthermore, gender-specific protheses would not necessarily fit any better than unisex designs.
Acknowledgments
TC, QW, and XZ conceived and designed the study. TC, CZ, MC, and JW extracted and analyzed the data. TC, CZ, and XP wrote the paper.
No competing interests declared.
This work was supported by the fund of the National Natural Science Foundation of China (81301571).
References
- Börjesson M, Weidenhielm L, Mattsson E, Olsson E. Gait and clinical measurements in patients with knee osteoarthritis after surgery: a prospective 5-year follow-up study . Knee. 2005;12(2):121–7. doi: 10.1016/j.knee.2004.04.002. [DOI] [PubMed] [Google Scholar]
- Bellemans J, Carpentier K, Vandenneucker H, Vanlauwe J, Victor J. Both morphotype and gender influence the shape of the knee in patients undergoing TKA . Clin Orthop. 2010;468(1):29–36. doi: 10.1007/s11999-009-1016-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catani F, Benedetti MG, Bianchi L, Marchionni V, Giannini S, Leardini A. Muscle activity around the knee and gait performance in unicompartmental knee arthroplasty patients: a comparative study on fixed- and mobile-bearing designs . Knee Surg Sports Traumatol Arthrosc. 2012;20(6):1042–8. doi: 10.1007/s00167-011-1620-z. [DOI] [PubMed] [Google Scholar]
- Chaichankul C, Tanavalee A, Itiravivong P. Anthropometric measurements of knee joints in Thai population: correlation to the sizing of current knee prostheses . Knee. 2011;18(1):5–10. doi: 10.1016/j.knee.2009.12.005. [DOI] [PubMed] [Google Scholar]
- Chin KR, Dalury DF, Zurakowski D, Scott RD. Intraoperative measurements of male and female distal femurs during primary total knee arthroplasty . J Knee Surg. 2002;15(4):213–7. [PubMed] [Google Scholar]
- Clarke HD, Hentz JG. Restoration of femoral anatomy in TKA with unisex and gender-specific components . Clin Orthop. 2008;466(11):2711–6. doi: 10.1007/s11999-008-0454-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conley S, Rosenberg A, Crowninshield R. The female knee: anatomic variations . J Am Acad Orthop Surg (Suppl 1) 2007;15:S31–6. doi: 10.5435/00124635-200700001-00009. [DOI] [PubMed] [Google Scholar]
- Dalury DF, Mason JB, Murphy JA, Adams MJ. Analysis of the outcome in male and female patients using a unisex total knee replacement system . J Bone Joint Surg (Br) 2009;91(3):357–60. doi: 10.1302/0301-620X.91B3.21771. [DOI] [PubMed] [Google Scholar]
- Dargel J, Michael JW, Feiser J, Ivo R, Koebke J. Human knee joint anatomy revisited: morphometry in the light of sex-specific total knee arthroplasty . J Arthroplasty. 2011;26(3):346–53. doi: 10.1016/j.arth.2009.12.019. [DOI] [PubMed] [Google Scholar]
- Fehring TK, Odum SM, Hughes J, Springer BD, Beaver W B. Jr. Differences between the sexes in the anatomy of the anterior condyle of the knee . J Bone Joint Surg (Am) 2009;91(10):2335–41. doi: 10.2106/JBJS.H.00834. [DOI] [PubMed] [Google Scholar]
- Gillespie RJ, Levine A, Fitzgerald SJ, Kolaczko J, DeMaio M, Marcus RE, Cooperman DR. Gender differences in the anatomy of the distal femur . J Bone Joint Surg (Br) 2011;93(3):357–63. doi: 10.1302/0301-620X.93B3.24708. [DOI] [PubMed] [Google Scholar]
- Guy SP, Farndon MA, Sidhom S, Al-Lami M, Bennett C, London NJ. Gender differences in distal femoral morphology and the role of gender specific implants in total knee replacement: a prospective clinical study . Knee. 2012;19(1):28–31. doi: 10.1016/j.knee.2010.12.005. [DOI] [PubMed] [Google Scholar]
- Hitt K, Shurman J R, 2nd, Greene K, McCarthy J, Moskal J, Hoeman T, Mont MA. Anthropometric measurements of the human knee: correlation to the sizing of current knee arthroplasty systems . J Bone Joint Surg (Am) (Suppl 4) 2003;85:115–22. [PubMed] [Google Scholar]
- Hsu RW, Himeno S, Coventry MB, Chao EY. Normal axial alignment of the lower extremity and load-bearing distribution at the knee . Clin Orthop. 1990;255:215–27. [PubMed] [Google Scholar]
- Johnson AJ, Costa CR, Mont MA. Do we need gender-specific total joint arthroplasty? . Clin Orthop. 2011;469(7):1852–8. doi: 10.1007/s11999-011-1769-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kamath AF, Horneff JG, Gaffney V, Israelite CL, Nelson CL. Ethnic and gender differences in the functional disparities after primary total knee arthroplasty . Clin Orthop. 2010;468(12):3355–61. doi: 10.1007/s11999-010-1461-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim YH, Choi Y, Kim JS. Comparison of a standard and a gender-specific posterior cruciate-substituting high-flexion knee prosthesis: a prospective, randomized, short-term outcome study . J Bone Joint Surg (Am) 2010a;92(10):1911–20. doi: 10.2106/JBJS.I.00910. [DOI] [PubMed] [Google Scholar]
- Kim YH, Choi Y, Kim JS. Comparison of standard and gender-specific posterior-cruciate-retaining high-flexion total knee replacements: a prospective, randomised study . J Bone Joint Surg (Br) 2010b;92(5):639–645. doi: 10.1302/0301-620X.92B5.24129. [DOI] [PubMed] [Google Scholar]
- Kumar V, Bhavuk G, Malhotra R. A randomized trial comparing gender specific with gender non-specific knee arthroplasty implants. J Bone Joint Surg (Br) (Suppl XXXVII) 2012;94:525. [Google Scholar]
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from . J Bone Joint Surg (Am) 2005;2007;89(4):780–5. doi: 10.2106/JBJS.F.00222. [DOI] [PubMed] [Google Scholar]
- Liebensteiner MC, Herten A, Gstoettner M, Thaler M, Krismer M, Bach CM. Correlation between objective gait parameters and subjective score measurements before and after total knee arthroplasty . Knee. 2008;15(6):461–6. doi: 10.1016/j.knee.2008.07.001. [DOI] [PubMed] [Google Scholar]
- Lionberger DR, Eggers MD, Brewer KE, Fang L. Improved knee flexion following high-flexion total knee arthroplasty . J Orthop Surg Res. 2012;7(22):22. doi: 10.1186/1749-799X-7-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lo CS, Wang SJ, Wu SS. Knee stiffness on extension caused by an oversized femoral component after total knee arthroplasty: a report of two cases and a review of the literature . J Arthroplasty. 2003;18(6):804–8. doi: 10.1016/s0883-5403(03)00331-0. [DOI] [PubMed] [Google Scholar]
- MacDonald SJ, Charron KD, Bourne RB, Naudie DD, McCalden RW, Rorabeck CH. Gender-specific total knee replacement: prospectively collected clinical outcomes. Clin Orthop. 2008;466(11):2612–6. doi: 10.1007/s11999-008-0430-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahoney OM, Kinsey T. Overhang of the femoral component in total knee arthroplasty: risk factors and clinical consequences . J Bone Joint Surg (Am) 2010;92(5):115–21. doi: 10.2106/JBJS.H.00434. [DOI] [PubMed] [Google Scholar]
- Merchant AC, Arendt EA, Dye SF, Fredericson M, Grelsamer RP, Leadbetter WB, Post WR, Teitge RA. The female knee: anatomic variations and the female-specific total knee design. Clin Orthop. 2008;466(12):3059–65. doi: 10.1007/s11999-008-0536-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Na SE, Ha CW, Lee CH. A new high-flexion knee scoring system to eliminate the ceiling effect . Clin Orthop. 2012;470(2):584–93. doi: 10.1007/s11999-011-2203-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Connor MI. Implant survival, knee function, and pain relief after TKA: are there differences between men and women?” . Clin Orthop. 2011;469(7):1846–51. doi: 10.1007/s11999-011-1782-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parratte S, Argenson JN, Since M, Pierre P BP, Pauly V, Aubaniac JM. Does gender specific implant improve function and patient satisfaction in total knee arthroplasty? J Bone Joint Surg (Br) (Suppl II) (supp II) 2011;93:93. [Google Scholar]
- Parsley BS, Bertolusso R, Harrington M, Brekke A, Noble PC. Influence of gender on age of treatment with TKA and functional outcome . Clin Orthop. 2010;468(7):1759–64. doi: 10.1007/s11999-010-1348-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ritter MA, Wing JT, Berend ME, Davis KE, Meding JB. The clinical effect of gender on outcome of total knee arthroplasty . J Arthroplasty. 2008;23(3):331–6. doi: 10.1016/j.arth.2007.10.031. [DOI] [PubMed] [Google Scholar]
- Senden R, Grimm B, Meijer K, Savelberg H, Heyligers IC. The importance to including objective functional outcomes in the clinical follow up of total knee arthroplasty patients . Knee. 2011;18(5):306–11. doi: 10.1016/j.knee.2010.07.008. [DOI] [PubMed] [Google Scholar]
- Singh H, Mittal V, Nadkarni B, Agarwal S, Gulati D. Gender-specific high-flexion knee prosthesis in Indian women: a prospective randomised study . J Orthop Surg (Hong Kong) 2012;20(2):153–6. doi: 10.1177/230949901202000203. [DOI] [PubMed] [Google Scholar]
- Song EK, Jung WB, Yoon TR, Park KS, Seo HY, Seon JK. Comparison of outcomes after bilateral simultaneous total knee arthroplasty using gender-specific and unisex knees . J Arthroplasty. 2012a;27(2):226–31. doi: 10.1016/j.arth.2011.03.046. [DOI] [PubMed] [Google Scholar]
- Song EK, Park SJ, Yoon TR, Park KS, Seo HY, Seon JK. Hi-flexion and gender-specific designs fail to provide significant increases in range of motion during cruciate-retaining total knee arthroplasty . J Arthroplasty. 2012b;27(6):1081–4. doi: 10.1016/j.arth.2011.10.011. [DOI] [PubMed] [Google Scholar]
- Tanavalee A, Rojpornpradit T, Khumrak S, Ngarmukos S. The early results of gender-specific total knee arthroplasty in Thai patients . Knee. 2011;18(6):483–7. doi: 10.1016/j.knee.2010.10.005. [DOI] [PubMed] [Google Scholar]
- Thomsen MG, Husted H, Bencke J, Curtis D, Holm G, Troelsen A. Do we need a gender-specific total knee replacement? A randomised controlled trial comparing a high-flex and a gender-specific posterior design . J Bone Joint Surg (Br) 2012;94(6):787–92. doi: 10.1302/0301-620X.94B6.28781. [DOI] [PubMed] [Google Scholar]
- Urabe K, Mahoney OM, Mabuchi K, Itoman M. Morphologic differences of the distal femur between Caucasian and Japanese women . J Orthop Surg (Hong Kong) 2008;16(3):312–5. doi: 10.1177/230949900801600309. [DOI] [PubMed] [Google Scholar]
- Vaidya SV, Ranawat CS, Aroojis A, Laud NS. Anthropometric measurements to design total knee prostheses for the Indian population . J Arthroplasty. 2000;15(1):79–85. doi: 10.1016/s0883-5403(00)91285-3. [DOI] [PubMed] [Google Scholar]
- Vincent KR, Vincent HK, Lee LW, Alfano AP. Outcomes in total knee arthroplasty patients after inpatient rehabilitation: influence of age and gender . Am J Phys Med Rehabil. 2006;85(6):482–9. doi: 10.1097/01.phm.0000219151.18749.50. [DOI] [PubMed] [Google Scholar]
- von Roth P, Matziolis G, Pfitzner T, Mayr HO, Klein T, Preininger B, Winkler T, Hube R. Early results of gender-specific posterior stabilized total knee arthroplasty without patella resurfacing . Orthopade. 2013;42(10):866–73. doi: 10.1007/s00132-013-2139-4. [DOI] [PubMed] [Google Scholar]
- Woodland LH, Francis RS. Parameters and comparisons of the quadriceps angle of college-aged men and women in the supine and standing positions . Am J Sports Med. 1992;20(2):208–11. doi: 10.1177/036354659202000220. [DOI] [PubMed] [Google Scholar]
- Yan M, Wang J, Wang Y, Zhang J, Yue B, Zeng Y. Gender-based differences in the dimensions of the femoral trochlea and condyles in the Chinese population: Correlation to the risk of femoral component overhang . Knee. 2014;21(1)(2):52–6. doi: 10.1016/j.knee.2012.11.005. [DOI] [PubMed] [Google Scholar]
- Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li G. Differences of knee anthropometry between Chinese and white men and women . J Arthroplasty. 2011a;26(1):124–30. doi: 10.1016/j.arth.2009.11.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li G. Gender differences in the knees of Chinese population . Knee Surg Sports Traumatol Arthrosc. 2011b;19(1):80–8. doi: 10.1007/s00167-010-1139-8. [DOI] [PubMed] [Google Scholar]
- Yue B, Wang J, Wang Y, Yan M, Zhang J, Zeng Y. How the gender or morphological specific TKA prosthesis improves the component fit in the Chinese population? . J Arthroplasty. 2014;29(1):71–4. doi: 10.1016/j.arth.2013.04.038. [DOI] [PubMed] [Google Scholar]
- Zeng YM, Wang Y, Zhu ZA, Dai KR. Effects of sex and lower extremity alignment on orientation of the knee joint line in knee surgery . Chin Med J (Engl) 2012;125(12):2126–31. [PubMed] [Google Scholar]