

Abstract
Objective
To evaluate the prevalence of known risk factors for contrast-induced nephropathy (CIN) and their association with the actual occurrence of CIN in patients undergoing intravenous contrast-enhanced computed tomography (CECT) in Korea.
Materials and Methods
Patients who underwent CECT in 2008 were identified in the electronic medical records of 16 tertiary hospitals of Korea. Data on demographics, comorbidities, prescriptions and laboratory test results of patients were collected following a standard data extraction protocol. The baseline renal function was assessed using the estimated glomerular filtration rate (eGFR). We identified the prevalence of risk factors along the eGFR strata and evaluated their influence on the incidence of CIN, defined as a 0.5 mg/dL or 25% increase in serum creatinine after CECT.
Results
Of 432425 CECT examinations in 272136 patients, 140838 examinations in 101487 patients met the eligibility criteria for analysis. The mean age of the participants was 57.9 ± 15.5 years; 25.1% of the patients were older than 70 years. The prevalence of diabetes mellitus was 11.9%, of hypertension 13.7%, of gout 0.55% and of heart failure was 1.7%. Preventive measures were used in 40238 CECT examinations (28.6%). The prevalence of risk factors and use of preventive measures increased as the renal function became worse. A CIN was occurred after 3103 (2.2%) CECT examinations, revealing a significant association with decreased eGFR, diabetes mellitus, and congestive heart failure after adjustment.
Conclusion
Risk factors for CIN are prevalent among the patients undergoing CECT. Preventive measures were seemingly underutilized and a system is needed to improve preventive care.
Keywords: Contrast-induced nephropathy, Contrast-enhanced computed tomography, Prevalence, Risk factor
INTRODUCTION
An intravenous administration of iodinated contrast media during contrast-enhanced computed tomography (CECT) can lead to contrast-induced nephropathy (CIN) (1), which is known to increase the length of hospital stay, costs of medical care and the risk of permanent renal impairment (2, 3). Although serious clinical outcomes after CIN have been reported to be rare (4, 5, 6, 7), efforts to reduce CIN caused by CECT are worthwhile (5, 6).
Current guidelines for CIN recommend a pre-contrast assessment of patients to identify risk factors such as impaired renal function, diabetes mellitus (DM) and congestive heart failure (CHF) in order to prompt appropriate actions including measurement of the serum creatinine (SCr) and adequate hydration for high risk patients (4, 8). However, a gap between the evidence-based guidelines and the daily practice of radiologists for CIN prevention in CECT patients has been identified (9), which is likely due to the logistics needed to enable SCr measurement, intravenous hydration and serial follow-up of SCr in the setting of a radiology department (10). The first step should be to measure the size of the population who are at risk of CIN, which would depend on the prevalence of the major risk factors to develop a feasible protocol for the prevention of CIN by CECT. Accordingly, the prevalence data on risk factors of CIN in patients undergoing CECT are essential for designing a control strategy of CIN. Thus far, such data have been collected mostly at a single institution. For this reason, we conducted a multi-center observational study to evaluate the prevalence of known risk factors for CIN and their association with the actual incidence of CIN in patients undergoing CECT in Korea.
MATERIALS AND METHODS
Data Collection
The study was compliant with the Personal Information Protection Act of the Republic of Korea. The study protocol was reviewed and approved by the Institutional Review Boards of each participating hospital with a waiver for informed consents of study participants.
Radiology departments of 16 tertiary hospitals in Korea participated in this study. We developed a method to extract data on CECT, pre-CT medication use, comorbidities and laboratory tests from the electronic medical records (EMRs) or computerized provider order entry (CPOE) systems of participating hospitals in a standardized format, using the codes originally to be used in the Korean National Health Insurance (KNHI) for a reimbursement claim. KNHI has been covering the entire Korean population since 1999. Out of the 16 participating centers in this study, 13 hospitals were using EMR in 2008, which reflects a higher adoption rate of EMR systems than those of other countries (11). Although not all hospitals were using comprehensive EMR systems, all participating centers were using electronic communication systems for medications, laboratory tests, diagnostic codes and CECTs. Physicians usually entered the diagnosis and prescription into the system by themselves during that period of time.
We retrospectively identified all patients undergoing CECT with intravenous iodinated contrast media in 2008 by accessing the EMRs or CPOEs of the participating hospitals. The collected variables included the age (with ages 70 years or older being categorized as advanced age) and sex of the patients, SCr level and diagnostic information on DM, CHF, gout and hypertension (HT). We also extracted prescription information of the patients to determine whether they took potential nephrotoxic medications including non-steroid anti-inflammatory drugs (NSAIDs), diuretics, angiotensin converting enzyme inhibitors (ACEIs), and angiotensin receptor blockers (ARBs) on the day of CECT and whether they received normal saline (NS) ≥ 500 mL, N-acetylcysteine (NAC) and sodium bicarbonate within 1 day prior to CECT as protective measures for CIN.
The extracted data were transmitted to the coordinating center for further data management and analysis after encryption according to the Electronic Communication Fundamental Law of Korea. Of 432425 CECT examinations performed in 272136 patients at the 16 participating hospitals in 2008, patients who were older than 15 years, who had at least 1 SCr test within 14 days before CECT and 1 SCr test within 3 days after CECT and whose pre-CECT estimated glomerular filtration rate (eGFR) (see below) was equal to or higher than 15 mL/min/1.73 m2 were selected for analysis. A total of 140838 CECT examinations performed in 101487 patients were included for analysis (Fig. 1).
Fig. 1.

Flow diagram of patient selection. CECT = contrast-enhanced computed tomography, eGFR = estimated glomerular filtration rate
As the eGFR can identify more patients with renal insufficiency than SCr (12), we calculated the eGFR of the pre-CECT state in each patient with the 4-variable Modification of Diet in Renal Diseases formula (13):
| eGFR (mL/min/1.73 m2) = 186 × (SCr)-1.154 × (age)-0.203 × (0.742 if female) × (1.212 if black) |
We found that 2 hospitals had used the isotope dilution mass spectrometry traceable SCr assay during the study period; we thus used the following formula for the 2 hospitals considering the utilization of standardized SCr assay:
| eGFR (mL/min/1.73 m2) = 175 × (standardized SCr)-1.154 × (age)-0.203 × (0.742 if female) × (1.212 if black) |
Based on the calculated eGFR prior to the CECT, we categorized the baseline renal function into 4 categories: eGFR ≥ 60 mL/min/1.73 m2, 45-59 mL/min/1.73 m2, 30-44 mL/min/1.73 m2, and 15-29 mL/min/1.73 m2.
Statistical Analysis
We appropriately presented the mean age ± standard deviation and the distribution of risk factors for CIN in frequency for the entire dataset and according to the eGFR strata with 95% confidence intervals (CIs). The rate of preventive measures use was described, categorized into either when NS (with our without combination with other agents) was used or when it was not used.
The eGRF was dichotomized by the value of 45 mL/min/1.73 m2 to analyze the association of the risk factors with the actual incidence of CIN (4). The most recent SCr within the 14 days before each CECT was used as the baseline. The highest SCr within the 3 days after the CECT was used as the follow-up SCr to determine the incidence of CIN. We calculated the difference between the follow-up and baseline SCr and CIN was defined as an increase of 0.5 mg/dL or 25% increase from the baseline (14). We described the characteristics of the CIN group versus the non-CIN group, showing the relative risk for CIN by each risk factor using the generalized estimating equations, which was the appropriate statistical model for our data which included patients who had undergone multiple CECT procedures. We also analyzed the data with the conditional logistic regression following the propensity score matching to eliminate the indication bias in estimating the effectiveness of preventive measures. After constructing a logistic regression model to calculate the probability of using preventive measures before CECT with the c-statistics of 0.79 we matched 1 non-user to each user according to the probability of using preventive measures such that the difference in the probability was less than 0.00001 within the user/non-user pair using a greedy algorithm. In addition, the incidence of CIN was determined for each risk factor after stratification by the use of preventive measures. All statistical tests were 2-sided and p values < 0.05 were considered statistically significant. The SAS version 9.1 (SAS Institute, Inc., Cary, NC, USA) was used for statistical analysis.
RESULTS
Of 140838 CECT examinations was the baseline eGFR greater than or equal to 60 mL/min/1.73 m2 in 118424 (84.1%), 45-59 mL/min/1.73 m2 in 16630 (11.8%), 30-44 mL/min/1.73 m2 in 4421 (3.1%), and 15-29 mL/min/1.73 m2 in 1363 (1.0%) (Table 1). The prevalence of risk factors showed an increasing tendency as the renal function worsened. However, the proportion of those in advanced age in the group with the worst renal function was smaller than that in the 3rd eGFR group. The mean age of the group with an eGFR of 15-29 mL/min/1.73 m2 was 67.2 (± 13.0), which was smaller than that of the 3rd eGFR group (p < 0.01). The prevalence of risk factors for CIN was 25.1% (95% CI: 24.9-25.3) for the advanced age; 11.9% (11.7-12.1) for DM; 13.7% (13.5-13.8) for HT; 1.7% (1.6-1.8) for CHF; and 0.55% (0.51-0.59) for gout. NSAIDs were prescribed in 25.2% (25.0-25.4), diuretics in 11.6% (11.4-11.7) and ACEI/ARB were prescribed for the day of CECT in 11.8% (11.6-11.9) of cases.
Table 1.
Prevalence of Risk Factors for Contrast Induced Nephropathy in Total of 140838 Contrast Enhanced Computed Tomography Examinations
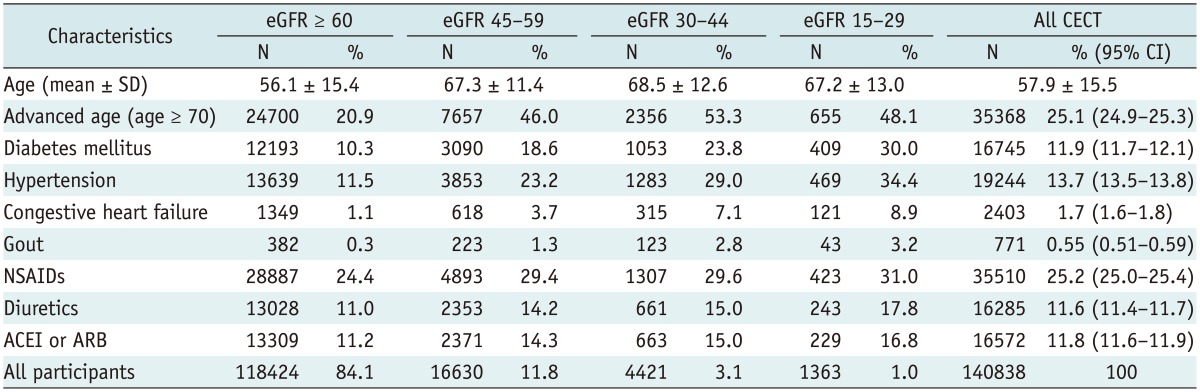
Note.- Estimated glomerular filtration rate (eGFR) was calculated using MDRD formula whose unit was mL/min/1.73 m2. ACEI = angiotensin converting enzyme inhibitor, ARB = angiotensin receptor blocker, CECT = contrast-enhanced computed tomography, CI = confidence interval, MDRD = Modification of Diet in Renal Diseases, NSAIDs = non-steroidal anti-inflammatory drugs, SD = standard deviation
Preventive measures were used in 40238 CECT examinations (28.6%), 37448 (26.6%) of which were NS with or without combination with other agents (Table 2). There was a prominent increase in preventive measures as eGFR dropped below 45 mL/min/1.73 m2, which was mostly attributed to the increased use of other preventive measures than NS.
Table 2.
Use of Preventive Measures
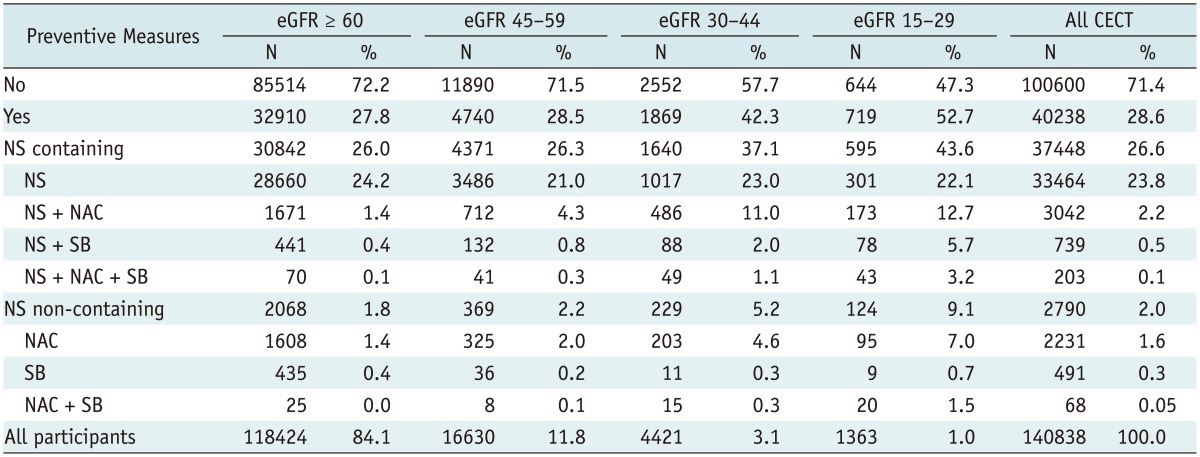
Note.- Estimated glomerular filtration rate (eGFR) was calculated using MDRD formula whose unit was mL/min/1.73 m2. CECT = contrast-enhanced computed tomography, MDRD = Modification of Diet in Renal Diseases, NAC = N-acetylcysteine, NS = normal saline, SB = sodium bicarbonate
We identified 3103 cases of CIN, which accounted for 2.2% of all CECT examinations. All of the risk factors were more prevalent in the CIN group and the difference was statistically significant except for nephrotoxic medications at the univariable analysis (Table 3). In the multivariable analysis, however, decreased eGFR, DM, and CHF only remained statistically significant after the adjustment. The most prominent risk factor was the decreased eGFR with an adjusted relative risk (aRR) of 11.52 (10.43-12.73) for CIN. Gout was with an aRR of 0.78 (0.52-1.18) insignificant after the adjustment. The aRR for advanced age was 0.84 (0.76-0.92). Preventive measures were related to CIN events with an aRR of 2.83 (2.62-3.07). Using the propensity of using preventive measures, we matched the 27369 CECT examinations performed after preventive measures to the same number of CECT examinations performed without preventive measures within the predefined probability difference of using preventive measures. However, the odds ratio (OR) for developing CIN was 2.70 (95% CI: 2.39-3.05) for the group that used preventative measures compared with the cases that did not use preventative measures, similar to the results of the multivariable analysis.
Table 3.
Association of Risk Factors of CIN with Actual Occurrence of CIN
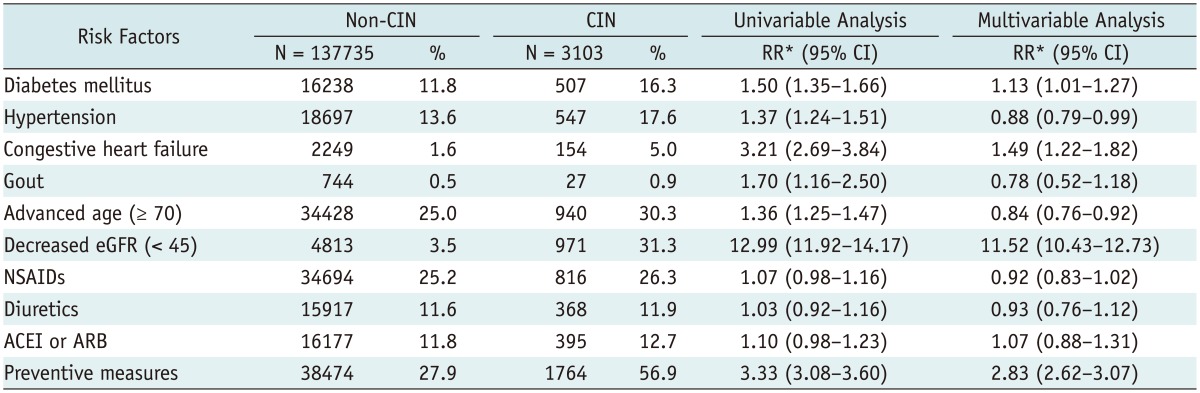
Note.- Estimated glomerular filtration rate (eGFR) was calculated using MDRD formula whose unit was mL/min/1.73 m2. *Estimates were calculated using generalized estimating equations. ACEI = angiotensin converting enzyme inhibitor, ARB = angiotensin receptor blocker, CI = confidence interval, CIN = contrast-induced nephropathy, MDRD = Modification of Diet in Renal Diseases, NSAID = non-steroidal anti-inflammatory drugs, RR = relative risk
When we calculated the incidence rate ratio of CIN for each risk factor group stratified by the use of preventive measures, we uniformly found smaller incidence rate ratios for each significant CIN risk factor in the cases where preventive measures were used than in those cases were no preventative measures were used. The aRR for DM were 1.19 (95% CI: 1.02-1.40), for CHF 1.73 (1.24-2.41) and for decreased eGFR 14.17 (12.21-16.44) in cases without use of preventative measures and 1.07 (0.91-1.26), 1.38 (1.09-1.76), and 9.96 (8.79-11.29), respectively, in cases with use of preventive measures. For the decreased eGFR, the 95% CI of the risk estimates was not overlapping, which suggested a significant decrease in CIN risk by preventive measures.
DISCUSSION
This study analyzed the prevalence of CIN risk factors and their relationship with the actual incidents of CIN using large data obtained from 16 tertiary hospitals in Korea. The incidence of CIN from all CECT procedures included to the analysis was 2.2% which was comparable to that found in previous studies. Balemans et al. (5) reported 23 CIN cases out of 944 procedures (2.43%), without the need for hemodialysis in any of the cases. Katzberg and Lamba (15) reviewed studies including 1075 patients with intravenous contrast media showing a 5.1% incidence of CIN without dialysis or mortality. El-Hajjar et al. (16) presented a very low incidence of CIN: only 4 CINs were reported out of 400 patients who underwent CT angiography with preventive measures. Although the prevalence of risk factors and the use of preventive measures varied among studies, the low incidence of CIN among CECT patients was consistent to previous studies.
A decreased renal function (eGFR < 45 mL/min/1.73 m2) was the most important independent risk factor for the development of CIN, although the aRR was larger than that of the previous studies. We found that DM, CHF and decreased renal function were associated with CIN; however, the age was associated with a decrease in the CIN. Many studies reported age as an independent risk factor of CIN (17, 18, 19). As we mentioned in the results section, the mean age of the group with an eGFR 15-29 mL/min/1.73 m2 was 67.2 years (± 13.0), which was smaller than that in the eGFR 30-44 mL/min/1.73 m2 group. Although a strong association between age and the deterioration of renal function has been identified (20), the mean all-cause mortality rate was the highest in elderly patients with low eGFR (21). The age distribution across eGFR groups in our data reflect the low chance of survival of elderly patients with advanced stage of chronic kidney disease. Furthermore, it was obvious that all the other risk factors increased as the patients became older. For those reasons, the incidence of CIN could be explained by the effect of risk factors other than advanced age in a multivariable model.
The adjusted OR was 2.83 (2.62-3.07) for preventive measures. However, it is well known that those treatments have been beneficial in prevention against CIN in patients who underwent a CECT. Like many other observational studies, our study was susceptible to unmeasured confounding. Regarding the results of the multivariable model, we did not attempt to conclude that preventive measures may increase the risk of CIN. This counterintuitive adjusted OR might have resulted from the fact that the preventive measures were likely performed in patients with a higher risk of CIN while some of the risk factors could not be accounted our statistical adjustment. The relevant data available in the medical records of the patients were likely not comprehensive enough to nullify the effect of all the confounders. Similarly, the results from the propensity score matching analysis also suggested that the input variables used to calculate the propensity score were not sufficient enough to properly evaluate the effect of the preventive measures.
Our data clearly showed that the risk factors of CIN were more prevalent in patients with a lower eGFR (Table 1) and that preventive measures became more prevalent as the eGFR decreased (Table 2). Therefore, it was obvious that patients with risk factors of CIN were more likely to have preventive measures referring to this data. We found this tendency consistently in every stratum of CIN risk factors and in the patient subgroup without any risk factors prior to CECT. Weisbord et al. (7) also reported a similar tendency that patients who were hospitalized or had lower baseline eGFR levels were more likely to undergo preventive measures and were seemingly more likely to derive benefit from such care. The hydration (OR 1.6, 95% CI: 0.6-4.1) and NAC (OR 2.4, 95% CI: 1.9-5.8) were associated with CIN when they defined CIN as a 25% increase in SCr.
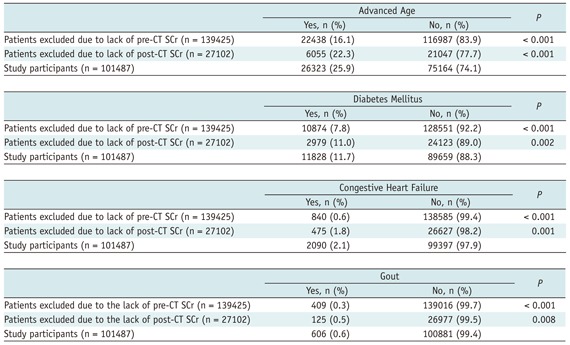
Our results should be interpreted with caution due to several limitations. Although we pooled the electronic data of a very large population, this was not a random sample of the target population; thus we cannot say that it is generalizable to all CECT patients. Carstensen et al. (22) reported a prevalence of renal insufficiency that was very similar to this study. However, the study participants could have had more risk factors than ordinary CECT patients, as we selected patients from tertiary hospitals, which might still result in an over-estimation of the prevalence of risk factors. A large number of patients without SCr checked either before or after CECT were excluded, which could have biased the estimates. We found that the patients excluded from the analysis due to the lack of SCr measurements had significantly low rates of risk factors than those who were analyzed in the study (Appendix). Therefore, the excluded patients may have been less likely to develop CIN than the study participants. Although we could not directly assess the incidence of CIN in the patients who were excluded due to the lack of SCr measurements, the prevalence of risk factors and incidence of CIN might have been over-estimated in our study. Another important aspect of the study population was derived from the fact that we did not exclude patients who were on dialysis, but we excluded patients with an eGFR below 15. Considering that there might have been some patients who were on dialysis with an eGFR of at least 15, this study might have included a small number of dialysis patients. However, it is likely that most of the patients on peritoneal dialysis were excluded, so that only a small proportion of patients on hemodialysis were misclassified into the group of study participants.
The incidence of CIN was not directly compared to the population undergoing non-contrast studies, even though a control group would be essential to elucidate the causal relationship between CECT and CIN. In terms of incidence, the interval for SCr measurements was irregular as the data were collected retrospectively, which could have caused a detection bias to underestimate the CIN incidence. The timing and rate of hydration were not available; thus our operational definition of the use of NS as a preventive measure might have inflated the usage rate of the preventive measures.
Some studies have reported the setting of care as an independent risk factor (7) and have noted a higher incidence of CIN in inpatients. We could not identify any difference in the incidence between the inpatients and outpatients since we did not collect information on the setting of care. For the nephrotoxic medications, the medication use a few days before CECT could have had a similar toxic effect that caused an increase in SCr though we defined the exposure as the prescription for the day of CECT. On the other hand, the physician might have given instructions to skip the medication to the patient on the day of CECT, some of which might have not been precisely noted in the medical records. Finally, the use of any other not prescribed nephrotoxic medication such as herbal medicine, if existed, could not be included in our analysis.
In conclusion, we found that DM, CHF and a decreased eGFR were significantly associated with the occurrence of CIN after CECT in Korea and preventive measures were underutilized. Further efforts are needed to develop a system for the identification of susceptible patients and for the facilitation of preventive measures are needed.
Appendix
Prevalence of Risk Factors for CIN in Patients Who Were Excluded Due to Lack of SCr
Footnotes
This study was funded by the 2010 Korean Society of Radiology-GE Healthcare Research Grant. The funding source did not participate in any steps of the study including planning, data collection, analysis, or interpretation of the data.
References
- 1.Parfrey PS, Griffiths SM, Barrett BJ, Paul MD, Genge M, Withers J, et al. Contrast material-induced renal failure in patients with diabetes mellitus, renal insufficiency, or both. A prospective controlled study. N Engl J Med. 1989;320:143–149. doi: 10.1056/NEJM198901193200303. [DOI] [PubMed] [Google Scholar]
- 2.Solomon R, Barrett B. Follow-up of patients with contrast-induced nephropathy. Kidney Int Suppl. 2006;(100):S46–S50. doi: 10.1038/sj.ki.5000374. [DOI] [PubMed] [Google Scholar]
- 3.Solomon RJ, Mehran R, Natarajan MK, Doucet S, Katholi RE, Staniloae CS, et al. Contrast-induced nephropathy and longterm adverse events: cause and effect? Clin J Am Soc Nephrol. 2009;4:1162–1169. doi: 10.2215/CJN.00550109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stacul F, van der Molen AJ, Reimer P, Webb JA, Thomsen HS, Morcos SK, et al. Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines. Eur Radiol. 2011;21:2527–2541. doi: 10.1007/s00330-011-2225-0. [DOI] [PubMed] [Google Scholar]
- 5.Balemans CE, Reichert LJ, van Schelven BI, van den Brand JA, Wetzels JF. Epidemiology of contrast material-induced nephropathy in the era of hydration. Radiology. 2012;263:706–713. doi: 10.1148/radiol.12111667. [DOI] [PubMed] [Google Scholar]
- 6.Kim SM, Cha RH, Lee JP, Kim DK, Oh KH, Joo KW, et al. Incidence and outcomes of contrast-induced nephropathy after computed tomography in patients with CKD: a quality improvement report. Am J Kidney Dis. 2010;55:1018–1025. doi: 10.1053/j.ajkd.2009.10.057. [DOI] [PubMed] [Google Scholar]
- 7.Weisbord SD, Mor MK, Resnick AL, Hartwig KC, Palevsky PM, Fine MJ. Incidence and outcomes of contrast-induced AKI following computed tomography. Clin J Am Soc Nephrol. 2008;3:1274–1281. doi: 10.2215/CJN.01260308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McCullough PA, Stacul F, Becker CR, Adam A, Lameire N, Tumlin JA, et al. Contrast-Induced Nephropathy (CIN) Consensus Working Panel: executive summary. Rev Cardiovasc Med. 2006;7:177–197. [PubMed] [Google Scholar]
- 9.Fishman EK, Reddan D. What are radiologists doing to prevent contrast-induced nephropathy (CIN) compared with measures supported by current evidence? A survey of European radiologists on CIN associated with computed tomography. Acta Radiol. 2008;49:310–320. doi: 10.1080/02841850701858257. [DOI] [PubMed] [Google Scholar]
- 10.Richenberg J. How to reduce nephropathy following contrast-enhanced CT: a lesson in policy implementation. Clin Radiol. 2012;67:1136–1145. doi: 10.1016/j.crad.2012.05.003. [DOI] [PubMed] [Google Scholar]
- 11.Yoon D, Chang BC, Kang SW, Bae H, Park RW. Adoption of electronic health records in Korean tertiary teaching and general hospitals. Int J Med Inform. 2012;81:196–203. doi: 10.1016/j.ijmedinf.2011.12.002. [DOI] [PubMed] [Google Scholar]
- 12.Herts BR, Schneider E, Poggio ED, Obuchowski NA, Baker ME. Identifying outpatients with renal insufficiency before contrast-enhanced CT by using estimated glomerular filtration rates versus serum creatinine levels. Radiology. 2008;248:106–113. doi: 10.1148/radiol.2481071528. [DOI] [PubMed] [Google Scholar]
- 13.Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function--measured and estimated glomerular filtration rate. N Engl J Med. 2006;354:2473–2483. doi: 10.1056/NEJMra054415. [DOI] [PubMed] [Google Scholar]
- 14.Thomsen HS, Morcos SK ESUR. ESUR guidelines on contrast media. Abdom Imaging. 2006;31:131–140. doi: 10.1007/s00261-005-0380-y. [DOI] [PubMed] [Google Scholar]
- 15.Katzberg RW, Lamba R. Contrast-induced nephropathy after intravenous administration: fact or fiction? Radiol Clin North Am. 2009;47:789–800. v. doi: 10.1016/j.rcl.2009.06.002. [DOI] [PubMed] [Google Scholar]
- 16.El-Hajjar M, Bashir I, Khan M, Min J, Torosoff M, DeLago A. Incidence of contrast-induced nephropathy in patients with chronic renal insufficiency undergoing multidetector computed tomographic angiography treated with preventive measures. Am J Cardiol. 2008;102:353–356. doi: 10.1016/j.amjcard.2008.03.067. [DOI] [PubMed] [Google Scholar]
- 17.Mehran R, Aymong ED, Nikolsky E, Lasic Z, Iakovou I, Fahy M, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44:1393–1399. doi: 10.1016/j.jacc.2004.06.068. [DOI] [PubMed] [Google Scholar]
- 18.Marenzi G, Lauri G, Assanelli E, Campodonico J, De Metrio M, Marana I, et al. Contrast-induced nephropathy in patients undergoing primary angioplasty for acute myocardial infarction. J Am Coll Cardiol. 2004;44:1780–1785. doi: 10.1016/j.jacc.2004.07.043. [DOI] [PubMed] [Google Scholar]
- 19.Pannu N, Wiebe N, Tonelli M Alberta Kidney Disease Network. Prophylaxis strategies for contrast-induced nephropathy. JAMA. 2006;295:2765–2779. doi: 10.1001/jama.295.23.2765. [DOI] [PubMed] [Google Scholar]
- 20.Ledermann HP, Mengiardi B, Schmid A, Froehlich JM. Screening for renal insufficiency following ESUR (European Society of Urogenital Radiology) guidelines with on-site creatinine measurements in an outpatient setting. Eur Radiol. 2010;20:1926–1933. doi: 10.1007/s00330-010-1754-2. [DOI] [PubMed] [Google Scholar]
- 21.Hallan SI, Matsushita K, Sang Y, Mahmoodi BK, Black C, Ishani A, et al. Age and association of kidney measures with mortality and end-stage renal disease. JAMA. 2012;308:2349–2360. doi: 10.1001/jama.2012.16817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Carstensen M, Keer D, Rempel J, Jeon P, Barrett B. Prevalence of risk factors for contrast-induced nephrotoxicity in outpatients undergoing intravenous contrast-enhanced computed tomography studies. Can Assoc Radiol J. 2012;63:177–182. doi: 10.1016/j.carj.2010.12.004. [DOI] [PubMed] [Google Scholar]