

Abstract
Ocular chemical burns are common and serious ocular emergencies that require immediate and intensive evaluation and care. The victims of such incidents are usually young, and therefore loss of vision and disfigurement could dramatically affect their lives. The clinical course can be divided into immediate, acute, early, and late reparative phases. The degree of limbal, corneal, and conjunctival involvement at the time of injury is critically associated with prognosis. The treatment starts with simple but vision saving steps and is continued with complicated surgical procedures later in the course of the disease. The goal of treatment is to restore the normal ocular surface anatomy and function. Limbal stem cell transplantation, amniotic membrane transplantation, and ultimately keratoprosthesis may be indicated depending on the patients' needs.
1. Introduction
A chemical ocular burn usually occurs when a corrosive substance is accidentally introduced to the eye and/or periocular tissues. Chemical burn is considered a true ocular emergency and requires immediate and intensive evaluation and care. This type of injury is most common among men 20 to 40 years of age that typically work in industrial chemical laboratories or factories [1]. Given their younger age, the long-term disabilities that follow ocular burns could dramatically affect the patients' lives. The goal of treatment is to minimize further damage to ocular surface and ultimately restore a normal ocular surface anatomy and visual function.
2. Presentation
The typical presentation after a chemical injury is a sudden onset of severe pain, epiphora, and blepharospasm [2]. Basic substances are lipophilic and penetrate the eye more rapidly compared to acidic chemicals. They may also find their way to the anterior chamber damaging the trabecular meshwork, ciliary body, and the lens. Due to the rapidity of this process, patients may experience irreversible intraocular damage in as little as 5–15 minutes [2]. Acid injuries tend to be less severe. Acids cause protein coagulation in the epithelium, which limits further penetration into the deeper layers of the eye (hydrofluoric acid is an exception among acid since it can rapidly pass through cell membranes) [3–5]. Shrinkage and contraction of the cornea and sclera may lead to acute rise of intraocular pressure. Long-term rises of intraocular pressure can occur from fibrotic damage to the trabecular meshwork as well as the inflammatory debris trapping within the meshwork [1–3]. Conjunctival inflammation and loss of goblet cells can leave the ocular surface prone to dryness, scarring, and contracture of the fornices [2, 3, 6, 7].
3. Clinical Examination
The initial examination (after thorough irrigation as described below) includes a complete eye examination [1, 2, 7]. It is essential to make sure that no foreign bodies are embedded in any part of the ocular structures. A spectrum of clinical manifestations after a chemical injury could be described, which may vary substantially over time. Acute periocular signs of injury include periorbital edema and erythema, deepithelialized skin, and loss of eyelashes and eyebrows. Early signs include corneal and conjunctival epithelial defects, chemosis, conjunctival inflammation, limbal ischemia (Figure 1), corneal cloudiness, sterile ulceration, edema, and occasionally perforation [1, 7]. High intraocular pressure may result from damage and/or inflammation of the trabecular meshwork. One of the most important prognostic factors for the visual outcome is the extent of ocular surface damage, initially reflected by the amount of limbal ischemia (Figure 2) [1–3, 6–8]. Extensive damage to the limbus leads to limbal stem cell deficiency (LSCD) which may ultimately result in failure of normal corneal epithelial healing, neovascularization, and conjunctivalization. Lagophthalmos can also interfere with reepithelialization; it may be secondary to mechanical changes in the lids, secondary to edema or scarring. Extensive conjunctival burns can lead to long-term consequences including symblepharon, cicatricial entropion and ectropion, and trichiasis that may further complicate the presentations [2, 9–14].
Figure 1.
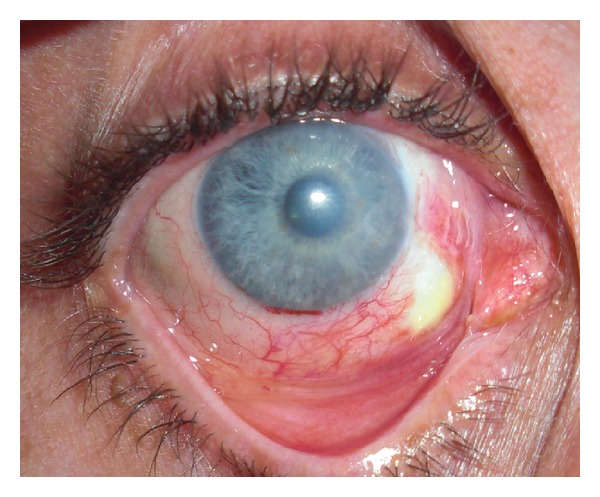
Limbal ischemia in the inferonasal quadrant 8 days after alkali burn. Patient subsequently underwent tenonplasty and conjunctival advancement to cover the defect.
Figure 2.
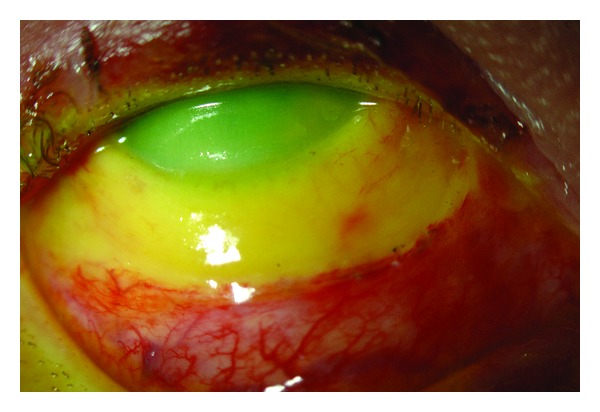
Patient with grade IV ocular surface burn. Note severe ischemia extending 4 mm from the cornea and corneal haze. Patient required multiple reconstructive procedures including combined conjunctival-limbal autograft and keratolimbal allograft.
4. Classification
Identifying the stage of a chemical eye burn is particularly helpful in prediction of the outcome. Most importantly, the relative proportion of surviving limbal tissue has been shown to be a major prognostic factor [1–3, 6–8]. Several classifications have been proposed [15–17]: the Roper-Hall classification system was initially developed in the mid 1960s, first by Ballen [18], and then modified by Roper-Hall [17]. The basis of this classification was largely on the degree of corneal haze and the amount of perilimbal ischemia (Table 1). Pfister subsequently presented a classification system grading the injury from mild, mild-moderate, moderate to severe, severe, and very severe based upon photographs demonstrating corneal haze and perilimbal ischemia [15]. Dua proposed a classification scheme based on clock hour limbal involvement (versus ischemia) as well as percentage of bulbar conjunctival involvement [16]. Overall, the key element is to note the amount of limbal, corneal, and conjunctival involvement at the time of injury [1].
Table 1.
Roper-Hall classification for the severity of ocular surface burns.
| Grade | Clinical findings | Prognosis | |
|---|---|---|---|
| Cornea | Conjunctiva/limbus | ||
| I | Corneal epithelial damage | No limbal ischemia | Good |
| II | Corneal haze, iris details visible | <1/3 limbal ischemia | Good |
| III | Total epithelial loss, stromal haze, and iris details obscured | 1/3–1/2 limbal ischemia | Guarded |
| IV | Cornea opaque, iris and pupil obscured | >1/2 limbal ischemia | Poor |
5. Pathogenesis
The typical pathophysiological course of events starts with a sudden change of tissue pH followed by pH-dependent chemical alterations [19, 20]. Until recently, the chemical characteristics including pH of the hazardous agent have been considered as the key element in determining the amount and type of tissue damage [19]. However, it has been shown that other factors such as temperature, amount, impact force, concentration, dissociation coefficient (e.g., osmolarity), redox-potential, and specific reactivity with the ocular tissues (pK values) can greatly influence the pathophysiologic cascade of chemical tissue damage [3].
The temperature determines nonspecific coagulation or cooling of the tissues. A hot solution generally causes more damage than a similar cool solution, since the chemical reactivity usually increases with a rise in temperature [3]. Solid substances are not removed by blinking, and corrosive powders such as lime or concrete may remain in greater concentration in conjunctival sac and thus have higher chances to destroy the tissues. Lime particles in particular may cause severe ongoing damage if they remain unnoticed in the deep fornices [3, 21]. The impact force of a corrosive agent is also noteworthy [3]; it influences the amount of corrosive substance placed on the cornea and in the conjunctival sac as well as the tissue reactivity after the accident. Low-concentration corrosives may cause extensive damage to the eye if they hit the cornea with great force. The resulting superficial corneal damage leads to direct stromal contact with the corrosive agent [22, 23]. A combination of acid burns with ocular contusion has been described for exploding modern car batteries [24, 25]. Similarly, the osmolarity gradient plays a major role in the propagation and progression of tissue damage caused by chemical burns [3, 26–28].
Alkaline agents, in general, penetrate more deeply than acids. The hydroxyl ion causes saponification of fatty acids in cell membranes which results in cellular disruption [19]. Once the epithelium is compromised, alkaline solutions penetrate more rapidly into the underlying tissues, destroying proteoglycan ground substance and the collagen matrix. If the agent reaches the collagen fibrils of the trabecular meshwork, it can cause scarring inhibiting aqueous outflow, leading to secondary glaucoma. Strong alkaline agents penetrate into the anterior chamber and cause widespread inflammation of iris, lens, and ciliary body [7, 19]. Acids can denature proteins and cause coagulation necrosis, forming a barrier which can reduce further tissue penetration [6, 7, 29]. As mentioned earlier, hydrofluoric acid may exceptionally penetrate as readily as alkaline agents creating the same spectrum of injuries [3–5]. It should be emphasized that while acidic agents cannot penetrate as quickly and readily as alkaline agents, they are nonetheless quite capable of causing severe damage to the ocular surface.
The lysis of cell membranes liberates mediators of chemotaxis and inflammation such as prostaglandins, leukotrienes, and interleukins leading to an immediate immunological response [30, 31]. The uniform initial clinical picture does not follow a common chemical or physical mechanism but rather is the reflection of a general disturbance of corneal hydration, protein content, and cell vitality [3]. Subsequent progression of the injury and the healing process may fall anywhere between a highly active inflammatory process to a hyporeactive nonviable process due to complete tissue necrosis [3, 8, 30–32].
6. Clinical Course
The clinical course of ocular chemical injury can be divided into immediate, acute, early reparative (8–20 days), and late reparative phases [33].
The immediate phase begins from the moment a chemical agent comes in contact with the ocular surface [1, 33]. The key elements for determining the extent of chemical ocular injury and prognosis consist of the total area of the corneal epithelial defect, the area of the conjunctival epithelial defect, the amount of clock hours or degrees of limbal blanching, the area and density of corneal opacification, and increased IOP on presentation and loss of lens clarity [1, 15–17, 33].
The first seven days after chemical eye injury constitute the acute phase of recovery. During this time, the tissues clear themselves of contaminants while reestablishing the superficial protective layer of corneal epithelium. Significant inflammatory mechanisms begin to evolve on the ocular surface and the anterior chamber [1, 33]. In this stage, there is usually a rise in the IOP in a bimodal manner [8].
Early reparative phase, 8–20 days after the injury, is the transition period of ocular healing, in which the immediate regeneration of ocular surface epithelium and acute inflammatory events give way to chronic inflammatory response, stromal repair, and scarring [1, 33]. A persistent epithelial defect can lead to corneal ulceration during this stage. It has been attributed to action of digestive enzymes such as collagenase, metalloproteinase, and other proteases released from the polymorphonuclear leukocytes and the healing epithelium [34–40].
Three weeks after a chemical injury, the healing process continues with so-called late reparative phase. This stage is characterized by completion of healing with good visual prognosis and complications in those with guarded visual prognosis [1, 33]. A chronic, severe inflammatory reaction is often triggered by breakdown products of the damaged ocular tissue that act as new antigens, causing invasion of leukocytes and macrophages [30, 31]. In severe cases, this may involve the eyelids, the peripheral vitreous, and the retina [41]. Treatment-resistant secondary glaucoma is a frequent complication, requiring surgical intervention and long-time treatment with antiglaucomatous medications [3, 41]. Corneal scarring, xerophthalmia, ankyloblepharon uveitis, cataract, symblephara, cicatricial entropion or ectropion, and trichiasis may occur subsequently [42–46].
7. Management of Chemical Burns
Care of chemical burns essentially echoes both the basic mechanism of the initial incident and the subsequent inflammatory response.
7.1. Emergency Therapy
Immediacy of treatment influences the final outcome favorably; hence, one should not delay the treatment waiting for careful assessment of the injury. After an acute chemical burn, immediate and extensive irrigation is necessary to wash out the offending chemicals [6, 19, 26, 29, 47–49]. It is suggested to continue rinsing the eye for no less than 10 minutes [3]. Irrigating contact lenses including Morgan Lens can also be used to provide ocular irrigation and/or medication to the cornea and conjunctiva after chemical burn [50]. Commonly, the ocular surface pH is checked using a urinary pH strip and irrigation is continued until pH normalizes to 7. Universal systems like amphoteric solutions (mostly Diphoterine) have less exothermic reactivity in addition to nonspecific binding capacity to bases and acids which makes them appropriate solutions for emergency neutralization [51–53]. Any remaining particles are removed from the ocular surface with a moist cotton tip or fine-tipped forceps. Successful first line management of eye burns and adequate training of nonophthalmological emergency teams are imperative to ensure the best possible outcome. It is shown that prognosis is closely related to the efficiency of the immediate treatment measures [3, 54].
7.2. Acute Phase Treatment
The treatment plan largely depends on the examination findings. The main objectives of acute phase treatment are to foster reepithelialization, decrease inflammation, prevent infection, avoid further epithelial and stromal breakdown, and minimize the sequela.
7.3. Promoting Reepithelization
Preservative free tear substitutes and lubricating ointment can ameliorate persistent epitheliopathy, reduce the risk of recurrent erosions, and accelerate visual rehabilitation [1]. Generally, burn patients benefit from systemic ascorbic acid which may promote collagen synthesis and wound healing [36, 55, 56]. Autologous serum tears which contain many factors that promote healing may be used to promote epithelialization [57–63]. Likewise, bandage contact lenses may be considered for delayed epithelial healing. Large-diameter gas-permeable scleral contact lenses, such as the prosthetic replacement of ocular surface ecosystem (PROSE) (originally called the Boston Scleral Lens), have been used after chemical or thermal injury in an inpatient setting [7, 64–67]. They can also protect the cornea from desiccation and friction of the eyelids via blinking [68].
7.4. Anti-Inflammatory Therapy
Topical corticosteroids play a critical role in controlling acute inflammation after chemical injuries. They reduce inflammatory cell infiltration and stabilize neutrophilic cytoplasmic and lysosomal membranes. They also help resolving anterior chamber as well as conjunctival inflammation [69]. The downside is that they also inhibit reepithelialization and collagen synthesis. The conventional belief is that topical steroids should not be used beyond 10 to 14 days, as they increase the risk of inhibition of collagenesis, worsening corneal thinning, and possible corneal perforation in alkali burns [70, 71]. However, this is primarily a concern in severe injuries with persistent epithelial defects; otherwise, corticosteroids can (and should) be used safely beyond 7–10 days if the epithelium has already closed [15, 72].
Citrate has been used successfully to prevent polymorphonuclear leukocyte migration into the burnt tissue, thus reducing the release of free radicals and proteolytic enzymes [36, 55, 56]. Free radicals are formed by hydroxyl ions and may be scavenged by ascorbic acid and tocopherols [3]. Cycloplegic drops can be considered to blunt the pain from iris-ciliary body spasm [19].
7.5. Treatment of High Intraocular Pressure
As mentioned, alkali injuries that reach the trabecular meshwork can lead to elevated intraocular pressure which can be easily overlooked [73]. To minimize toxicity to the epithelium, oral aqueous suppression is generally preferred over topical agents.
7.6. Sequelae Prevention
The ocular surface should be inspected daily for symblepharon formation. A symblepharon ring can be placed in the fornices to effectively prevent symblepharon formation [7]. The largest size is preferable which provides good separation of the palpebral conjunctiva from the bulbar conjunctiva. Although the above measures can successfully prevent symblepharon formation in the acute phase, they cannot prevent the chronic cicatricial changes that lead to the formation of scarring and adhesions [74].
Corneal ulceration and melting tend to occur in the most severe injuries. Corneal thinning is potentiated by collagenases or matrix metelloproteinases, released from polymorphonuclear cells and other resident cells [75]. Proteinase inhibitors such as Aprotinin and collagenase inhibitors such as cysteine, acetylcysteine, sodium ethylenediamine tetra acetic acid (EDTA), calcium EDTA, penicillamine, citrate, and especially tetracyclines were found to prevent corneal thinning in chemically burned corneas [1, 19, 35, 75–77]. Systemic tetracycline may also boost healing of persistent corneal epithelial defects [7, 34].
8. Surgical Management
The primary intention of early surgery in the face of a chemical ocular burn is to maintain the globe and promote reepithelialization. Surgical management starts with initial debridement of the necrotic material and continues with amniotic membrane transplantation and tectonic grafting if necessary. Late surgical interventions, on the other hand, are aimed at restoring the normal ocular surface anatomy and visual function. These include correcting eyelid abnormalities, management of glaucoma, limbal stem cell transplantation, and ultimately keratoplasty.
8.1. Amniotic Membrane Transplantation
Amniotic membrane transplantation (AMT) can be used both as a graft which can provide a basement membrane for epithelialization and/or as a patch where it acts as a biological bandage contact lens [78–80]. It was shown that cryopreserved amniotic membrane transplantation to the entire ocular surface within two weeks of a chemical or thermal burn results in immediate pain relief and healing of epithelial defects in patients with grade II-III burns [81]. In addition, it is often used as an adjunct to medical therapy to decrease ocular surface inflammation and reduce scarring [2, 9, 79, 81–95]. Besides, multilayered AMT is an appropriate surrogate in severe corneal thinning [96, 97]. Further, amniotic membrane may also be applied to the cornea using a contact lens type carrier (ProKera, Bio-Tissue, Inc., Miami, FL) with the amniotic membrane being secured to a flexible plastic ring [11, 98]. The ring-amniotic membrane complex is placed onto the ocular surface, without any need for suturing or gluing. The amniotic membrane usually lasts days to weeks (typically around one week); however, its application can be repeated. Furthermore, AMT may be used as an adjunct to different techniques of stem cell transplantations if those procedures are indicated in the course of the treatment [11, 13, 14, 46, 82, 83, 98–103].
8.2. Tenonplasty
In severe, grade IV injuries, the loss of limbal vascularity may lead to anterior segment necrosis in addition to lack of reepithelialization and subsequent conjunctivalization of the cornea. Early intervention to reestablish the limbal blood supply may potentially prevent late complications [104]. Tenonplasty involves debridement of necrotic tissue and advancing viable, vascular Tenon's layer to the limbus securing it to sclera, combined with AMT with or without lamellar corneal patch grafting (Figure 1). It has been shown to prevent further scleral ischemia and melting [3, 104, 105].
8.3. Limbal Stem Cell Transplantation
Limbal stem cells deficiency is one of the most visually significant long-term sequelae of severe chemical injuries. Patients suffering from chronic irritation persistent epithelial defects with clinical signs of corneal conjunctivalization may be considered for stem cell transplantation [11, 12, 14, 103, 105–109]. In general, it is best to delay limbal stem cell transplantation (from the time of injury) as much as possible, since the more the ocular surface inflammation is controlled, the better the results would be. Likewise, it is advised to have all eyelid abnormalities (e.g., trichiasis and symblepharon) addressed before considering limbal stem cell transplantation [14, 45, 46, 103, 106, 110, 111].
Limbal stem cells can be harvested from the patient (conjunctival-limbal autograft (CLAU) [44] and cultivated limbal epithelial transplantation (CLET) [43]), immediate family members including parents, siblings, or children (living-related conjunctival-limbal allograft (lr-CLAL)), or cadaveric eyes (keratolimbal allograft (KLAL)). Several surgical techniques have been described [14, 99, 112–115]. CLAU is only possible in unilateral burns but invariably has excellent results, with complete regression of corneal neovascularization such that successful reepithelialization and functional vision are achieved in 80–90% of patients (Figure 3) [44, 116]. CLET is a very suitable surgical alternative in cases with total unilateral LSCD [43]. In patients with bilateral ocular surface injury, lr-CLAL or KLAL are the available options. Harvesting tissue from one eye or both eyes of a first-degree relative provides fresh tissue with closer genetic composition. On the other hand, KLAL graft is more accessible with more stem cells because of larger clock hours of graft tissue available (Figure 4). Lr-CLAL also has the advantage of providing viable conjunctival tissue which may be used in patients with severe conjunctival deficiency. Systemic immunosuppression consisting of short-term steroids, tacrolimus (or cyclosporine), and mycophenolate (or azathioprine) is necessary to prevent limbal allograft rejection [14, 106, 110, 111]. Close collaboration with an organ transplant team is generally needed for the optimal management of the immunosuppression and monitoring of side effects [117].
Figure 3.

Patient with total limbal stem cell deficiency after chemical burn who was successfully treated with conjunctival-limbal autograft (2 years after surgery).
Figure 4.

Patient with total limbal stem cell deficiency after chemical burn who underwent keratolimbal allograft and penetrating keratoplasty with systemic immunosuppression (18 months after surgery).
8.4. Corneal Transplantation
Tectonic penetrating keratoplasty (PKP) which is a surgical intervention of last resort in burn patients may be inevitable in cases with severe thinning, large descemetoceles, and impending or frank corneal perforation. Conventional lamellar keratoplasty (LKP) or deep anterior lamellar keratoplasty (DALK; Melles and Anwar techniques) can be performed for visual rehabilitation of patients with extensive stromal scarring [118, 119]. Most often, due to corneal scar formation and variability of corneal thickness and irregularity, conventional LKP and Melles techniques are preferred [118]. Otherwise, full thickness transplants can be performed successfully, once the limbal stem cell deficiency has been addressed [120].
8.5. Keratoprosthesis
Artificial corneas undoubtedly can improve vision but should be considered in cases when PKP has failed or expected to fail (e.g., in the setting of extensive stromal vascularization) [121–126]. Currently, the Boston keratoprosthesis remains the main option in patients in which it has not been possible to restore corneal clarity and a normal ocular surface with any of previous measures [121, 127]. Their long-term risks, the need for life-long regular followups, and adherence to daily antibiotic prophylaxis are some of the issues that may make some patients less than ideal candidates for keratoprosthesis [122, 124, 125]. The Boston keratoprosthesis study group found excellent anatomical retention in patients with a chemical burn [122]. Reported long-term complications include retroprosthetic membrane formation, intraocular pressure elevation and/or glaucoma progression, sterile corneal stromal necrosis or corneal thinning, infectious keratitis, persistent epithelial defect, retinal detachment, sterile uveitis/vitritis, and infectious endophthalmitis [128–130]. The osteo-odonto-keratoprosthesis (OOKP) surgery is one of the last resorts usually kept for patients with bilateral corneal blindness resulting from several ocular and systemic pathologies [131]. Indications include severe end-stage Stevens-Johnson syndrome, Lyell's syndrome, epidermolysis bullosa, severe trachoma, chemical or physical injury, loss of lids, and multiple corneal graft failure. Other surgical alternatives available for treatment of such cases (e.g., ocular surface reconstruction with stem cell transplant) should be considered prior to OOKP surgery [132].
9. Conclusion
Chemical burns can have devastating consequences for the ocular surface and periocular structures. They frequently cause chronic pain, disfigurement, and vision loss. The overall goal of treatment is restoration of the normal ocular surface anatomy which starts with intensive treatment in the beginning and ultimately complex surgical procedures later in the course. With advancements in regenerative medicine, the clinical outcomes are expected to improve further.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
References
- 1.Singh P, Tyagi M, Kumar Y, et al. Ocular chemical injuries and their management. Oman Journal of Ophthalmology. 2013;6(2):83–86. doi: 10.4103/0974-620X.116624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fish R, Davidson RS. Management of ocular thermal and chemical injuries, including amniotic membrane therapy. Current Opinion in Ophthalmology. 2010;21(4):317–321. doi: 10.1097/ICU.0b013e32833a8da2. [DOI] [PubMed] [Google Scholar]
- 3.Schrage NF, Langefeld S, Zschocke J, Kuckelkorn R, Redbrake C, Reim M. Eye burns: an emergency and continuing problem. Burns. 2000;26(8):689–699. doi: 10.1016/s0305-4179(00)00044-9. [DOI] [PubMed] [Google Scholar]
- 4.McCulley JP. Ocular hydrofluoric acid burns: animal model, mechanism of injury and therapy. Transactions of the American Ophthalmological Society. 1990;88:649–684. [PMC free article] [PubMed] [Google Scholar]
- 5.Kirkpatrick JJR, Enion DS, Burd DAR. Hydrofluoric acid burns: a review. Burns. 1995;21(7):483–493. doi: 10.1016/0305-4179(95)93254-h. [DOI] [PubMed] [Google Scholar]
- 6.Spector J, Fernandez WG. Chemical, thermal, and biological ocular exposures. Emergency Medicine Clinics of North America. 2008;26(1):125–136. doi: 10.1016/j.emc.2007.11.002. [DOI] [PubMed] [Google Scholar]
- 7.Lin A, Patel N, Yoo D, Demartelaere S, Bouchard C. Management of ocular conditions in the burn unit: thermal and chemical burns and stevens-johnson syndrome/toxic epidermal necrolysis. Journal of Burn Care & Research. 2011;32(5):547–560. doi: 10.1097/BCR.0b013e31822b0f29. [DOI] [PubMed] [Google Scholar]
- 8.Paterson CA, Pfister RR. Intraocular pressure changes after alkali burns. Archives of Ophthalmology. 1974;91(3):211–218. doi: 10.1001/archopht.1974.03900060219014. [DOI] [PubMed] [Google Scholar]
- 9.Shekhar H, Titiyal J, Sinha R, Tinwala S. Amniotic membrane transplantation in ocular surface disorders: a review. Journal of Clinical Ophthalmology and Research. 2013;1(1):64–69. [Google Scholar]
- 10.Liu J, Sheha H, Fu Y, Liang L, Tseng SCG. Update on amniotic membrane transplantation. Expert Review of Ophthalmology. 2010;5(5):645–661. doi: 10.1586/eop.10.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liang L, Sheha H, Li J, Tseng SC. Limbal stem cell transplantation: new progresses and challenges. Eye. 2009;23(10):1946–1953. doi: 10.1038/eye.2008.379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cauchi PA, Ang GS, Azuara-Blanco A, Burr JM. A systematic literature review of surgical interventions for limbal stem cell deficiency in humans. American Journal of Ophthalmology. 2008;146(2):251.e2–259.e2. doi: 10.1016/j.ajo.2008.03.018. [DOI] [PubMed] [Google Scholar]
- 13.Lavker RM, Tseng SC, Sun TT. Corneal epithelial stem cells at the limbus: looking at some old problems from a new angle. Experimental Eye Research. 2004;78(3):433–446. doi: 10.1016/j.exer.2003.09.008. [DOI] [PubMed] [Google Scholar]
- 14.Kim JY, Djalilian AR, Schwartz GS, Holland EJ. Ocular surface reconstruction: limbal stem cell transplantation. Ophthalmology Clinics of North America. 2003;16(1):67–77. doi: 10.1016/s0896-1549(02)00107-4. [DOI] [PubMed] [Google Scholar]
- 15.Pfister RR. Chemical injuries of the eye. Ophthalmology. 1983;90(10):1246–1253. [PubMed] [Google Scholar]
- 16.Dua HS, King AJ, Joseph A. A new classification of ocular surface burns. British Journal of Ophthalmology. 2001;85(11):1379–1383. doi: 10.1136/bjo.85.11.1379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Roper-Hall MJ. Thermal and chemical burns. Transactions of the Ophthalmological Societies of the United Kingdom. 1965;85:631–653. [PubMed] [Google Scholar]
- 18.Ballen PH. Treatment of chemical burns of the eye. Eye, Ear, Nose & Throat Monthly. 1964;43:57–61. [PubMed] [Google Scholar]
- 19.Wagoner MD. Chemical injuries of the eye: current concepts in pathophysiology and therapy. Survey of Ophthalmology. 1997;41(4):275–313. doi: 10.1016/s0039-6257(96)00007-0. [DOI] [PubMed] [Google Scholar]
- 20.Pfister RR. The effects of chemical injury on the ocular surface. Ophthalmology. 1983;90(6):601–609. doi: 10.1016/s0161-6420(83)34509-7. [DOI] [PubMed] [Google Scholar]
- 21.Schirner G, Schrage NF, Salla S, Reim M, Burchard W-G. Conjunctival tissue examination in severe eye burns: a study with scanning electron microscopy and energy dispersive X-ray analysis. Graefe's Archive for Clinical and Experimental Ophthalmology. 1995;233(5):251–256. doi: 10.1007/BF00177645. [DOI] [PubMed] [Google Scholar]
- 22.Frazer DG, Armstrong MFJ, Archer DB. Compression keratopathy. American Journal of Ophthalmology. 1986;102(2):208–210. doi: 10.1016/0002-9394(86)90146-7. [DOI] [PubMed] [Google Scholar]
- 23.Bullock JD, Ballal DR, Johnson DA, Bullock RJ. Ocular and orbital trauma from water balloon slingshots: a clinical, epidemiologic, and experimental study. Ophthalmology. 1997;104(5):878–887. doi: 10.1016/s0161-6420(97)30218-8. [DOI] [PubMed] [Google Scholar]
- 24.Siebert S. Ocular trauma from lead-acid vehicle battery explosions. Australian Journal of Ophthalmology. 1982;10(1):53–61. [PubMed] [Google Scholar]
- 25.Monestier-Carlus D, Jonqueres J, Ayral G. Ocular accidents caused by explosion of the so-called maintenance-free batteries. Bulletin des societes d'ophtalmologie de France. 1988;88(3):323–326. [PubMed] [Google Scholar]
- 26.Paterson CA, Pfister RR, Levinson RA. Aqueous humor pH changes after experimental alkali burns. American Journal of Ophthalmology. 1975;79(3):414–419. doi: 10.1016/0002-9394(75)90614-5. [DOI] [PubMed] [Google Scholar]
- 27.Maurice DM. The permeability to sodium ions of the living rabbit's cornea. The Journal of Physiology. 1951;112(3-4):367–391. doi: 10.1113/jphysiol.1951.sp004535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Schrage NF, Flick S, Redbrake C, Reim M. Electrolytes in the cornea: a therapeutic challenge. Graefe's Archive for Clinical and Experimental Ophthalmology. 1996;234(12):761–764. doi: 10.1007/BF00189358. [DOI] [PubMed] [Google Scholar]
- 29.Salzman M, O'Malley RN. Updates on the evaluation and management of caustic exposures. Emergency Medicine Clinics of North America. 2007;25(2):459–476. doi: 10.1016/j.emc.2007.02.007. [DOI] [PubMed] [Google Scholar]
- 30.Pfister RR, Haddox JL, Sommers CI. Alkali-degraded cornea generates a low molecular weight chemoattractant for polymorphonuclear leukocytes. Investigative Ophthalmology and Visual Science. 1993;34(7):2297–2304. [PubMed] [Google Scholar]
- 31.Pfister RR, Haddox JL, Dodson RW, Harkins LE. Alkali-burned collagen produces a locomotory and metabolic stimulant to neutrophils. Investigative Ophthalmology and Visual Science. 1987;28(2):295–304. [PubMed] [Google Scholar]
- 32.Chiang TS, Moorman LR, Thomas RP. Ocular hypertensive response following acid and alkali burns in rabbits. Investigative Ophthalmology. 1971;10(4):270–273. [PubMed] [Google Scholar]
- 33.McCulley JP. Chemical injuries. In: Smolin G, Thoft R, editors. The Cornea: Scientific Foundation and Clinical Practice. Boston, Mass, USA: Little Brown and Company; 1987. [Google Scholar]
- 34.Seedor JA, Perry HD, McNamara TF, Golub LM, Buxton DF, Guthrie DS. Systemic tetracycline treatment of alkali-induced corneal ulceration in rabbits. Archives of Ophthalmology. 1987;105(2):268–271. doi: 10.1001/archopht.1987.01060020122043. [DOI] [PubMed] [Google Scholar]
- 35.Ralph RA. Tetracyclines and the treatment of corneal stromal ulceration: a review. Cornea. 2000;19(3):274–277. doi: 10.1097/00003226-200005000-00003. [DOI] [PubMed] [Google Scholar]
- 36.Pfister RR, Nicolaro ML, Paterson CA. Sodium citrate reduces the incidence of corneal ulcerations and perforations in extreme alkali-burned eyes—acetylcysteine and ascorbate have no favorable effect. Investigative Ophthalmology and Visual Science. 1981;21(3):486–490. [PubMed] [Google Scholar]
- 37.Perry HD, Kenyon KR, Lamberts DW, Foulks GN, Seedor JA, Golub LM. Systemic tetracycline hydrochloride as adjunctive therapy in the treatment of persistent epithelial defects. Ophthalmology. 1986;93(10):1320–1322. doi: 10.1016/s0161-6420(86)33570-x. [DOI] [PubMed] [Google Scholar]
- 38.Golub LM, Lee HM, Lehrer G, et al. Minocycline reduces gingival collagenolytic activity during diabetes. Preliminary observations and a proposed new mechanism of action. Journal of Periodontal Research. 1983;18(5):516–526. doi: 10.1111/j.1600-0765.1983.tb00388.x. [DOI] [PubMed] [Google Scholar]
- 39.Brown SI, Weller CA. Collagenase inhibitors in prevention of ulcers of alkali-burned cornea. Archives of Ophthalmology. 1970;83(3):352–353. doi: 10.1001/archopht.1970.00990030352013. [DOI] [PubMed] [Google Scholar]
- 40.Brown SI, Akiya S, Weller CA. Prevention of the ulcers of the alkali-burned cornea. Preliminary studies with collagenase inhibitors. Archives of Ophthalmology. 1969;82(1):95–97. doi: 10.1001/archopht.1969.00990020097023. [DOI] [PubMed] [Google Scholar]
- 41.Kuckelkorn R, Kottek A, Reim M. Intraocular complications following severe eye burns. Frequency and management. Klinische Monatsblatter fur Augenheilkunde. 1994;205(2):86–92. doi: 10.1055/s-2008-1045497. [DOI] [PubMed] [Google Scholar]
- 42.Sharifipour F, Baradaran-Rafii A, Idani E, Zamani M, Bonyadi MHJ. Oxygen therapy for acute ocular chemical or thermal burns: a pilot study. American Journal of Ophthalmology. 2011;151(5):823–828. doi: 10.1016/j.ajo.2010.11.005. [DOI] [PubMed] [Google Scholar]
- 43.Eslani M, Baradaran-Rafii A, Ahmad S. Cultivated limbal and oral mucosal epithelial transplantation. Seminars in Ophthalmology. 2012;27(3-4):80–93. doi: 10.3109/08820538.2012.680641. [DOI] [PubMed] [Google Scholar]
- 44.Eslani M, Baradaran-Rafii A, Djalilian A. Conjunctival-Limbal Autograft (CLAU) In: Thomsen WL, editor. Advances in Eye Research. Vol. 1. Hauppauge, NY, USA: Nova Biomedical Press; 2011. [Google Scholar]
- 45.Baradaran-Rafii A, Eslani M, Djalillian AR. Complications of keratolimbal allograft surgery. Cornea. 2013;32(5):561–566. doi: 10.1097/ICO.0b013e31826215eb. [DOI] [PubMed] [Google Scholar]
- 46.Baradaran-Rafii A, Eslani M, Jamali H, Karimian F, Tailor UA, Djalilian AR. Postoperative complications of conjunctival limbal autograft surgery. Cornea. 2012;31(8):893–899. doi: 10.1097/ICO.0b013e31823f095d. [DOI] [PubMed] [Google Scholar]
- 47.Rodrigues Z. Irrigation of the eye after alkaline and acidic burns. Emergency Nurse. 2009;17(8):26–29. doi: 10.7748/en2009.12.17.8.26.c7431. [DOI] [PubMed] [Google Scholar]
- 48.Gerard M, Merle H, Chiambaretta F, Rigal D, Schrage N. An amphoteric rinse used in the emergency treatment of a serious ocular burn. Burns. 2002;28(7):670–673. doi: 10.1016/s0305-4179(02)00094-3. [DOI] [PubMed] [Google Scholar]
- 49.Chau JPC, Lee DTF, Lo SHS. A systematic review of methods of eye irrigation for adults and children with ocular chemical burns. Worldviews on Evidence—Based Nursing. 2012;9(3):129–138. doi: 10.1111/j.1741-6787.2011.00220.x. [DOI] [PubMed] [Google Scholar]
- 50.Morgan LB. A new drug delivery system for the eye. IMS, Industrial Medicine and Surgery. 1971;40(6):11–13. [PubMed] [Google Scholar]
- 51.Schrage NF, Schlomacher B, Aschenbernner W, Langefeld S. Phosphate buffer in alkali eye burns as an inducer of experimental corneal calcification. Burns. 2001;27(5):459–464. doi: 10.1016/s0305-4179(00)00148-0. [DOI] [PubMed] [Google Scholar]
- 52.Schrage NF, Kompa S, Haller W, Langefeld S. Use of an amphoteric lavage solution for emergency treatment of eye burns: first animal type experimental clinical considerations. Burns. 2002;28(8):782–786. doi: 10.1016/s0305-4179(02)00194-8. [DOI] [PubMed] [Google Scholar]
- 53.Rihawi S, Frentz M, Reim M, Schrage NF. Rinsing with isotonic saline solution for eye burns should be avoided. Burns. 2008;34(7):1027–1032. doi: 10.1016/j.burns.2008.01.017. [DOI] [PubMed] [Google Scholar]
- 54.Kuckelkorn R, Kottek A, Schrage N, Reim M. Poor prognosis of severe chemical and thermal eye burns: the need for adequate emergency cave and primary prevention. International Archives of Occupational and Environmental Health. 1995;67(4):281–284. doi: 10.1007/BF00409410. [DOI] [PubMed] [Google Scholar]
- 55.Pfister RR, Paterson CA. Ascorbic acid in the treatment of alkali burns of the eye. Ophthalmology. 1980;87(10):1050–1057. doi: 10.1016/s0161-6420(80)35126-9. [DOI] [PubMed] [Google Scholar]
- 56.Pfister RR, Haddox JL, Lank KM. Citrate or ascorbate/citrate treatment of established corneal ulcers in the alkali-injured rabbit eye. Investigative Ophthalmology & Visual Science. 1988;29(7):1110–1115. [PubMed] [Google Scholar]
- 57.Vajpayee RB, Mukerji N, Tandon R, et al. Evaluation of umbilical cord serum therapy for persistent corneal epithelial defects. British Journal of Ophthalmology. 2003;87(11):1312–1316. doi: 10.1136/bjo.87.11.1312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Tsubota K, Goto E, Fujita H, et al. Treatment of dry eye by autologous serum application in Sjogren's syndrome. British Journal of Ophthalmology. 1999;83(4):390–395. doi: 10.1136/bjo.83.4.390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Tananuvat N, Daniell M, Sullivan LJ, et al. Controlled study of the use of autologous serum in dry eye patients. Cornea. 2001;20(8):802–806. doi: 10.1097/00003226-200111000-00005. [DOI] [PubMed] [Google Scholar]
- 60.Poon AC, Geerling G, Dart JKG, Fraenkel GE, Daniels JT. Autologous serum eyedrops for dry eyes and epithelial defects: clinical and in vitro toxicity studies. British Journal of Ophthalmology. 2001;85(10):1188–1197. doi: 10.1136/bjo.85.10.1188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Panda A, Jain M, Vanathi M, Velpandian T, Khokhar S, Dada T. Topical autologous platelet-rich plasma eyedrops for acute corneal chemical injury. Cornea. 2012;31(9):989–993. doi: 10.1097/ICO.0b013e3182114661. [DOI] [PubMed] [Google Scholar]
- 62.Imanishi J, Kamiyama K, Iguchi I, Kita M, Sotozono C, Kinoshita S. Growth factors: importance in wound healing and maintenance of transparency of the cornea. Progress in Retinal and Eye Research. 2000;19(1):113–129. doi: 10.1016/s1350-9462(99)00007-5. [DOI] [PubMed] [Google Scholar]
- 63.Goto E, Shimmura S, Shimazaki J, Tsubota K. Treatment of superior limbic keratoconjunctivitis by application of autologous serum. Cornea. 2001;20(8):807–810. doi: 10.1097/00003226-200111000-00006. [DOI] [PubMed] [Google Scholar]
- 64.Segal O, Barkana Y, Hourovitz D, et al. Scleral contact lenses may help where other modalities fail. Cornea. 2003;22(4):308–310. doi: 10.1097/00003226-200305000-00006. [DOI] [PubMed] [Google Scholar]
- 65.Ruedemann AD, Jr., Jardon F. Ten years experience with scleral lenses. Transactions of the American Ophthalmological Society. 1970;68:245–276. [PMC free article] [PubMed] [Google Scholar]
- 66.Kalwerisky K, Davies B, Mihora L, Czyz CN, Foster JA, Demartelaere S. Use of the Boston ocular surface prosthesis in the management of severe periorbital thermal injuries: a case series of 10 patients. Ophthalmology. 2012;119(3):516–521. doi: 10.1016/j.ophtha.2011.08.027. [DOI] [PubMed] [Google Scholar]
- 67.Burns CL, Chylack LT., Jr. Thermal burns: the management of thermal burns of the lids and globes. Annals of Ophthalmology. 1979;11(9):1358–1368. [PubMed] [Google Scholar]
- 68.Rosenthal P, Cotter J. The Boston scleral lens in the management of severe ocular surface disease. Ophthalmology Clinics of North America. 2003;16(1):89–93. doi: 10.1016/s0896-1549(02)00067-6. [DOI] [PubMed] [Google Scholar]
- 69.Saud EE, Moraes HV, Jr., Marculino LG, Gomes JA, Allodi S, Miguel NC. Clinical and histopathological outcomes of subconjunctival triamcinolone injection for the treatment of acute ocular alkali burn in rabbits. Cornea. 2012;31(2):181–187. doi: 10.1097/ICO.0b013e318221ce99. [DOI] [PubMed] [Google Scholar]
- 70.Donshik PC, Berman MB, Dohlman CH, Gage J, Rose J. Effect of topical corticosteroids on ulceration in alkali-burned corneas. Archives of Ophthalmology. 1978;96(11):2117–2120. doi: 10.1001/archopht.1978.03910060497024. [DOI] [PubMed] [Google Scholar]
- 71.Beams R, Linabery L, Grayson M. Effect of topical corticosteroids on corneal wound strength. American Journal of Ophthalmology. 1968;66(6):1131–1133. doi: 10.1016/0002-9394(68)90822-2. [DOI] [PubMed] [Google Scholar]
- 72.Davis AR, Ali QH, Aclimandos WA, Hunter PA. Topical steroid use in the treatment of ocular alkali burns. British Journal of Ophthalmology. 1997;81(9):732–734. doi: 10.1136/bjo.81.9.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Tsai JH, Derby E, Holland EJ, Khatana AK. Incidence and prevalence of glaucoma in severe ocular surface disease. Cornea. 2006;25(5):530–532. doi: 10.1097/01.ico.0000220776.93852.d9. [DOI] [PubMed] [Google Scholar]
- 74.Gregory DG. The ophthalmologic management of acute Stevens-Johnson syndrome. Ocular Surface. 2008;6(2):87–95. doi: 10.1016/s1542-0124(12)70273-2. [DOI] [PubMed] [Google Scholar]
- 75.Reim M, Bahrke C, Kuckelkorn R, Kuwert T. Investigation of enzyme activities in severe burns of the anterior eye segment. Graefe's Archive for Clinical and Experimental Ophthalmology. 1993;231(5):308–312. doi: 10.1007/BF00919110. [DOI] [PubMed] [Google Scholar]
- 76.Ling S, Li W, Liu L, et al. Allograft survival enhancement using doxycycline in alkali-burned mouse corneas. Acta Ophthalmologica. 2013;91(5):e369–e378. doi: 10.1111/aos.12070. [DOI] [PubMed] [Google Scholar]
- 77.Gabler WR, Creamer HR. Suppression of human neutrophil functions by tetracyclines. Journal of Periodontal Research. 1991;26(1):52–58. doi: 10.1111/j.1600-0765.1991.tb01626.x. [DOI] [PubMed] [Google Scholar]
- 78.Shimmura S, Shimazaki J, Ohashi Y, Tsubota K. Antiinflammatory effects of amniotic membrane transplantation in ocular surface disorders. Cornea. 2001;20(4):408–413. doi: 10.1097/00003226-200105000-00015. [DOI] [PubMed] [Google Scholar]
- 79.Dua HS, Gomes JAP, King AJ, Maharajan VS. The amniotic membrane in ophthalmology. Survey of Ophthalmology. 2004;49(1):51–77. doi: 10.1016/j.survophthal.2003.10.004. [DOI] [PubMed] [Google Scholar]
- 80.Bouchard CS, John T. Amniotic membrane transplantation in the management of severe ocular surface disease: indications and outcomes. Ocular Surface. 2004;2(3):201–211. doi: 10.1016/s1542-0124(12)70062-9. [DOI] [PubMed] [Google Scholar]
- 81.Meller D, Pires RTF, Mack RJS, et al. Amniotic membrane transplantation for acute chemical or thermal burns. Ophthalmology. 2000;107(5):980–990. doi: 10.1016/s0161-6420(00)00024-5. [DOI] [PubMed] [Google Scholar]
- 82.Baradaran-Rafii A, Javadi M, Rezaei Kanavi M, Eslani M, Jamali H, Karimian F. Limbal stem cell deficiency in chronic and delayed-onset mustard gas keratopathy. Ophthalmology. 2010;117(2):246–252. doi: 10.1016/j.ophtha.2009.07.012. [DOI] [PubMed] [Google Scholar]
- 83.Tseng SCG. Amniotic membrane transplantation for ocular surface reconstruction. Bioscience Reports. 2001;21(4):481–489. doi: 10.1023/a:1017995810755. [DOI] [PubMed] [Google Scholar]
- 84.Kheirkhah A, Johnson DA, Paranjpe DR, Raju VK, Casas V, Tseng SCG. Temporary sutureless amniotic membrane patch for acute alkaline burns. Archives of Ophthalmology. 2008;126(8):1059–1066. doi: 10.1001/archopht.126.8.1059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Tseng SCG, di Pascuale MA, Liu DT, Ying YG, Baradaran-Rafii A. Intraoperative mitomycin C and amniotic membrane transplantation for fornix reconstruction in severe cicatricial ocular surface diseases. Ophthalmology. 2005;112(5):896–903. doi: 10.1016/j.ophtha.2004.11.041. [DOI] [PubMed] [Google Scholar]
- 86.Tejwani S, Kolari RS, Sangwan VS, Rao GN. Role of amniotic membrane graft for ocular chemical and thermal injuries. Cornea. 2007;26(1):21–26. doi: 10.1097/ICO.0b013e31802b4201. [DOI] [PubMed] [Google Scholar]
- 87.Tandon R, Gupta N, Kalaivani M, Sharma N, Titiyal JS, Vajpayee RB. Amniotic membrane transplantation as an adjunct to medical therapy in acute ocular burns. British Journal of Ophthalmology. 2011;95(2):199–204. doi: 10.1136/bjo.2009.173716. [DOI] [PubMed] [Google Scholar]
- 88.Sorsby A, Symons HM. Amniotic membrane grafts in caustic burns of the eye (burns of the second degree) The British Journal of Ophthalmology. 1946;30:337–345. [PubMed] [Google Scholar]
- 89.Sinha R, Tinwala S, Shekhar H, Titiyal J. Amniotic membrane transplantation in ocular surface disorders: a review. Journal of Clinical Ophthalmology and Research. 2013;1(1, article 64) [Google Scholar]
- 90.Shahriari HA, Tokhmehchi F, Reza M, Hashemi NF. Comparison of the effect of amniotic membrane suspension and autologous serum on alkaline corneal epithelial wound healing in the rabbit model. Cornea. 2008;27(10):1148–1150. doi: 10.1097/ICO.0b013e318173138a. [DOI] [PubMed] [Google Scholar]
- 91.Kim JC, Tseng SC. Transplantation of preserved human amniotic membrane for surface reconstruction in severely damaged rabbit corneas. Cornea. 1995;14(5):473–484. [PubMed] [Google Scholar]
- 92.Gomes JAP, dos Santos MS, Cunha MC, Mascaro VLD, de Nadai Barros J, de Sousa LB. Amniotic membrane transplantation for partial and total limbal stem cell deficiency secondary to chemical burn. Ophthalmology. 2003;110(3):466–473. doi: 10.1016/s0161-6420(02)01888-2. [DOI] [PubMed] [Google Scholar]
- 93.Fernandes M, Sridhar MS, Sangwan VS, Rao GN. Amniotic membrane transplantation for ocular surface reconstruction. Cornea. 2005;24(6):643–653. doi: 10.1097/01.ico.0000151501.80952.c5. [DOI] [PubMed] [Google Scholar]
- 94.Azuara-Blanco A, Pillai CT, Dua HS. Amniotic membrane transplantation for ocular surface reconstruction. The British Journal of Ophthalmology. 1999;83(4):399–402. doi: 10.1136/bjo.83.4.399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Clare G, Suleman H, Bunce C, Dua H. Amniotic membrane transplantation for acute ocular burns. Cochrane Database of Systematic Reviews. 2012;9 doi: 10.1002/14651858.CD009379.pub2.CD009379 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Alió JL, Abad M, Scorsetti DH. Preparation, indications and results of human amniotic membrane transplantation for ocular surface disorders. Expert Review of Medical Devices. 2005;2(2):153–160. doi: 10.1586/17434440.2.2.153. [DOI] [PubMed] [Google Scholar]
- 97.Hanada K, Shimazaki J, Shimmura S, Tsubota K. Multilayered amniotic membrane transplantation for severe ulceration of the cornea and sclera. American Journal of Ophthalmology. 2001;131(3):324–331. doi: 10.1016/s0002-9394(00)00825-4. [DOI] [PubMed] [Google Scholar]
- 98.Kheirkhah A, Casas V, Raju VK, Tseng SCG. Sutureless amniotic membrane transplantation for partial limbal stem cell deficiency. American Journal of Ophthalmology. 2008;145(5):787–794. doi: 10.1016/j.ajo.2008.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Javadi M, Baradaran-Rafii A. Living-related conjunctival-limbal allograft for chronic or delayed-onset mustard gas keratopathy. Cornea. 2009;28(1):51–57. doi: 10.1097/ICO.0b013e3181852673. [DOI] [PubMed] [Google Scholar]
- 100.Liang L, Sheha H, Tseng SC. Long-term outcomes of keratolimbal allograft for total limbal stem cell deficiency using combined immunosuppressive agents and correction of ocular surface deficits. Archives of Ophthalmology. 2009;127(11):1428–1434. doi: 10.1001/archophthalmol.2009.263. [DOI] [PubMed] [Google Scholar]
- 101.Meller D, Tseng SC. Reconstruction of the conjunctival and corneal surface. Transplantation of amnionic membrane. Ophthalmologe. 1998;95(12):805–813. doi: 10.1007/s003470050357. [DOI] [PubMed] [Google Scholar]
- 102.Sangwan VS, Tseng SC. New perspectives in ocular surface disorders. An integrated approach for diagnosis and management. Indian Journal of Ophthalmology. 2001;49(3):153–168. [PubMed] [Google Scholar]
- 103.Bakhtiari P, Djalilian A. Update on limbal stem cell transplantation. Middle East African Journal of Ophthalmology. 2010;17(1):9–14. doi: 10.4103/0974-9233.61211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Kuckelkorn R, Schrage N, Reim M. Treatment of severe eye burns by tenonplasty. The Lancet. 1995;345(8950):657–658. doi: 10.1016/s0140-6736(95)90564-2. [DOI] [PubMed] [Google Scholar]
- 105.Tseng SCG, Prabhasawat P, Barton K, Gray T, Meiler D. Amniotic membrane transplantation with or without limbal allografts for corneal surface reconstruction in patients with limbal stem cell deficiency. Archives of Ophthalmology. 1998;116(4):431–441. doi: 10.1001/archopht.116.4.431. [DOI] [PubMed] [Google Scholar]
- 106.Djalilian AR, Mahesh SP, Koch CA, et al. Survival of donor epithelial cells after limbal stem cell transplantation. Investigative Ophthalmology and Visual Science. 2005;46(3):803–807. doi: 10.1167/iovs.04-0575. [DOI] [PubMed] [Google Scholar]
- 107.Fernandes M, Sangwan VS, Rao SK, et al. Limbal stem cell transplantation. Indian Journal of Ophthalmology. 2004;52(1):5–22. [PubMed] [Google Scholar]
- 108.Crawford AZ, Mcghee CNJ. Management of limbal stem cell deficiency in severe ocular chemical burns. Clinical & Experimental Ophthalmology. 2012;40(3):227–229. doi: 10.1111/j.1442-9071.2012.02775.x. [DOI] [PubMed] [Google Scholar]
- 109.Anderson DF, Ellies P, Pires RTF, Tseng SCG. Amniotic membrane transplantation for partial limbal stem cell deficiency. British Journal of Ophthalmology. 2001;85(5):567–575. doi: 10.1136/bjo.85.5.567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Welder JD, Pandya HK, Nassiri N, Djalilian AR. Conjunctival limbal autograft and allograft transplantation using fibrin glue. Ophthalmic Surgery Lasers and Imaging. 2012;43(4):323–327. doi: 10.3928/15428877-20120618-04. [DOI] [PubMed] [Google Scholar]
- 111.Nassiri N, Pandya HK, Djalilian AR. Limbal allograft transplantation using fibrin glue. Archives of Ophthalmology. 2011;129(2):218–222. doi: 10.1001/archophthalmol.2010.370. [DOI] [PubMed] [Google Scholar]
- 112.Espana EM, Di Pascuale M, Grueterich M, Solomon A, Tseng SCG. Keratolimbal allograft in corneal reconstruction. Eye. 2004;18(4):406–417. doi: 10.1038/sj.eye.6700670. [DOI] [PubMed] [Google Scholar]
- 113.Solomon A, Ellies P, Anderson DF, et al. Long-term outcome of keratolimbal allograft with or without penetrating keratoplasty for total limbal stem cell deficiency. Ophthalmology. 2002;109(6):1159–1166. doi: 10.1016/s0161-6420(02)00960-0. [DOI] [PubMed] [Google Scholar]
- 114.Dua HS, Azuara-Blanco A. Allo-limbal transplantation in patients with limbal stem cell deficiency. British Journal of Ophthalmology. 1999;83(4):414–419. doi: 10.1136/bjo.83.4.414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Daya SM, Ilari FACSL. Living related conjunctival limbal allograft for the treatment of stem cell deficiency. Ophthalmology. 2001;108(1):126–133. doi: 10.1016/s0161-6420(00)00475-9. [DOI] [PubMed] [Google Scholar]
- 116.Özdemir Ö, Tekeli O, Örnek K, Arslanpençe A, Yalçindağ NF. Limbal autograft and allograft transplantations in patients with corneal burns. Eye. 2004;18(3):241–248. doi: 10.1038/sj.eye.6700640. [DOI] [PubMed] [Google Scholar]
- 117.Krakauer M, Welder JD, Pandya HK, Nassiri N, Djalilian AR. Adverse effects of systemic immunosuppression in keratolimbal allograft. Journal of Ophthalmology. 2012;2012:5 pages. doi: 10.1155/2012/576712.576712 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Baradaran-Rafii A, Eslani M, Sadoughi M-M, Esfandiari H, Karimian F. Anwar versus melles deep anterior lamellar keratoplasty for keratoconus: a prospective randomized clinical trial. Ophthalmology. 2013;120(2):252–259. doi: 10.1016/j.ophtha.2012.07.090. [DOI] [PubMed] [Google Scholar]
- 119.Alio JL, Shah S, Barraquer C, Bilgihan K, Anwar M, Melles GRJ. New techniques in lamellar keratoplasty. Current Opinion in Ophthalmology. 2002;13(4):224–229. doi: 10.1097/00055735-200208000-00006. [DOI] [PubMed] [Google Scholar]
- 120.Nassiri N, Djalilian AR. Keratoplasty: moving to the front. Journal of Ophthalmic & Vision Research. 2009;4(1):5–7. [PMC free article] [PubMed] [Google Scholar]
- 121.Hou JH, de la Cruz J, Djalilian AR. Outcomes of boston keratoprosthesis implantation for failed keratoplasty after keratolimbal allograft. Cornea. 2012;31(12):1432–1435. doi: 10.1097/ICO.0b013e31823e2ac6. [DOI] [PubMed] [Google Scholar]
- 122.Zerbe BL, Belin MW, Ciolino JB. Results from the multicenter Boston type 1 keratoprosthesis study. Ophthalmology. 2006;113(10, article e1):1779–1784. doi: 10.1016/j.ophtha.2006.05.015. [DOI] [PubMed] [Google Scholar]
- 123.Hicks CR, Crawford GJ, Dart JKG, et al. AlphaCor: clinical outcomes. Cornea. 2006;25(9):1034–1042. doi: 10.1097/01.ico.0000229982.23334.6b. [DOI] [PubMed] [Google Scholar]
- 124.Harissi-Dagher M, Dohlman CH. The Boston Keratoprosthesis in severe ocular trauma. Canadian Journal of Ophthalmology. 2008;43(2):165–169. doi: 10.3129/i08-009. [DOI] [PubMed] [Google Scholar]
- 125.Bradley JC, Hernandez EG, Schwab IR, Mannis MJ. Boston type 1 keratoprosthesis: the University of California Davis experience. Cornea. 2009;28(3):321–327. doi: 10.1097/ICO.0b013e31818b8bfa. [DOI] [PubMed] [Google Scholar]
- 126.Dohlman CH, Schneider HA, Doane MG. Prosthokeratoplasty. American Journal of Ophthalmology. 1974;77(5):694–700. doi: 10.1016/0002-9394(74)90534-0. [DOI] [PubMed] [Google Scholar]
- 127.Aldave AJ, Kamal KM, Vo RC, Yu F. The Boston type I keratoprosthesis: improving outcomes and expanding indications. Ophthalmology. 2009;116(4):640–651. doi: 10.1016/j.ophtha.2008.12.058. [DOI] [PubMed] [Google Scholar]
- 128.Kim MJ, Bakhtiari P, Aldave AJ. The international use of the boston type I keratoprosthesis. International Ophthalmology Clinics. 2013;53(2):79–89. doi: 10.1097/IIO.0b013e31827ab3d3. [DOI] [PubMed] [Google Scholar]
- 129.Khan BF, Harissi-Dagher M, Khan DM, Dohlman CH. Advances in Boston keratoprosthesis: enhancing retention and prevention of infection and inflammation. International Ophthalmology Clinics. 2007;47(2):61–71. doi: 10.1097/IIO.0b013e318036bd8b. [DOI] [PubMed] [Google Scholar]
- 130.Aldave AJ, Sangwan VS, Basu S, et al. International results with the Boston type I keratoprosthesis. Ophthalmology. 2012;119(8):1530–1538. doi: 10.1016/j.ophtha.2012.02.015. [DOI] [PubMed] [Google Scholar]
- 131.Gomaa A, Comyn O, Liu C. Keratoprostheses in clinical practice—a review. Clinical and Experimental Ophthalmology. 2010;38(2):211–224. doi: 10.1111/j.1442-9071.2010.02231.x. [DOI] [PubMed] [Google Scholar]
- 132.Hille K, Grabner G, Liu C, Colliardo P, Falcinelli G, Taloni M. Standards for modified osteoodontokeratoprosthesis (OOKP) surgery according to Strampelli and Falcinelli: the Rome-Vienna Protocol. Cornea. 2005;24(8):895–908. doi: 10.1097/01.ico.0000157401.81408.62. [DOI] [PubMed] [Google Scholar]