

Abstract
Purpose
To evaluate safety, gastrointestinal tolerance, and growth of a new experimental starter formula (NESF) fortified with lutein, prebiotics, probiotics, nucleotides and beta-carotene, fed to infants within the first months of life.
Methods
This was a non-randomized, open, uncontrolled study conducted from December 2010 to May 2011. Twenty-three healthy infants aged 10 days to 2 months old were enrolled. Outcomes included gastrointestinal tolerance, physical growth and safety. Prior to the initiation of the trial, the Scientific Research Institute of Nutrition of the Russian Academy of Medical Sciences confirmed that the NESF met all safety and nutritional parameters.
Results
NESF was well tolerated. The majority of infants fed this formula passed semi-liquid, yellow or yellow-brown. The mean stool frequency/day was 2.5±0.4 on study-day 14 and 1.8±0.5 on study-day 28. The mean daily weight gain was 30.9±3.8 grams and the mean length gain during the 28 days of follow up was 3.1±0.8 cm, corresponding to the average physical growth normally seen in the first months of life in Russian infants. Six children left the study: one refused to drink the formula, one left the study as parents changed residence; and one child's parents have recalled their informed consent due to adverse event unrelated to the product. Three infants presented adverse events possibly related to the product (rash; colic and abdominal pain; constipation). Seventeen infants completed the trial.
Conclusion
This study demonstrated that lutein-fortified formula is safe, well-tolerated and supported physical growth of evaluated infants.
Keywords: Infant formula, Lutein, Gastrointestinal tolerance, Safety
INTRODUCTION
Breastfeeding is viewed as the optimal method of infant feeding that provides many benefits to both the infant and the mother. Exclusive breastfeeding is recommended up to 6 months of age, with continued breastfeeding, along with appropriate complementary foods, up to 2 years of age or beyond. The Russian Ministry of Health and Social Development has made breastfeeding a cornerstone of its maternal and child-health program. However, despite great efforts in support of breastfeeding being made in the Russian Federation, its rate is still low [1].
Infant formulas are intended to serve as a substitute for breast milk in infants who cannot be fed at the breast, or should not receive breast milk, or for whom breast milk is not available [2]. Most of the modern infant formulas currently in the Russian market are also enriched with nucleotides, taurine, long-chain polyunsaturated fatty acids, etc. In recent years, researchers have been paying particular attention to another functional component of breast milk, the carotenoid lutein, which is a representative of the class of natural carotenoids and has a chemical structure close to that of beta-carotene but with no vitamin A activity. Significant quantities of lutein and its isomer, zeaxanthin, have been found in the eye tissue and, in particular, the yellow spot, where their concentrations are three times higher than the average concentrations in other eye tissues. The biological and physiological functions of lutein are associated with its participation in the development and function of the eyes in infants [3,4].
Lutein has an antioxidant activity and a role as an optical filter that protects the retina from being damaged by light wavelengths from 400 to 500 nm (blue light). Lutein and zeaxanthin are localized in the eye area that contains retinal receptors rich in lipids (i.e., in the position optimal for exerting protection). This information is in accordance with the epidemiological data obtained in human observations and implying that lutein is capable of decreasing the risk of senile degeneration of the yellow pigment, which is the main cause of blindness in the elderly; this process may begin very early, as the immature lens of infants cannot ensure filtration of ultraviolet and blue light reaching the retina and causing damage [5]. These data indicate that lutein is critical for maintaining visual function. At the same time, the pigments lutein and zeaxanthin are not synthesized in the human body. Therefore, they can be classified as essential micronutrients that must be present in infants' and children's food. The main dietary source of lutein and zeaxanthin for adults and older children is vegetables and fruit. The main source of lutein and zeaxanthin for infants under the age of 1 year, especially during the first few months of life, is breast milk [6].
The lutein content of breast milk varies from 3 to 232 µg/L, depending on the lactation stage and place of residence. The average lutein content of breast milk is 15-17 µg/L in Australia, the United Kingdom, and Canada and 44-45µg/L in Japan and China. Levels vary from 146 µg/L (for colostrum) to 22 µg/L (after 6 months of lactation) in the United States. These variations mainly depend on the nutrition of the breastfeeding woman [7]. In contrast to breast milk, infant formulas contain only minor quantities of lutein. High-performance liquid chromatography (HPLC) studies yield levels from 0.07 to 0.13 µg/L [8]. As a result, a number of infant formula manufacturers have recently developed lutein-fortified formulas.
The data obtained from volunteers who took very large amounts of lutein, as well as from animal studies, has confirmed the safety of lutein intake [9]. However, the inclusion of any new ingredient in the composition of infant formulas requires (in accordance with the current international practice) thorough additional hygienic and clinical-physiological assessment of the nutritional safety and efficacy of this component. In Russia, this assessment should include a detailed analysis undertaken to find out whether all tested sanitary-chemical and microbiological safety indices of the ingredient meet the requirements of applicable Russian and international hygienic standards. A subsequent clinical evaluation is needed in many cases. In fact, regulations set standards for manufacturers to produce safe infant formulas that support healthy growth. Clinical studies are essential to ensure the safety of infant formulas, and deviation from normal physical growth and development, attributable to a new ingredient, should be considered a safety risk. Growth studies, currently a core of clinical evaluation of infant formulas, should include precise and reliable measurements of gains in weight and length, as well as gastrointestinal tolerance and food intake [10].
Infant formulas are the sole or predominant source of nutrition for many infants and are fed during a sensitive period of development; therefore, assessments on safety and efficacy are recommended. Adhering to the above requirements, we carried out a safety, tolerance, and growth assessment in infants younger than 2 months of age, who were fed with a new infant formula fortified with lutein.
MATERIALS AND METHODS
This was a nonrandomized, open, uncontrolled study of safety and tolerance of a new experimental starter infant formula (NESF). This formula (Similac; Premium 1 from Abbott Laboratories, SA, Spain) is an instant, adapted milk intended for mixed and bottle-feeding of infants aged from a few days to 6 months old. The study was conducted in the period from December 2010 to May 2011. The composition of this NESF (Table 1) includes defatted dry milk; a whey protein concentrate; lactose; partially hydrolyzed whey proteins; galactooligosaccharides (GOS); a mixture of vegetable oils without palm olein; a mixture of vitamins and mineral substances; lutein; a probiotic culture of Bifidobacterium lactis; L-tryptophan; choline; L-carnitine; inositol; taurine; and the nucleotides adenosine, cytidine, guanosine, and uridine monophosphate. The hygienic expert assessment conducted by the Scientific Research Institute of Nutrition of the Russian Academy of Medical Sciences has confirmed that the NESF meets all safety standards and the regulated nutritive value parameters. In addition, the NESF meets the Russian Federation law on "Technical regulations for milk and dairy products," the International Codex Alimentarius established by Food and Agriculture Organization/World Health Organization, and the European Union Directive standards. The energy content of the formula is 680 kcal/L, which meets domestic and international standards established for adapted milk formulas [11,12]. In contrast to the previously used adapted milk formulas, the experimental product contains lutein levels not exceeding 250 µg/L, meeting governmental regulations for milk and dairy products. The source of lutein used for this formula is marigold (Calendula), a plant of the Asteraceae family.
Table 1.
Composition of Study Product
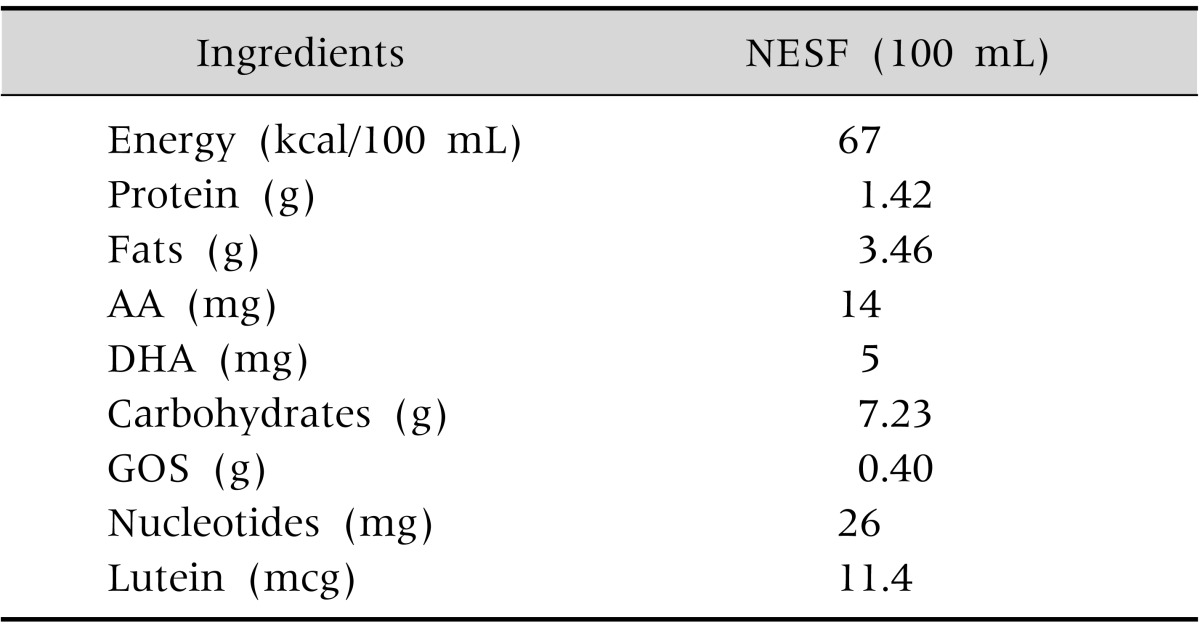
NESF: new experimental starter formula, AA: arachidonic acid, DHA: docosahexaenoic acid, GOS: galactooligosaccharide.
This was a multicenter study conducted at the following clinical sites: (1) Children's City Polyclinics No. 63 and No. 66 of the Moscow Department of Health; (2) Children's Polyclinic Department of Lyubertsy District Hospital No. 3; (3) Municipal Establishment of Health Care LDH No. 3, CPD No. 1; and (4) Children's City Polyclinic of Khimki, Moscow Region. An independent ethics committee approved the protocol.
Inclusion criteria included healthy, full-term infants (birth weight>2,490 g) less than 60-day-old and not receiving any additional food or supplements. Exclusion criteria included infants receiving breast milk in an amount above one-third of their total daily food intake, infants with medical conditions that could affect the interpretation of the dietary intervention, or a mother's history of drug abuse. Infants were withdrawn from the study if they started receiving additional food or other formula.
Criteria for evaluating the product's tolerance included (1) a subjective disapproval (drank willingly or unwillingly, refused to drink the product) and (2) a clinical assessment of the product's tolerability on the following basis: (a) daily registration of feeding frequency and the formula amount taken by the baby from the start of use to study day 28; (b) daily registration of undesirable clinical events (development or exacerbation of colic, or flatulence); (c) daily registration of stool frequency and consistency, the presence/absence of pathological inclusions in feces, its color, odor, etc.; and (d) behavioral assessment (was restless or irritability, liked being played with).
Changes in physical development markers included (1) body weight measurement at the start of the study, on study day 14 (±3 days), and on study day 28 (±3 days), using a standardized scale; (2) body length measurement at the start of the study, on study day 14 (±3 days), and on study day 28 (±3 days), using a standardized height meter; and (3) measurements of the head and chest circumferences at the start of the study, on study day 14 (±3 days), and on study day 28 (±3 days).
At the first visit, the parents signed the Informed Consent Form, and the investigators checked whether the infant met the inclusion/exclusion criteria; collected demographic data; and measured the infant's body weight, body length, and head and chest circumferences. The parents were instructed on how to prepare the formula and feed the baby. Information concerning the stool frequency, intake formula volume, and stool appearance was recorded in a specially designed diary to be filled out by the mother. The investigators conducted telephone interviews of the mothers several times throughout the product administration period.
During visit 2 (14th day of product use ±3 days) and visit 3 (28th day of product use ±3 days), the parents were asked to complete daily dietary intake records and stool records. Data collected included volume of formula consumed at each feeding, incidence of spit-up and vomiting associated with feedings, and characteristics of the infant's stools (frequency, consistency and color).
Investigators performed a physical examination and registered anthropometric data (body weight, body length, and head and chest circumferences) and the product amounts consumed on study days 14 and 28. We enrolled 23 infants aged 10 days to 2 months old. All infants were born at term and had satisfactory weights, heights, and Apgar scores. Delivery was natural in 19 women and by C-section in 4 women. By the time of study enrollment, subjects were receiving breast milk and formula (7 infants) or bottle only (16 infants). Feeding with the NESF was introduced gradually, beginning with 10-30 mL per feeding. The follow-up duration was up to study day 28.
RESULTS
Adaptation to the study formula was uncomplicated. The infants received the formula willingly and remained calm between feedings. The majority of study infants' parents noted good taste, consistency, and odor of the experimental product. Most mothers described the appearance and color of the formula as "very appropriate." In total, 6 children left the study: One refused to drink the formula; one left the study, as the parents changed their place of residence and it became impossible to follow up; and one child's parents recalled their informed consent due to an adverse event unrelated to the product's use. The other 3 subjects left the study due to adverse events possibly related to product use (one child has rash, one complained of colic and abdominal pain, and the third one had constipation). Seventeen infants completed the trial. Table 2 shows results obtained at the end of the feeding period. This information includes mean values of food intake, stool pattern, and anthropometrics. In fact, the mean daily formula consumed on study day 28 was 849.7+113.8 mL. The majority of infants fed the experimental product passed semiliquid, yellow or yellow-brown, odorless feces without pathological inclusions, with a frequency of 1 to 5 per day. The mean defecation frequency was found to be 2.5±0.4 per day on study day 14 and 1.8±0.5 per day on study day 28. Regarding anthropometrics, the mean body weight increment was found to be 30.9+3.8 g/day, with an average weight gain during this feeding period of 865.4+108.1; the mean length gain during the 28 days of follow-up was 3.1+0.8 cm; and the mean head circumference gain was 1.6+0.4, thus corresponding to the average physical development results normally seen in Russian infants in the first months of life.
Table 2.
Performance of New Experimental Starter Formula on Study Day 28
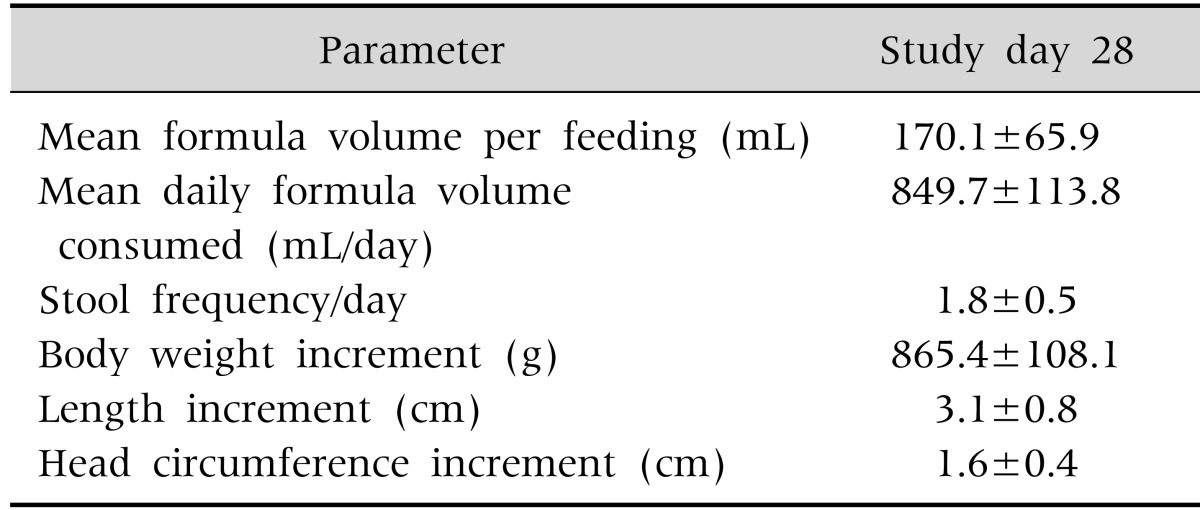
Values are presented as mean±standard error of the mean.
The z-scores of followed-up infants are presented in Table 3 and Fig. 1 and 2. As demonstrated by this table and these figures, the obtained physical development results were within respective reference intervals.
Table 3.
Z-score (Number of Subjects)
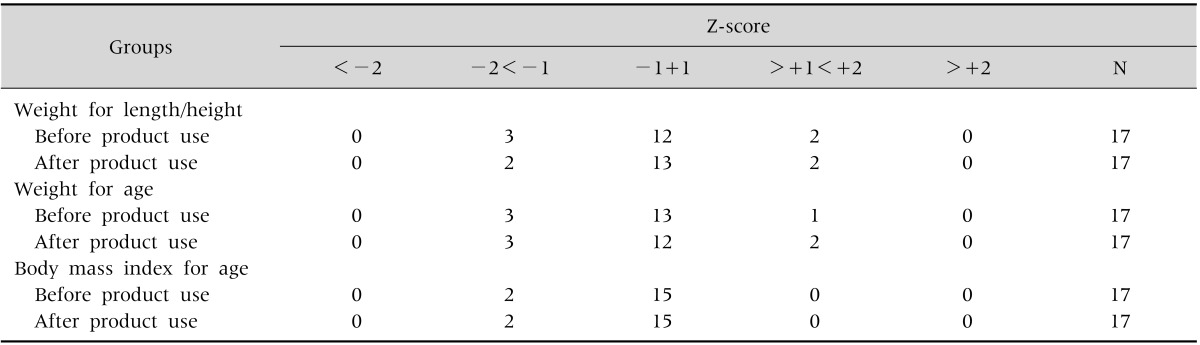
Fig. 1.

Z-score weight/age: before and after intervention. WHO: World Health Organization.
Fig. 2.

Z-score weight for length/height: before and after intervention. WHO: World Health Organization.
DISCUSSION
Optimal growth and development are the top goals of good nutrition for young children. In fact, the nutritional quality of the diet is of paramount importance at an early age. During the first few months after birth, tissue and organ synthesis rates are high while the processes of maturation continue rapidly [7]. Experts agree that breastfeeding is ideal for optimum nutrition. Infant formulas are intended to serve as a substitute for breast milk for infants who cannot be fed at the breast, or should not receive breast milk, or for whom breast milk is not available [13].
In recent years, scientific progress in infant nutrition has shown the role of some health-promoting nutrients. These bioactive ingredients exert a positive influence on function and well-being. These actions include supporting the development of the immune system, digestion/absorption of nutrients, vision and cognition, bone functions, etc. [14].
Broad variations of lutein in human milk exist and are highly related to maternal dietary intake. Lutein is not naturally found in infant formulas, and formulas are not routinely supplemented with this nutrient [8].
The main objective of this small pilot study was to assess the effect of a new infant formula supplemented with the carotenoid lutein on tolerance, growth, and safety of very young Russian infants.
Results showed that the experimental formula (EF) was well-tolerated by infants. In fact, the stool pattern showed that infants passed stools at an average of 2.5+0.4 on study day 14 and 1.8+0.5 on study day 28. No reports of constipation or liquid stools were obtained in the evaluable population. Stool consistency was similar to what we usually see in infants fed with human milk. The volume of formula intake matched standard volume intake for the age. Anthropometric growth also matched international standard increments for this age group.
In fact, on study day 28, the mean increment for weight gain was 856+108 g (with a daily weight gain of 30.9+3.8), for length gain was 3.1+0.8, and for head circumference was 1.6+0.4. All these results were within average standard increments for that age. Z-scores of weight for length, weight for age, and body mass index for age measured at baseline and at the completion of the study (pre- and post-intervention) also resulted in growth that matched international references.
A starter formula without lutein, similar in composition to the one tested in the present study, was studied in American infants [15]. This study was a randomized, double-blinded, safety and tolerance clinical trial conducted in 180 full-term, healthy infants. The arms included a control formula without prebiotics, two EFs supplemented with different levels of GOS (4 g/L and 8 g/L; EF-4 and EF-8, respectively), and a human milk-fed reference group. If we take the results of the arm EF-4 and compare this information to what we found with our NESF (a formula also fortified with 4 g of GOS), we find that 74% of children in both studies completed the trial. The percentage of children that did not complete the study due to adverse events is comparable between the trials. Data on weight gain per day, formula intake, mean number of stools per day, and stool consistency and color, as well as infant behavior and formula satisfaction, are not different between the two populations.
Mackey et al. [16] tested standard starter formulas supplemented with different levels of lutein. The control (no lutein added) and EFs in this study were also very similar in macro and micronutrients to the one we studied in the present study (NESF). The aim of these investigators was to assess plasma concentrations of beta-carotene, lutein, and lycopene 56 days after feeding infants milk-based infant formula without or with different concentrations of added carotenoids. Ninety-nine subjects were enrolled, and 23 were allocated to a formulation containing 52.6 mcg/L of lutein. From this group, 18 were considered evaluable subjects. Body weight, length, and head circumference measurements at Study Days 28 and 56 were comparable among all groups. Average daily study formula intake, number of study feedings, average number of stools per day, and predominant stool consistency were not significantly different between the formula groups in terms of safety. In addition, no differences in adverse event incidence were observed among the formula groups in the evaluable population.
A group of investigators in the Philippines [17] conducted a double-blind trial in 240 healthy, full-term infants younger than 2 weeks of age. The objective of this study was to assess the effects on growth and safety of an experimental standard starter formula supplemented with lutein. Infants were fed either the control formula (no lutein added) or EF (200 µg/L) with a 75% higher content of lutein than the level we tested in our study. Results showed that infants in both treatment groups demonstrated appropriate anthropometric growth. No differences between groups were found in any of the measures of growth. Gastrointestinal tolerance was good for the two groups. The composition in macro and micronutrients in this Asian trial was not similar to the formula we tested in Russia. However, the data obtained in this large trial, using a formula with much higher levels of lutein, support the safety of this ingredient when fed to young infants.
Lutein is the predominant carotenoid in the infant brain, accounting for more than half of the concentration of carotenoids [18]. No data currently exist that demonstrate lutein supplementation can influence brain development during critical/sensitive periods at an early age. However, a recent study in infants during the first year of life has shown that lutein and other carotenoids are present in the infant brain. The concentration of lutein was significantly higher than the other carotenoids in four critical brain regions important for learning [18] and development. In fact, lutein was highly concentrated in (1) the auditory cortex linked to language development; (2) the frontal cortex, which is recognized as being responsible for problem solving and motor function; (3) the hippocampus, known to be important for memory functions; and (4) the occipital cortex, responsible for the brain's visual-processing system. Therefore, we can assume that lutein may be important for early neural development. As infant formula is not normally supplemented with lutein, more investigation of the influence of lutein intake on neural development is justified.
In conclusion, our results demonstrated that the experimental NESF tested in the present study was well-tolerated, is safe, and supports normal infant growth. This preliminary information supports the safety of lutein-enriched infant formula and its ability to ensure normal infant growth. More studies are needed, with a bigger sample size, targeting the role of this very critical nutrient in the development of young babies.
References
- 1.Abolyan LV. The breastfeeding support and promotion in Baby-Friendly Maternity Hospitals and Not-as-Yet Baby-Friendly Hospitals in Russia. Breastfeed Med. 2006;1:71–78. doi: 10.1089/bfm.2006.1.71. [DOI] [PubMed] [Google Scholar]
- 2.Koletzko B, Baker S, Cleghorn G, Neto UF, Gopalan S, Hernell O, et al. Global standard for the composition of infant formula: recommendations of an ESPGHAN coordinated international expert group. J Pediatr Gastroenterol Nutr. 2005;41:584–599. doi: 10.1097/01.mpg.0000187817.38836.42. [DOI] [PubMed] [Google Scholar]
- 3.Hammond BR, Jr, Wooten BR, Curran-Celentano J. Carotenoids in the retina and lens: possible acute and chronic effects on human visual performance. Arch Biochem Biophys. 2001;385:41–46. doi: 10.1006/abbi.2000.2184. [DOI] [PubMed] [Google Scholar]
- 4.Landrum JT, Bone RA. Lutein, zeaxanthin, and the macular pigment. Arch Biochem Biophys. 2001;385:28–40. doi: 10.1006/abbi.2000.2171. [DOI] [PubMed] [Google Scholar]
- 5.Ham WT, Jr, Mueller HA, Ruffolo JJ, Jr, Clarke AM. Sensitivity of the retina to radiation damage as a function of wavelength. Photochem Photobiol. 1979;29:735–743. doi: 10.1111/j.1751-1097.1979.tb07759.x. [DOI] [PubMed] [Google Scholar]
- 6.Zimmer JP, Hammond BR., Jr Possible influences of lutein and zeaxanthin on the developing retina. Clin Ophthalmol. 2007;1:25–35. [PMC free article] [PubMed] [Google Scholar]
- 7.Jewell VC, Mayes CB, Tubman TR, Northrop-Clewes CA, Thurnham DI. A comparison of lutein and zeaxanthin concentrations in formula and human milk samples from Northern Ireland mothers. Eur J Clin Nutr. 2004;58:90–97. doi: 10.1038/sj.ejcn.1601753. [DOI] [PubMed] [Google Scholar]
- 8.Canfield LM, Clandinin MT, Davies DP, Fernandez MC, Jackson J, Hawkes J, et al. Multinational study of major breast milk carotenoids of healthy mothers. Eur J Nutr. 2003;42:133–141. doi: 10.1007/s00394-003-0403-9. [DOI] [PubMed] [Google Scholar]
- 9.Stahl W, Sies H. Antioxidant effects of carotenoids. In: Cadenas E, Packer L, editors. Handbook of antioxidants. 2nd ed. New York: Marcel Dekker Inc.; 2002. pp. 223–233. [Google Scholar]
- 10.National Research Council. Infant formula: evaluating the safety of new ingredients. Washington, DC: The National Academies Press; 2004. [PubMed] [Google Scholar]
- 11.Codex Alimentarius Commission of FAO/WHO. Rome: Codex Alimentarius Commission; Available from: http://www.codexalimentarius.org. [Google Scholar]
- 12.European Union Commission. European Union Commission Directive. Brussels: European Union Commission; 2013. Available from: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2013:230:0016:0019:EN:PDF. [Google Scholar]
- 13.World Health Organization. Resolution WHA 39.28. Infant and young child feeding. Volume 1. Resolutions and records. Final; Thirty-ninth World Health Assembly; Geneva; 5-16 May 1986. Geneva: World Health Organization; 1986. pp. 122–135. WHA39/1986/REC/1, annex 6. [Google Scholar]
- 14.Raikos V, Dassios T. Health-promoting properties of bioactive peptides derived from milk proteins in infant food: a review. Dairy Sci Technol. 2014;94:91–101. doi: 10.1007/s13594-013-0152-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Williams T, Choe Y, Price P, Katz G, Boff J, Suarez F, et al. Safety and tolerance of infant formulas containing prebiotics in healthy term infants. Microb Ecol. 57:585–586. doi: 10.1097/MPG.0000000000000513. [DOI] [PubMed] [Google Scholar]
- 16.Mackey AD, Albrecht D, Oliver J, Williams T, Long AC, Price PT. Plasma carotenoid concentrations of infants are increased by feeding a milk-based infant formula supplemented with carotenoids. J Sci Food Agric. 2013;93:1945–1952. doi: 10.1002/jsfa.5996. [DOI] [PubMed] [Google Scholar]
- 17.Capeding R, Gepanayao CP, Calimon N, Lebumfacil J, Davis AM, Stouffer N, et al. Lutein-fortified infant formula fed to healthy term infants: evaluation of growth effects and safety. Nutr J. 2010;9:22. doi: 10.1186/1475-2891-9-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Vishwanathan R, Kuchan M, Johnson E. Lutein is the predominant carotenoid in infant brain. Acta Biol Crac Ser Bot. 2011;53(Suppl 1):29. [Google Scholar]