

Abstract
Introduction
In recent years there has been a spurt of peer-reviewed publications on the ophthalmic complications of dengue fever. The authors aim to review the ocular manifestations, utility of relevant diagnostic tests, management, prognosis, and sequelae of dengue-related ocular complications.
Methods
A comprehensive literature search was conducted on Medline, PubMed, and Google Scholar databases. Only articles published or translated into the English language were considered, and key data from the full article of each paper was extracted and evaluated.
Results
The authors’ search yielded 29 articles. A total of 686 patients with a mean age of 33.4 years (range 14–73 years) were included. Blurring of vision was the most common presenting symptom followed by scotoma. Ocular findings were mostly seen in the posterior pole of the fundus, manifesting as retinal hemorrhages, macular edema, foveolitis, vasculitis, and optic neuropathy. Most patients with dengue-related ophthalmic complications recover spontaneously without any treatment. Patients with severe visual loss or bilateral involvement were treated with systemic steroids and occasionally immunoglobulins. Prognosis of dengue-related ophthalmic complications is favorable; almost all patients had normal or showed improvement in visual acuity and complete resolution of dengue ophthalmic complications was noted in almost all cases.
Conclusion
The pathological process of dengue ophthalmic complications is complex and clinical manifestations varied. Ophthalmic complications are usually seen in young adults who often present at the nadir of thrombocytopenia. Despite good recovery of vision and resolution of clinical signs in most patients, ophthalmologists and physicians should be aware and vigilant as isolated reports of cases of dengue ophthalmic complications with poor visual acuity refractory to treatment have been reported.
Keywords: Blurring of vision, Complications, Dengue, Maculopathy, Ocular, Ophthalmic, Retinal hemorrhage, Scotoma, Treatment
Introduction
Dengue fever is a mosquito borne disease that is commonly found in the tropics [1]. Dengue virus belongs to the Flavivirus genus of the family, Flaviviridae, and its members include the four antigenically-related serotypes of dengue virus (DENV 1–4). It is transmitted to humans by the bite of an infected female Aedes mosquito, usually the Aedes aegypti mosquito.
Dengue infection is characterized by an acute onset of fever associated with symptoms of malaise, sore throat, rhinitis and cough, headache, muscle ache, retro-orbital pain, joint pain, abdominal discomfort, and rash [1]. Other clinical manifestations of dengue are related to the bleeding diathesis from thrombocytopenia. Dengue infection is usually a clinical diagnosis but can be confirmed with laboratory tests based on the time of presentation; frequently used tests include polymerase chain reaction (PCR), and immunoglobulin M (IgM) or immunoglobulin G (IgG) enzyme immunoassays [1]. During the early phase of the infection, when febrile illness is within 5 days, dengue PCR is performed. If febrile illness exceeds 5 days, the preferred tests are dengue IgM and IgG tests. It is well documented that serology is negative during the febrile phase and early infection, becoming positive after the fever settles [2, 3]. In contrast, PCR has a much higher sensitivity during the febrile phase, becoming negative after fever settles [2, 3].
Dengue is usually a self-limiting infection. Recovery from infection with one serotype provides lifelong immunity against that serotype, but confers only transient and partial immunity against subsequent infection by other serotypes [4]. Sequential infections with other serotypes may increase the risk of more serious systemic disease, such as dengue hemorrhagic fever or dengue shock syndrome, which are life-threatening [4].
Since the beginning of the new millennium, there have been an increasing number of reports describing a myriad of ocular signs and symptoms associated with dengue fever [5–11]. The precise pathophysiologic mechanism of dengue ophthalmic complications is not well understood; however, many studies have alluded to the possibility of an immune-mediated process as a likely mechanism [10–12]. In this paper, the authors aim to review the ocular manifestations, utility of diagnostic tests, management, prognosis, and sequelae of dengue-related ocular complications.
Materials and Methods
A comprehensive literature search was conducted on Medline, PubMed, and Google Scholar databases in October 2011. Search temporal limits included articles published from 1929 to October 2011 with the purpose of providing the most recent evidence. Studies were queried using the following keywords in various combinations: “dengue,” “ocular,” and “ophthalmic complications.” Articles included for the review provided a description of dengue-related ophthalmic complications, its clinical course, management, and visual outcome. Only articles published in the English language were considered. Articles, such as preliminary reports and abstracts, were excluded as they did not have descriptive details available.
Results
Population Characteristics
Table 1 [13–33] summarizes the details of dengue-related ophthalmic complications in the 29 articles that were included for the purpose of this review. There were 14 case reports and 15 case series. A total of 686 patients were included in the authors’ review; there were 401/686 (58.5%) males and 285/686 (41.5%) females with a mean age of 33.4 years (range 14–73 years). Cases from Singapore formed the majority, with 608/686 (88.3%) patients, followed by 67/686 (9.8%) from India. Some of the case series published from Singapore were from the same institution and it was not possible to know whether they were reporting different aspects of the same group of patients. For the purpose of this review, the authors have assumed that multiple case series from the same institution were of different patients. The mean time interval when patients presented with ocular symptoms after the onset of dengue fever was 7 days (range 1–28 days). Presentation of dengue-related ocular signs and symptoms often corresponds to the nadir of thrombocytopenia [10, 20]. A delay in the onset of uveitis, 3–5 months after dengue infection, which was confirmed with positive dengue IgM, has also been reported [30].
Table 1.
Summary of ophthalmic complications in dengue fever
| Paper | Design | No of cases/gender | Interval | Ocular symptoms | Ocular signs | Investigations performed | Treatment | Follow-up | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Haritoglou et al. [5] | Case report | 1/F | 1 day |
BOV BE; VA 6/150 BE; color vision severely affected |
Small hemorrhages at NFL; exudative maculopathy BE |
- Electrophysiological exam: • Prolonged latencies • Reduced amplitude of visually evoked cortical responses • Mild reduction of amplitudes in mfERG BE - Arden color contrast test: Abnormal |
No treatment | 8 weeks | VA improved: RE 6/30 LE 6/9.5 |
| Yamamoto et al. [13] | Case report | 1/M | 24 days |
BOV BE; VA CF BE |
Fundoscopy was normal; Optic neuropathy suspected as cause of visual disturbance |
- MRI brain: no abnormalities in the optic nerves, cerebellum and cerebrum - MRI spine: multiple high-intensity spotty lesions from Th-7 to Th-11 - Lumbar puncture: mild elevation of protein and pleocytosis |
IVMP | NA | Mild visual disturbance BE |
| Cruz-Villegas et al. [14] | Case report | 1/M | 3 days |
BOV BE; VA: RE 6/24 LE 6/120; scotomas BE; ocular pain BE |
AC cells BE; AC shallow BE; Extensive bilateral choroidal effusions |
- CT brain and MRI brain: normal - Lumbar puncture: negative |
Topical prednisolone | 1 week |
VA 6/6 BE; AC deeper with trace of cells; choroidal effusions subsided |
| Lim et al. 2004 [6] | Case series | 6/M:F 1:5 | 6.8 days |
n = 11 eyes BOV (90.9%); VA range from 6/6 to HM; scotomas (36.4%) |
n = 11 eyes AC cells (18.2%); vitreous cells (18.2%); RPE changes (27.3%); RPE discoloration (9.1%); retinal hemorrhage (36.4%); retinal vasculitis (9.1%); intraretinal white lesions (18.2%); macular edema (54.5%) |
n = 11 eyes - FFA • Arteriolar focal knobby hyperfluorescence in the macula with mild vascular wall staining and leakage (27.3%) • Early hyperfluorescent spots at the level of the RPE (36.4%) • Transmission defects (36.4%) - ICG • Diffuse choroidal hyperfluorescence (81.8%) - HVF and Amsler chart: central scotoma (9.1%) |
No treatment (1 case); steroid therapy (1 topical, 2 periocular, 2 oral) |
2 weeks– 4 months |
RPE discoloration over affected areas; partial recovery of VA (3 cases); VA stable (3 cases) |
| Siqueira et al. [7] | Case report | 1/F | 13 days |
BOV BE; VA: RE 6/30 LE 6/60 |
No AC or vitreous cells BE; pre-retinal hemorrhages at equator; CWS at macula; peripheral vascular sheathing BE |
- FFA: areas of capillary nonperfusion in both the equator and macula. - MRI brain and carotid Doppler studies: normal |
Oral anti-platelet therapy; LE Pars plana vitrectomy; RE PRP |
2 years |
Poor visual acuity in LE; no further retinal vasculitis |
| Nainiwal et al. [9] | Case report | 1/F | 2 days |
BOV BE; VA: RE PL LE 6/18 |
Vitreous hemorrhage BE | NA | Initially conservative; RE pars plana vitrectomy | 7 months |
VA improved; VA 6/12 BE |
| Chlebicki et al. [8] | Case series | 4/M:F 1:3 | 6.25 days |
n = 4 cases BOV (100%); VA reduced (100%); metamorphopsia (25%) |
n = 4 cases Blot hemorrhages within the vascular arcades BE (100%) |
NA |
Standard supportive care (4 cases); platelet transfusion (2 cases) |
NA | Complete resolution within 2 days (3 cases); reduced VA & metamorphopsia after 2 months (1 case) |
| Mehta [15] | Case series | 5/M:F 4:1 | NA |
n = 5 cases VA 6/6 (20%); rest had no VA done |
n = 10 eyes SCH (60%); roth spots (10%); intraretinal hemorrhage (60%); yellow thickening in choroid & retina (40%) |
NA | NA | NA | NA |
| Preechawat et al. [16] | Case report | 1/M | 10 days |
BOV BE; VA CF BE |
Flame-shaped hemorrhage at fovea RE; mild bilateral optic disc hyperemia |
- FFA: no disc leakage - GVF: bilateral cecocentral scotomas - Lumbar puncture, brain and orbit MRI: all normal |
IVMP followed by OPNL | 26 months |
VA: 6/6 BE; color vision: normal |
| Habot-Wilner et al. [17] | Case report | 1/M | 2 days |
VA 6/6 BE; eyelid edema BE; conjunctival irritation BE; scotoma in central VF BE |
Vitreous cells RE; retinal infiltrate with central dot hemorrhages and microhemorrhages infernosal to fovea of RE; macula edema RE; dot hemorrhage macula of LE |
- Fundoscopy: optic disc normal BE - FFA: no retinal or choroidal leakage or staining |
NA | 1 month |
VA: 6/6 BE Fundocopy: normal BE Scotoma resolved |
| Chan et al. [10] | Case series | 13/M:F 6:7 | 7 days |
n = 13 cases BOV (100%); VA range from 6/7.5 to CF; Scotomas (92.3%) |
n = 13 cases Anterior uveitis (7.7%); retinal vasculitis (30.8%); exudative retinal detachment (15.4%); macular edema (76.9%); blot hemorrhages at macula (69.2%); perifoveal telangectasia and CWS (7.7%) |
n = 13 cases - FFA: extensive fluid leakage from retinal vessels (30.8%) - HVF and Amsler chart: central scotomas (100%) - OCT: thickening of the macula (30.8%) |
Conservative (11 cases); OPNL (1 case); IVMP followed by OPNL (1 case); topical prednisolone (1 case) |
2–20 weeks | Better than VA 6/9 (3 cases); central scotoma (13 cases); macular edema resolved (8 cases); macular edema improved (2 cases) |
| Kapoor et al. [18] | Case series | 54/M 63.4% | NA |
n = 54 cases Retrobulbar pain (11.1%) |
n = 108 eyes SCH (76.9%); CWS (27.8%); dilatation and tortuosity of vessels (37.0%); isolated retinal hemorrhages (46.3%); superficial retinal hemorrhage sparing the macula with hard exudates and CWS (27.8%) |
NA | No treatment | 2–8 weeks | SCH resolved (16 cases); posterior segment findings resolved (6 cases) |
| Garcia et al. [19] | Case report | 1/M | 8 days |
BOV BE; VA: RE 6/15 LE 6/9; retrobulbar pain |
Vitritis BE; macular star exudates BE; optic disc swelling BE; optic disc hemorrhage BE; papillitis with areas of serous detachment in the posterior pole and vascular arcades BE |
- Nuclear magnetic resonance of cranium and orbits: normal - HVF • Increased blind spot BE • Islands of sensitivity loss in the upper nasal and lower temporal regions of RE |
No treatment | 2 months | VA 6/6 BE; neuroretinitis resolved; disappearance of perimetric alterations |
| Teoh et al. [20] | Case series | 50/M:F 34:16 | 7 days |
n = 50 cases BOV (60%); VA range from 6/6 to CF central scotoma (30%); micropsia/metamorphopsia (4%); VF defect (2%); floaters (6%); near visual disturbance (6%); redness (2%); |
n = 65 eyes SCH (4.6%); anterior uveitis (7.7%); intermediate uveitis (12.3%); posterior vitreous cells (10.8%); retinal vasculitis (23%); macular edema (77%); macular hemorrhage (69%); optic neuritis (1.5%); optic disc swelling (3.1%) |
n = 65 eyes - OCT: foveal elevation (33.8%) - HVF and Amsler chart: central scotoma (39%) |
Conservative (37 cases); OPNL (6 cases); IVMP followed by OPNL (7 cases); topical prednisolone (5 cases) |
1 year |
n = 50 cases VA 6/12 or better in 3 months (76%); and at 1 year (86.2%); 11 eyes from 7 patients (17%) who received IVMP had vision remaining between 6/12 to 6/60; persistent scotoma at 3 months (80%) and at 1 year (6%) |
| Seet et al. [21] | Case series | 156/M:F 89:67 | 4.6 days |
n = 156 cases Eye strain (29.5%); retro-ocular pain (19.9%); BOV (10.3%); double vision (3.2%); foreign body sensation (3.2%); eye flashes (1.9%); floaters (1.3%) |
n = 156 cases Retinal hemorrhages (1.3%) |
- Slit-lamp examination: normal - Fundoscopy: normal |
NA | NA | NA |
| Chang et al. [22] | Case report | 1/F | 7 days |
BOV BE; VA 6/120 BE |
Mild vitreous hemorrhage BE; disc hemorrhage and swelling BE; retinal hemorrhage and vasculitis BE; sheathing of macular arterioles BE; macular detachment BE |
- FFA: bilateral macular arteriolar leakage | IVMP followed by IVIG, followed by IVMP and OPNL | 1 week | VA: 6/12 BE |
| Tan et al. [23] | Case report | 1/M | 8 days |
BOV BE; VA: RE 6/30 LE 6/50; reduced colour vision |
Flame and blot hemorrhages in posterior pole BE; soft exudates and macula ischemia; hyperemic optic discs; dilated veins |
- FFA: no leakages - ICG: spots of hyperfluorescence |
High dose steroids | NA | VA and color vision improved markedly |
| Bacsal et al. [11] | Case series | 41/M:F 17:24 | 6.9 days |
n = 71 eyes BOV (87%); VA range from 6/6 to HM; scotomas (63%); floaters (1%) |
n = 71 eyes AC cells (17%); vitreous cells (31%); both anterior and vitreous cells (11%); vitreous hemorrhage (1%); RPE mottling (17%); intraretinal precipitates (1%); yellow subretinal dots (28%); arteriolar sheathing (4%); venular sheathing (45%); retinal hemorrhage (45%); optic disc hyperemia (14%); optic disc edema (11%); foveal swelling (15%) |
n = 71 eyes - FFA • Arteriolar leakage (3%) • Venular occlusion (25%) • Venular leakage (13%) - ICG: • Early large-vessel hyperfluorescence (31%) • Mid to late hypofluorescent spots (29%) - HVF: central or paracentral scotomas (63%) - OCT: • Exudative RD (10%) • RPE thickening at the fovea (26%) • RPE atrophy (2%) - Amsler chart: bilateral large dense central scotomas (2.8%) |
n = 41 cases Steroid therapy (28 cases): - IVMP followed by OPNL (12 cases) - OPNL (11 cases) - IVIG with IV hydrocortisone & OPNL (3 cases) - Periocular methylprednisolone (10 eyes) - Intravitreal triamcinolone acetonide (2 eyes) - Topical prednisolone acetate (1 eye) |
5.4 months |
n = 71 eyes Improvement in VA (100%); 52.1% of eyes at initial follow-up improved to better than 6/12 vision, followed by 85.9% of eyes at final follow-up |
| Su et al. [12] | Case series | 197/M:F 119:78 | 6.8 days |
BOV; VA range from 6/6 to 6/36; scotomas; visual complaints |
Maculopathy (27 eyes); white spots at macula (15 eyes); yellow spots at macula (3 eyes); PED (1 eye); vascular sheathing (1 eye); RPE mottling (4 eyes); hyperemic optic disc (2 eyes); swollen optic disc (1 eye); optic disc hemorrhages (1 eye) |
- FFA: mild anteriolar and/or venular leakage in some eyes - ICG: hypofluorescence in mid and late phases in some areas - OCT: outer neurosensory retina/RPE thickening at fovea (1 case) - Amsler chart: abnormalities noted |
NA | NA | NA |
| Tan et al. [24] | Case report | 1/F | 6 days |
BOV BE; VA: RE 6/120 LE CF; metamorphopsia BE |
Yellowish retinal infiltrates BE; extensive retinal vasculitis in the macula BE complicated by BRVO RE; macular edema BE; blot hemorrhages at macula BE |
- FFA: leakage indicative of panretinal vasculitis. Follow-up FFA at 10 weeks showed retinal capillary nonperfusion at the infero-nasal margin of the foveal avascular zone - OCT: central foveal thickening - Amsler chart: distortion in RE |
Platelet transfusion; conservative treatment otherwise |
10 weeks |
VA 6/6; No residual inflammation or macular edema; RE has mild red desaturation and visual distortion on Amsler grid monitoring |
| Beral et al. [25] | Case series | 3/M:F 2:1 |
1 month (2 cases); 15 days (1 case) |
n = 6 eyes impaired vision (83.3%); VA range from 20/20 to HM; diffuse orbital pain (33.3%) |
n = 6 eyes Nasal parapapillary hemorrhage (33.3%); Optic disc swelling (83.3%) |
- VF testing: severe global loss of contrast sensitivity - MRI brain: normal - Lumbar puncture: normal |
IVMP | NA |
VA: RE 6/15 LE PL (1 case); VA: RE 6/9 LE 6/7.5; inferior scotoma and enlargement of the blind spot BE; residual temporal atrophy of both optic nerves; color vision tests no residual abnormality (1 case); worsening of VA to HM (1 case) |
| Filho et al. [26] | Case report | 1/F | 3 days |
Impaired vision BE; VA HM BE; intense ocular pain; lacrimation; photophobia; redness; raised IOP |
Corneal edema; shallow AC; iris atrophy; fixed and moderately dilated pupils BE; both crystalline lenses exhibited nuclear sclerosis 2 + and glaucomflecken |
- Gonioscopy: closed angles - Fundoscopy: not clear - B scan ultrasonography: normal posterior segments BE - CT head: normal |
Medical treatment followed by bilateral laser iridotomies | 1 month |
VA: 6/60 BE; IOP normalized; no significant alterations on eye fundus exploration without dilatation |
| Kanugo et al. [27] | Case report | 1/F | 7 days |
BOV; VA 6/6 BE; RE inferior visual field defect; ocular pain |
CWS LE; BRAO RE |
- FFA: • Midphase narrowing of the affected arterial segment RE • Late phase staining and leakage of the occluded artery RE - Kinetic central field charting with Bjerrum’s screen: infero-nasal field defect RE |
NA | 3 months |
VA 6/6 BE; persistent inferior field defect RE |
| Loh et al. [28] | Case series | 6/M:F 4:2 |
5–7 (8 eyes); 9 (2 eyes) |
n = 10 eyes BOV (80%); VA range from 6/7.5 to CF; central scotoma (90%) |
n = 10 eyes AC cells (20%); CWS (20%); venular sheathing (30%); BRVO (20%); blot hemorrhages (50%); retinal striae (20%); yellow-orange lesion at fovea (100%); macular edema (20%) |
n = 10 eyes - FFA: early hypofluorescence that persisted in the late phase at the fovea (30%) - Electrophysiological exam: mfERG-decreased foveal and parafoveal responses (100%) - OCT: • Outer neurosensory retina disruption (100%) • Elevation of fovea (20%) |
IVMP followed by OPNL (1 case); OPNL (2 cases); IVIG (2 cases); periocular depomedrol (2 eyes); periocular traicinolone acetonide (1 eye); no treatment (1 eye) |
9.7 months |
n = 10 eyes 6/6 by 3 months (60%); 6/6 by 5 months (10%); 6/7.5 by 3 months (10%); 6/7.5 by 1 year 3 months (10%); 6/12 with persistent yellow-orange lesion at fovea at 3 months (10%) |
| Sanjay et al. [29] | Case series | 3/M:F 1:2 | 5–7 |
n = 6 eyes BOV (50%); VA range from 6/6 to CF; impaired color vision (16.7%); scotomas (33.3%); enlarged blindspot (16.7%) |
n = 6 eyes Retinal edema (16.7%); retinal hemorrhages (66.7%); CWS (66.7%); optic disc swelling (66.7%); optic disc atrophy (16.7%) |
n = 6 eyes - Electrophysiological exam: • mfERG-centrocecal scotoma (16.7%) • pVEP-delayed P100 latency (16.7%) and absent response (16.7%) - MRI: edema of optic nerve sheath complex (16.7%) - HVF: • Central scotoma (16.7%) • Paracentral scotoma (33.3%) • Enlarged blind spot (16.7%) |
IVMP followed by OPNL (1 case) | 6 weeks–1 year |
VA 6/9 with impaired color vision and paracentral scotoma (1 eye); NPL RE and resolved VF defects in LE (1 case); VA 6/6 with signs and symptoms completely resolved (1 case) |
| Gupta et al. [30] | Case series | 6/M:F 2:4 | 3–5 months |
n = 7 eyes BOV (100%); VA range from 6/12 to CF; ocular pain (42.9%); redness (28.6%) |
n = 7 eyes Ciliary congestion (42.9%) anterior uveitis (85.7%); vitritis (14.3%); retinal vasculitis (14.3%); macular edema (14.3%) |
n = 7 eyes - FFA: vasculitis and retinal hemorrhages in perimacular region (14.3%) - OCT: macular edema (14.3%) |
OPNL and topical medications (steroids and ocular hypotensive medications) | 3–5 months |
All responded to treatment: 6/9 in 5 eyes; 6/24 and 6/18 in other 2 eyes due to cataract |
| Quek et al. [31] | Case report | 1/F | 7 days; 5 daysa |
1st infection: BOV BE; VA: RE 6/120 LE CF; metamorphopsia BE Recurrent infection: BOV BE; VA 6/6 BE; scotomas RE |
1st infection: Posterior uveitis; flame-shaped hemorrhages; CWS at macula; vascular sheathing at macula Recurrent infection: mild macular edema |
1st infection: - FFA: • Vascular leakage in all quadrants • Retinal periphlebitis with right macular BRVO and macular edema - OCT: cystic edema BE |
Conservative treatment | 6 months; 2 years |
1st infection: Vision and metamorphopsia improved; VA 6/6 BE; posterior uveitis and vasculitis resolved; macular edema resolved; persistent, non-progressive paracentral relative scotoma Recurrent infection: symptoms resolved; scotoma persisted |
| Chee et al. [32] | Case series | 87/M:F 59:28 | 6.2 days | Normal VA | None |
- Amsler chart: normal - Fundoscopy: normal - Slit lamp: normal |
NA | 14 days | No change |
| Teoh et al. 2010 [33] | Case series | 41/M:F 22:19 | 7 days |
n = 41 cases BOV (51.2%); VA ≥6/24 (41.9% of affected eyes); <6/24 (50% of affected eyes); scotomas (34.1%); floaters (4.9%); micropsia (4.9%); Near vision disturbance (4.9%) |
n = 41 cases Anterior uveitis (7.3%); intermediate uveitis (4.9%); optic neuritis (2.4%) |
n = 74 eyes - OCT • Diffuse oedema (44.6%) • Macular oedema (21.6%) • Cystic foveolitis (33.8%) - Amsler chart: relative scotomas (91.9%) |
NA | 2 years |
VA < 6/24 (50% of affected eyes at presentation and 2.7% after 2 years) 59.5% of affected eyes retained a persistent relative central/paracentral scotomata even after 2 years, but only in 1.4% was it visually disturbing. |
AC anterior chamber, BE both eyes, BOV blurring of vision, BRAO branch retinal artery occlusion, BRVO branch retinal vein occlusion, CF counting fingers, CT computed tomography, CWS cotton wool spots, F female, FFA fundus fluorescein angiography, GVF Goldmann visual field, HM hand movement, HVF Humphrey visual field, ICG indocyanine green, IOP intraocular pressure, IV intravenous, IVIG intravenous immunoglobulin, IVMP intravenous methylprednisolone, LE left eye, M male, mfERG multifocal electroretinogram, MRI magnetic resonance imaging, NA Not applicable/Not available, NFL nerve fiber layer, NPL no perception of light, OCT optical coherence tomography, OPNL oral prednisolone, PED pigment epithelial detachment, PL perception to light, PRP panretinal photocoagulation, pVEP pattern visual evoked potential, RD retinal detachment, RE right eye, RPE retinal pigment epithelium, SCH subconjunctival hemorrhage, Th thoracic vertebrae, VA visual acuity, VF visual field
aCase of recurrent bilateral dengue maculopathy following two sequential infections
Diagnosis of Dengue Infection
The diagnosis of dengue fever is based on clinical features and laboratory parameters. Serological tests were carried out in most of the studies with the majority of dengue infection confirmed by IgM, followed by IgG and PCR. A study by Chee et al. compared the prevailing dengue serotype of the population during the epidemics in 2005 and 2007, and found that the predominant serotype in Singapore was DENV-1 and DENV-2, respectively [32, 34, 35]. Interestingly, none of the patients in the 2007 cohort had dengue-related ophthalmic complications, whereas 10% of patients in the 2005 cohort had dengue-related maculopathy. Only four case series had the diagnosis of dengue established based on characteristic clinical signs and presumed because of the typical clinical picture and proximity of their living environment to known clusters of infected individuals [11, 12, 15, 28].
Ophthalmic Symptoms of Dengue-Related Complications
Blurring of Vision
The most common complaint was blurring of vision. In three case series involving 23 patients, all of them complained of blurring of vision with visual acuity ranging from 6.0/7.5 to counting fingers in two of the studies [8, 10, 30]. Three studies conducted in Singapore showed that blurring of vision was the most common complaint in patients with dengue fever [6, 20, 33]. Patients with dengue-related maculopathy were more likely to have vision worse than LogMar 0.15 (P = 0.005) [12]. As much as 51.2% of 41 patients with dengue-related maculopathy had blurring of vision [11]. One study compared the degree of blurring of vision with the type of maculopathy, and found that patients with cystoid macular edema had poorer visual acuity, and the degree of visual loss and prognosis correlated with the amount of macular edema [33].
Scotoma
The next most common symptom experienced by patients with dengue-related ophthalmic complications is central scotoma. In the case series by Chan et al. [10], 12 out of 13 patients had central scotoma in association with blurring of vision. The areas of scotoma corresponded to the areas of edema and hemorrhage in the macula [32]. However, not all patients with dengue-related maculopathy presented with scotoma. In one study of 50 patients with dengue fever, the majority presented with macular hemorrhage (69.2%) and macular edema (76.9%); however, only 15 out of 50 (30.0%) presented with scotoma [20]. In another study, scotoma was present in 14 out of 41 patients (34.1%) with dengue-related maculopathy [11].
Ocular Pain
There were 8 out of 29 papers that described ocular pain as a presenting symptom [14, 18, 19, 21, 25–27, 30]. Three of them described the location of pain as retrobulbar and one described it as a diffuse pain in 33.3% of patients [18, 19, 21, 25]. The patients with retrobulbar pain consisted of those who presented with subconjunctival hemorrhage and retinopathy sparing the macula [18], stellar neuroretinitis [19], and retinal hemorrhages [21].
Other Symptoms
Metamorphopsia was reported in six patients [8, 24, 31] and micropsia in four patients [20, 33]. Impairment of color vision had been reported in patients with optic neuropathy [24] and maculopathy [5, 29]. Floaters were less common, occurring between 1% and 6% [11, 20, 21, 33]. Redness was the least common symptom and was reported in four patients, two of which had uveitis [30] and one had angle closure glaucoma [26].
Ocular Complications Involving the Anterior Segment of the Eye
Subconjunctival Hemorrhage
A study by Kapoor et al. accounted for the majority of cases of dengue-related subconjunctival hemorrhage, and in the 50 patients with subconjunctival hemorrhage, 42 (84%, n = 50) patients had petechial hemorrhages present in the conjunctivae and eight (16%, n = 50) patients had diffuse hemorrhages noted in one to four quadrants [18]. Another study in India reported subconjunctival hemorrhage as the only anterior segment finding in three out of five patients with dengue hemorrhagic fever [15]. One other study reported subconjunctival hemorrhage present in 3 eyes of 50 patients (65 eyes) diagnosed with dengue fever and had visual symptoms [20].
Uveitis
Patients with dengue infection rarely presented with uveitis. A case series by Gupta et al. [30] reported dengue-related uveitis in six patients, with five isolated in the anterior chamber and only one with panuveitis. Another case series of 41 patients with dengue-related ocular signs and symptoms had anterior uveitis in 12 eyes (17%), vitritis in 22 eyes (31%), and panuveitis in eight eyes (11%) [11]. Most case series report a small percentage of patients with uveitis. A series of 62 patients with dengue-related visual complaints reported three patients with anterior uveitis and two with intermediate uveitis [33]. Anterior uveitis, intermediate uveitis, and vitritis were present in 5, 8, and 7 of 65 eyes (50 patients), respectively, in patients with dengue-related visual complaints [20]. Lim et al. [6], Chan et al. [10], and Loh et al. [28] reported anterior uveitis in only 1 patient out of their case series of 6, 13, and 6 patients, respectively.
Other Anterior Segment Signs
There were two case reports on patients with dengue-related shallow anterior chamber [14, 26]. The intraocular pressure was normal in the patient with bilateral choroidal effusions but was elevated in the other patient with angle closure glaucoma. Ciliary congestion was noted in two out of six patients with uveitis [30].
Ocular Complications Involving the Posterior Segment of the Eye
Maculopathy
Hemorrhages associated with dengue-related maculopathy are mostly intraretinal and can take the form of dot, blot, or flame-shaped hemorrhages. In a case series of 41 patients (71 eyes) with dengue-related maculopathy, 32 eyes (45%) presented with intraretinal hemorrhages mostly in association with venous sheathing [11]. Similar findings of intraretinal and flame-shaped hemorrhages were also reported [33]. Macular hemorrhage was the second commonest presentation of dengue-related ocular sign, affecting 45 of 65 eyes (69.2%) in another case series of patients in Singapore [20]. Bilateral blot hemorrhages in the macula of four patients were the only ocular sign associated with dengue fever in the series by Chlebicki et al. [8]. Vascular sheathing [6, 11, 28, 31] and vasculitis [6, 10, 20, 24] were often found in association with macular hemorrhage.
Dengue-related foveolitis refers to the yellow-orange lesion at the fovea of patients with dengue maculopathy, which corresponds to a disruption of the outer neurosensory retina in optical coherence tomography (OCT) [28]. It was formally described by Loh et al. [28] in 10 eyes of 6 patients and the term foveolitis was coined. Previously, Bacsal et al. and Su et al. [11, 12] had reported similar findings of yellow subretinal dots in 20 of 71 eyes (28%) and 3 of 27 eyes (11%), respectively. The fundus photo (Fig. 1) of the authors’ patient exhibited foveolitis as evidenced by an orange lesion at the fovea. This patient also had blot hemorrhages and cotton wool spots mainly in the posterior pole.
Fig. 1.
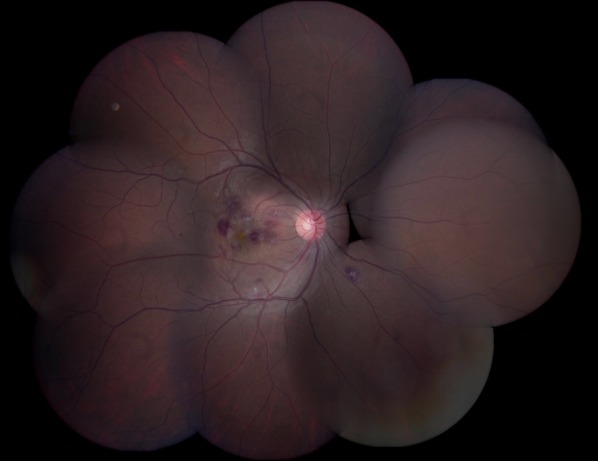
A fundus photo of a patient who had dengue fever and blurring of vision in the right eye showed intraretinal hemorrhage, cotton wool spots, macular edema confined to the macula, and a yellow-orange spot at the fovea
Macular Edema
Dengue-related maculopathy commonly presents with macular edema [10, 20, 33]. One series by Teoh et al. [33] further categorized the type of macular edema based on their appearance on OCT. The three patterns of macular edema on OCT include type 1, which is diffuse edema, type 2, which is cystoid edema, and type 3, which is cystic foveolitis. There are also isolated case reports of patients with dengue-related macular edema [5, 17, 24, 31].
Optic Neuropathy
Optic disc swelling, hyperemia, and disc hemorrhages are common presentations of dengue-related optic neuropathy. Only one patient with optic disc swelling progressed to develop optic atrophy with a visual acuity of no light perception [29]. Case series by Beral et al. and Sanjay et al. [25, 29] described six patients (nine eyes) with optic disc swelling with visual acuity ranging from 6/6 to no light perception. Optic neuropathy is relatively uncommon compared to other dengue-related ocular signs. Optic disc swelling and hyperemia were less common findings, accounting for 14% and 11%, respectively, in the group of patients with dengue-related maculopathy [11]. The series by Teoh et al. [20] reported disc swelling in only 3.1% (2 of 65 eyes) of eyes with dengue-related ophthalmic complications.
Other Posterior Segment Signs
Other less common dengue-related ocular signs include vitreous hemorrhage, which was reported in three studies [9, 11, 22]. Vascular occlusions were reported in four studies and mainly consisted of vein occlusions [24, 27, 28, 31]. Only one out of the four studies reported arterial occlusion of the superotemporal macular branch [27].
Investigations
Ophthalmic investigations were performed mostly for posterior segment pathology. The Amsler grid test was used to detect scotomas in patients with dengue-related maculopathy. A relative central scotoma was demonstrated on the Amsler chart in 25 out of 65 eyes (39%) in the series by Teoh et al. [20] and as much as 12 of 13 patients (92.3%) in the study by Chan et al. [10], both of which correspond to visual field testing by an automated Humphrey field analyzer. In the study by Su et al. [12], the Amsler grid test abnormalities were more likely to occur in patients with dengue maculopathy (P = 0.001).
Fundus fluorescein angiography (FFA) demonstrated mainly vascular occlusion or leakage, and has aided in the diagnosis of vein occlusions [11, 31] and vasculitis [24, 30, 31]. In a study of 41 patients (71 eyes) with dengue-related ocular signs and symptoms, FFA picked up venular occlusion in 25% of eyes and vascular (arteriolar/venular) leakage in 16% of eyes [11]. Indocyanine green angiography (ICG) was less commonly performed. Su et al. [12] reported hypofluorescence on ICG, which corresponded to white or yellow dots in the macula. This finding was similar to the study by Bacsal et al. [11] who noted that 50% of yellow subretinal dots in the macula corresponded to hypofluorescent spots on ICG. A case series of six patients with a decrease in visual acuity related to dengue infection demonstrated diffuse hyperfluorescence on ICG with late silhouetting of larger choroidal vessels in four patients [6].
OCT imaging of the macula has been employed in a number of studies to evaluate retinal thickness and morphology. Foveolitis is a term used to describe the presence of a yellow-orange lesion at the fovea, which corresponds to an area of disruption to the outer retina of the fovea in OCT [28]. Teoh et al. [33] used OCT to characterize the type of retinal thickening (diffuse/cystoid/cystic foveolitis) and correlated it with visual acuity and prognosis.
Electrophysiology tests were less commonly performed and the results were reported in three studies [5, 28, 29]. Multifocal electroretinography (mfERG) showed decreased foveal or parafoveal responses in all 10 eyes of the 6 patients studied [28]. One case report also demonstrated a decrease in amplitude of mfERG [5]. In a study by Sanjay et al. [29] on dengue-related optic neuropathy, the pattern visual evoked potential (pVEP) revealed a delayed P100 latency in one eye (one patient) and a centrocecal scotoma on mfERG. The other patient had a reduced N95:P50 ratio with no response on pVEP of the right eye [29].
Lumbar puncture was performed in four studies [13, 14, 16, 25] with only one showing abnormal results of mildly elevated protein and pleocytosis [13]. Brain imaging was performed in four studies and they were all normal [13, 14, 25, 26]. A magnetic resonance imaging examination of the spine in one patient with acute disseminated encephalomyelitis following dengue fever showed multiple high-intensity spotty lesions on thoracic vertebrae T7–11 [13]. In total, 4 out of 28 studies did not report any ophthalmic investigation or neuroimaging [8, 9, 15, 18].
Treatment
Steroid Therapy
Steroids were the mainstay of treatment in patients who were persistently symptomatic and had poor vision due to dengue-related ocular complications. However, a large number of patients had dengue-related ocular disease that was self-limiting and resolved spontaneously without any treatment. Teoh et al. [20] reported that 37 out of 50 patients with dengue-related ocular symptoms had spontaneous resolution of clinical signs without any treatment. In another series by Chan et al. [10], 11 out of 13 patients were treated conservatively with spontaneous resolution of maculopathy upon recovery from thrombocytopenia. In the study conducted in East India, 50 out of 134 patients hospitalized for dengue fever had ocular complications that resolved spontaneously without any treatment [18]. Figure 2 shows spontaneous and complete resolution of dengue-related retinopathy and foveolitis 4 weeks after onset of dengue maculopathy without any treatment.
Fig. 2.

A fundus photo of the right eye in the same patient as in Fig. 1 showing spontaneous and complete resolution of posterior segment findings after 4 weeks without any treatment
Steroids can be administered topically or systemically depending on ocular involvement. Topical prednisolone was administered in patients with dengue-related uveitis [20, 30]. In a study by Bacsal et al. [11], 11 out of 28 patients who received treatment for dengue-related ocular complications were given oral prednisolone (1 mg/kg) alone and tapered according to clinical response. Intravenous methylprednisolone was given to 12 out of 28 patients who had visual acuity worse than 6/60 or who did not respond to initial treatment with oral prednisolone [11]. Patients with unilateral disease were treated with periocular methylprednisolone injections in 10 eyes [11]. Intravenous methylprednisolone was also administered to another 7 patients (11 eyes) who had extensive macular and panretinal vasculitis [20]. In 3 out of 10 patients with dengue-related maculopathy and visual acuity of 6/120 or worse in at least one eye, intravenous methylprednisolone was administered together with intravenous immunoglobulin in two out of three patients [28]. Intravenous methylprednisolone was also administered in four other isolated case reports [13, 16, 22, 25].
The visual outcome of dengue ophthalmic complications following treatment with systemic steroids in the form of intravenous or oral prednisolone is favorable. Only 2 out of 25 eyes of patients that received oral prednisolone did not show much improvement in visual acuity [6]. One out of the two patients had deterioration of vision and was lost to follow-up, whilst the other had only subjective improvement in vision with best corrected visual acuity unchanged at 20/30 in the right and 20/20 in the left eye [6]. Most patients treated with intravenous methylprednisolone had marked improvement of visual acuity, with 12 out of 27 patients (44.4%) having persistent poor visual outcome [11, 20, 25, 29]. In the study by Teoh et al. [20], 11 eyes of 7 patients with extensive panretinal and macular vasculitis had vision that remained between 6/12 and 6/60, despite treatment with intravenous methylprednisolone. Only 3 out of 27 patients with dengue-related optic neuropathy showed deterioration of vision after treatment [25, 29].
Other Ocular Interventions
Intravenous immunoglobulin was administered to six patients because of poor or worsening visual acuity that did not respond to initial intravenous methylprednisolone and oral prednisolone [11, 22, 28]. Visual outcome following intravenous immunoglobulin treatment was generally favorable with four out of six patients reported to have marked improvement of visual acuity [11, 22, 28].
Two patients underwent pars plana vitrectomy; one for vitreous hemorrhage in the right eye [9] and the other for retinal hemorrhage from preretinal neovascularization secondary to retinal capillary occlusion in the left eye [7]. Pan retinal photocoagulation was performed in the right eye of one patient for treatment of worsening vitreous hemorrhage [7]. Another patient underwent bilateral laser iridotomies for angle closure glaucoma [26].
Systemic Supportive Treatment
One patient had oral anti-platelet therapy (500 mg acetylsalicylic acid/day) for 20 days to improve retinal perfusion secondary to retinal capillary occlusion [7]. The majority of patients with dengue ophthalmic complications were treated conservatively with only three patients needing platelet transfusion because of thrombocytopenia [8, 24]. The nadir platelet count in these patients ranged from 26 to 44 × 109/L [8, 24].
Prognosis
The mean time of follow-up for patients with dengue ophthalmic complications was 8.1 months, with a range of 0.3–26.0 months. Ophthalmic involvement secondary to dengue fever carries a good prognosis with good visual outcome. However, a significant number of patients have persistent scotoma despite clinical resolution of dengue ophthalmic complications. Patients with dengue-related maculopathy had persistent central or paracentral scotoma in as much as 59.5% of 74 affected eyes at 2-year follow-up from a study by Teoh et al. [33]. Despite this, only one patient had poor vision of worse than 6/24 after 2 years and another had persistent difficulty with near vision [33].
Overall, visual prognosis was good except in 13 patients, with residual visual acuity ranging from 6/30 to complete loss of vision. This was attributed to optic neuropathy in two patients [6, 29]; extensive panretinal and macular vasculitis in seven patients [20]; macular vaso-occlusive processes in one patient [7]; and acute angle closure glaucoma in one patient [26]. In the remaining two patients, the cause of residual visual deficit was not elaborated upon. Ten patients received intravenous methylprednisolone and the remaining two patients received surgical intervention, such as pars plana vitrectomy and laser iridotomies. Only 1 out of the 13 patients with poor visual outcome did not receive any form of treatment or intervention [5].
Conclusion
Dengue is endemic in tropical countries and the authors have seen a resurgence of dengue cases in the mid to late 2000s. This inflammatory process typically affects young immunocompetent adults, who often present at the nadir of thrombocytopenia with visual impairment. A myriad of ocular complications relate to dengue infection with most of them confined to the posterior pole of the fundus. The mechanism behind dengue infection and ocular involvement is unknown, but speculated to be related to an immune-mediated process and possibly associated with dengue serotyping. The prognosis for ophthalmic complications is good with improved visual acuity and resolution of ocular signs in most patients without any treatment. A proportion of patients with more severe ocular impairment require steroid treatment with most patients achieving reasonable improvement in vision and resolution of signs. Further studies are needed to elucidate the mechanism of ophthalmic complications of dengue. Randomized, controlled trials will aid to standardize investigations and determine the best form of treatment for these patients. This is important in the background of changing epidemiological patterns and co-circulation of various dengue serotypes. Ophthalmologists and physicians should be aware and vigilant towards patients with dengue-related ophthalmic complaints as a small minority of patients may have poor visual acuity refractory to treatment.
Acknowledgments
All authors have been involved in the drafting, writing, editing, and submission of this article in accordance to the International Committee of Medical Journal Editors’ guidelines. Dr. Sanjay is the guarantor for this article, and takes responsibility for the integrity of the work as a whole.
Conflict of interest
The authors declare no conflict of interest.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
References
- 1.World Health Organization. Dengue and dengue haemorrhagic fever—Fact sheet. 2009; Available at: http://www.who.int/csr/disease/dengue/en. Accessed 19 May 2011.
- 2.Barkham TM, Chung YK, Tang KF, Ooi EE. The performance of RT-PCR compared with a rapid serological assay for acute dengue fever in a diagnostic laboratory. Trans R Soc Trop Med Hyg. 2006;100:142–148. doi: 10.1016/j.trstmh.2005.05.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.De Oliveira Poersch C, Pavoni DP, Queiroz MH, et al. Dengue virus infections: comparison of methods for diagnosing the acute disease. J Clin Virol. 2005;32:272–277. doi: 10.1016/j.jcv.2004.08.008. [DOI] [PubMed] [Google Scholar]
- 4.Gubler DJ. Dengue and dengue hemorrhagic fever. Clin Microbiol Rev. 1998;11:480–496. doi: 10.1128/cmr.11.3.480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Haritoglou C, Dotse SD, Rudolph G, Stephan CM, Thurau SR, Klauss V. A tourist with dengue fever and visual loss. Lancet. 2002;360:1070. doi: 10.1016/S0140-6736(02)11145-7. [DOI] [PubMed] [Google Scholar]
- 6.Lim WK, Mathur R, Koh A, Yeoh R, Chee SP. Ocular manifestations of dengue fever. Ophthalmology. 2004;111:2057–2064. doi: 10.1016/j.ophtha.2004.03.038. [DOI] [PubMed] [Google Scholar]
- 7.Siqueira RC, Vitral NP, Campos WR, Orefice F, de Moraes Figueiredo LT. Ocular manifestations in dengue fever. Ocul Immunol Inflamm. 2004;12:323–327. doi: 10.1080/092739490500345. [DOI] [PubMed] [Google Scholar]
- 8.Chlebicki MP, Ang B, Barkham T, Laude A. Retinal hemorrhages in 4 patients with dengue fever. Emerg Infect Dis. 2005;11:770–772. doi: 10.3201/eid1105.040992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nainiwal S, Garg SP, Prakash G, Nainiwal N. Bilateral vitreous haemorrhage associated with dengue fever. Eye. 2005;19:1012–1013. doi: 10.1038/sj.eye.6701704. [DOI] [PubMed] [Google Scholar]
- 10.Chan DP, Teoh SC, Tan CS, et al. Eye institute dengue-related ophthalmic complications workgroup. Ophthalmic complications of dengue. Emerg Infect Dis. 2006;12:285–289. doi: 10.3201/eid1202.050274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bacsal KE, Chee SP, Cheng CL, Flores JV. Dengue-associated maculopathy. Arch Ophthalmol. 2007;125:501–510. doi: 10.1001/archopht.125.4.501. [DOI] [PubMed] [Google Scholar]
- 12.Su DH, Bacsal K, Chee SP, et al. Prevalence of dengue maculopathy in patients hospitalized for dengue fever. Ophthalmology. 2007;114:1743–1747. doi: 10.1016/j.ophtha.2007.03.054. [DOI] [PubMed] [Google Scholar]
- 13.Yamamoto Y, Takasaki T, Yamada K, et al. Acute disseminated encephalomyelitis following dengue fever. J Infect Chemother. 2002;8:175–177. doi: 10.1007/s101560200030. [DOI] [PubMed] [Google Scholar]
- 14.Cruz-Villegas V, Berrocal AM, Davis JL. Bilateral choroidal effusions associated with dengue fever. Retina. 2003;23:576–578. doi: 10.1097/00006982-200308000-00031. [DOI] [PubMed] [Google Scholar]
- 15.Mehta S. Ocular lesions in severe dengue hemorrhagic fever (DHF) J Assoc Physicians India. 2005;53:656–657. [PubMed] [Google Scholar]
- 16.Preechawat P, Poonyathalang A. Bilateral optic neuritis after dengue viral infection. J Neuroophthalmol. 2005;25:51–52. doi: 10.1097/00041327-200503000-00014. [DOI] [PubMed] [Google Scholar]
- 17.Habot-Wilner Z, Moisseiev J, Bin H, Rubinovitch B. A returned traveler with dengue fever and visual impairment. Isr Med Assoc J. 2005;7:200–201. [PubMed] [Google Scholar]
- 18.Kapoor HK, Bhai S, John M, Xavier J. Ocular manifestations of dengue fever in an East Indian epidemic. Can J Ophthalmol. 2006;41:741–746. doi: 10.3129/I06-069. [DOI] [PubMed] [Google Scholar]
- 19.de Amorim Garcia CA, Gomes AH, de Oliveira AG. Bilateral stellar neuroretinitis in a patient with dengue fever. Eye (Lond). 2006;20:1382–3. [DOI] [PubMed]
- 20.Teoh SC, Chan DP, Nah GK, et al. Eye institute dengue-related ophthalmic complications workgroup. A re-look at ocular complications in dengue fever and dengue haemorrhagic fever. Dengue Bull. 2006;30:184–193. [Google Scholar]
- 21.Seet RC, Quek AM, Lim EC. Symptoms and risk factors of ocular complications following dengue infection. J Clin Virol. 2007;38:101–105. doi: 10.1016/j.jcv.2006.11.002. [DOI] [PubMed] [Google Scholar]
- 22.Chang PE, Cheng CL, Asok K, Fong KY, Chee SP, Tan CK. Visual disturbances in dengue fever: an answer at last? Singapore Med J. 2007;48:71–73. [PubMed] [Google Scholar]
- 23.Tan SY, Kumar G, Surrun SK, Ong YY. Dengue maculopathy: a case report. Travel Med Infect Dis. 2007;5:62–63. doi: 10.1016/j.tmaid.2006.01.017. [DOI] [PubMed] [Google Scholar]
- 24.Tan CS, Teoh SC, Chan DP, Wong IB, Lim TH. Dengue retinopathy manifesting with bilateral vasculitis and macular oedema. Eye (Lond) 2007;21:875–877. doi: 10.1038/sj.eye.6702748. [DOI] [PubMed] [Google Scholar]
- 25.Beral L, Merle H, David T. Ocular complications of dengue fever. Ophthalmology. 2008;115:1100–1101. doi: 10.1016/j.ophtha.2008.02.017. [DOI] [PubMed] [Google Scholar]
- 26.Pierre Filho Pde T, Carvalho Filho JP, Pierre ET. Bilateral acute angle closure glaucoma in a patient with dengue fever: case report. Arq Bras Oftalmol. 2008;71:265–8. [DOI] [PubMed]
- 27.Kanungo S, Shukla D, Kim R. Branch retinal artery occlusion secondary to dengue fever. Indian J Ophthalmol. 2008;56:73–74. doi: 10.4103/0301-4738.37606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Loh BK, Bacsal K, Chee SP, Cheng BC, Wong D. Foveolitis associated with dengue fever: a case series. Ophthalmologica. 2008;222:317–320. doi: 10.1159/000144074. [DOI] [PubMed] [Google Scholar]
- 29.Sanjay S, Wagle AM, Au Eong KG. Optic neuropathy associated with dengue fever. Eye (Lond). 2008;22:722–4. [DOI] [PubMed]
- 30.Gupta A, Srinivasan R, Setia S, Soundravally R, Pandian DG. Uveitis following dengue fever. Eye (Lond) 2009;23:873–876. doi: 10.1038/eye.2008.124. [DOI] [PubMed] [Google Scholar]
- 31.Quek DT, Barkham T, Teoh SC. Recurrent bilateral dengue maculopathy following sequential infections with two serotypes of dengue virus. Eye (Lond) 2009;23:1471–1472. doi: 10.1038/eye.2008.149. [DOI] [PubMed] [Google Scholar]
- 32.Chee E, Sims JL, Jap A, Tan BH, Oh H, Chee SP. Comparison of prevalence of dengue maculopathy during two epidemics with differing predominant serotypes. Am J Ophthalmol. 2009;148:910–913. doi: 10.1016/j.ajo.2009.06.030. [DOI] [PubMed] [Google Scholar]
- 33.Teoh SC, Chee CK, Laude A, Goh KY, Barkham T, Ang BS. Optical coherence tomography patterns as predictors of visual outcome in dengue-related maculopathy. Retina. 2010;30:390–398. doi: 10.1097/IAE.0b013e3181bd2fc6. [DOI] [PubMed] [Google Scholar]
- 34.Ministry of Health, Singapore. Communicable disease surveillance in Singapore 2007, Singapore, 2008. Available at: http://www.moh.gov.sg/content/dam/moh_web/Publications/Reports/2008/2/Vector_Borne_Diseases.pdf. Accessed 13 Jun 2009.
- 35.Ministry of Health, Singapore. Communicable disease surveillance in Singapore 2005, Singapore, 2006. Available at: http://www.moh.gov.sg/content/dam/moh_web/Publications/Reports/2006/2/Vector_Borne_Diseases.pdf. Accessed 13 Jun 2009.