

Abstract
Background:
This case report represents one of the estimated 17,000 aneurysms clipped annually in the United States, often with nickel-containing clips. The authors highlight the development of life-threatening allergic vasculitis in a 33-year-old woman after aneurysm clipping.
Case Description:
After suffering subarachnoid hemorrhage, the patient had coil embolization at another facility for rupture of a right internal carotid artery (ICA) aneurysm. An incidental finding, an unruptured left posterior communicating artery aneurysm unamenable to coiling, was then successfully clipped via a left pterional craniotomy. Arriving in our emergency department 11 days later, she progressively declined during the next weeks, facing deteriorating clinical status (i.e. seizures) and additional infarctions in the left frontal lobe, midline shift, and new infarctions in the bilateral frontal lobe, right sylvian, right insular regions, and posterior cerebral artery distribution. During decompressive surgery, biopsy findings raised the possibility of lymphocytic vasculitis; consultations with rheumatology, allergy, and immunology specialists identified that our patient had a nickel allergy. After reoperation to replace the nickel-containing clip with one of a titanium alloy, the patient had an uncomplicated postoperative course and was discharged 6 days later to a rehabilitation facility.
Conclusions:
Nickel-related allergies are more common than appreciated, affecting up to 10% of patients. Fortunately, severe reactions are rare; nevertheless, vascular neurosurgeons should be aware of this potential complication when using cobalt alloy aneurysms clips. The use of titanium alloy clips eliminates this risk.
Keywords: Complication, nickel allergy, nickel sensitization
INTRODUCTION
Although rare, allergic reactions to nickel-containing aneurysm clips are also theoretically possible.[11] Given that nickel-related allergies affect about 10% of the United States population, this raises a concern for a comparable percentage of patients whose aneurysms are clipped using traditional metal clips. Specifically, allergies to common aneurysm clip components, such as nickel, affect an estimated 17% of women and 3% of men, whereas cobalt and chromium allergies affect 1-3% of the same population. This case report describes a young woman who developed a life-threatening allergic vasculitis after undergoing elective clipping of a posterior communicating artery aneurysm (PComA).
CASE REPORT
After suffering a subarachnoid hemorrhage (SAH), a 33-year-old woman underwent a coil embolization at an outside hospital for rupture of a right internal carotid artery (ICA) aneurysm [Figure 1]. At that time, cerebral angiography incidentally revealed an unruptured left PComA aneurysm that was deemed high risk for coiling. Following an excellent recovery from SAH, treatment of the unruptured aneurysm was recommended. Referred to our institution's cerebrovascular and stroke center for elective surgical repair, the patient underwent a left pterional craniotomy with anterior clinoidectomy and clipping of the unruptured aneurysm. With an uncomplicated initial postoperative course, she was discharged home the next day.
Figure 1.
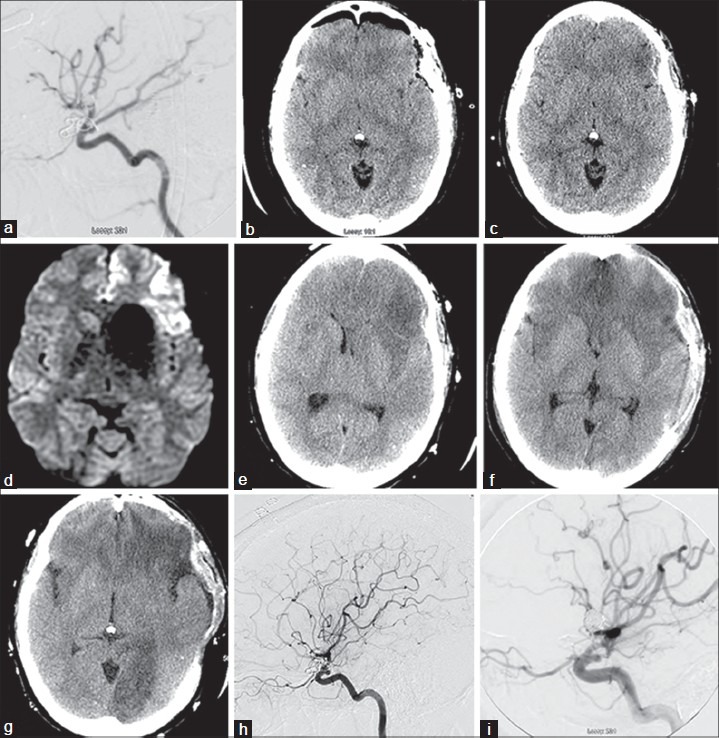
Tracing the month long course of life-threatening vasculitis after aneurysm clipping in a 33-year-old woman. Initial clipping. (a) After coil embolization for rupture of a right internal carotid artery (ICA) aneurysm, an unruptured left posterior communicating artery (PComA) aneurysm was incidentally detected and then treated by clipping; this intraoperative angiogram demonstrated flow in PComA and fetal posterior cerebral artery (PCA) after clipping and no residual aneurysm filling. (b) Postoperative CT confirms clipping was successful. Readmission and reclipping. Eleven days later (day 1), patient returns to the emergency department where head CT (c) and MRI (d) showed acute infarction in the orbitofrontal and left frontal opercular cortical regions. CTs during hospital days 11–22. Day 11 (e), progressive mass effect and infarction; day 12 (f), after surgical decompression, evolution of new bifrontal infarctions and day 16 (g) demonstrating new left PCA infarct with worsening of bilateral frontal infarctions. Day 17 (h), repeat angiogram shows high-grade stenosis and near-complete occlusion of the left PCA at the P1-2 junction; mild short segment stenosis involves several cortical branch vessels of left MCA. Day 22 (i), intraoperative angiogram after nickel-containing clip removal was replaced with titanium clip
However, 11 days later, the patient was readmitted in the emergency department with decreased oral intake, fever, altered mental status, and aphasic speech. On readmission (day 1), findings on head computed tomography (CT) and magnetic resonance imaging (MRI) studies demonstrated a small, acute left frontal lobe infarction. A CT angiography (CTA) performed the following day, though limited by significant streak artifact, revealed a moderate narrowing of the left paraclinoid ICA and non-visualization of P1. On day 2, the patient suffered a seizure, which was both witnessed and confirmed on emergent electroencephalography (EEG) findings. With clinical status precipitously declining and quickly progressing to status epilepticus, the patient was intubated and placed in a pharmacologically induced coma with pentobarbital.
During the following 3 days, she was slowly weaned from the pentobarbital coma; her neurological status remained poor. On day 6, the patient had a fixed and dilated right pupil; repeat CT scanning then demonstrated an enlarging infarction of the left frontal lobe with 7 mm of left-to-right midline shift, and new infarctions in the bilateral frontal lobe, right Sylvian, and right insular regions. During placement of a ventricular catheter, the opening pressure exceeded 20 mm Hg. The patient then underwent emergent decompressive fronto-temporo-parietal craniectomy; biopsies of the dura and frontal cortex were performed to evaluate for possible infectious or inflammatory process.
Although her neurological exam slightly improved postoperatively while in the neuroscience intensive care unit, intracranial pressures continued to spike after decompression. Biopsy findings, from the frontal dural and cortex, revealed nonspecific lymphocytic cuffing in small vessel walls with few neutrophils and rare eosinophils. With these findings, though nonspecific, raising the possibility of a so-called lymphocytic vasculitis, a trial of hydrocortisone began. Within 48 h of intravenous steroid therapy, intracranial pressures normalized. When the patient suffered repeated seizures on day 16, an emergent head CT demonstrated a new infarction now in the left posterior cerebral artery (PCA) territory. The following day, cerebral angiography to further evaluate the now suspected vasculitis demonstrated diminished flow in the left PComA, high grade stenosis of the left PCA near the P1–P2 junction, and mild short segment stenosis involving several cortical branch vessels of the left middle cerebral artery.
In consulting with rheumatology, allergy, and immunology specialists, we confirmed the likelihood of a nickel allergy. Given a standard nickel-containing Yasargil clip had been used for clipping the unruptured PComA aneurysm 32 days earlier, we reoperated and replaced it with a titanium alloy clip (Aesculap). With an uncomplicated postoperative course, the patient was discharged 6 days later to a long-term acute care facility for rehabilitation.
DISCUSSION
Our patient developed life-threatening encephalitis caused by an allergic reaction following clipping of an unruptured PComA aneurysm with a nickel-containing clip. During the 27-day period of this patient's continuing clinical and neurological decline, repeated imaging studies, surgeries, biopsies, and consults with other specialists confirmed the lymphocytic vascultis that led to reoperation and replacement with a pure titanium clip. Our case represents one of the estimated 17,000 aneurysms clipped each year with the routine use of nickel-containing clips.[1,5,6,7,8,12,13]
Metal allergies and surgical considerations
Metal allergies have been reported in a wide range of surgical cases from pediatric to orthopedic to neurosurgical. Rates have ranged as high as 28% in the orthopedic literature for early studies of metal-on-metal hip replacement[2] or as low as 2.2% for the Nuss procedure using a static implant for repair of pectus excavatum.[12] In the neurosurgical literature, metal allergies were reported in a case report by Ross et al. of intense pruritus after placement of a cobalt–nickel alloy clip.[11] In a study of deep brain stimulation in 79 patients with 124 electrodes, the authors reported allergic reactions in 2 (2.5%) of these patients.[10]
Nearly 10% of the general population experience nickel dermatitis,[3] with other studies delineating this further as affecting 5-20% of women and 2-4% of men[4] and posing questions about the complication risks associated with metal allergy for the 17,000 aneurysms clipped annually.[12] Women have a higher incidence of nickel allergy than men because of ear piercing – the most common cause of sensitization.[9]
Diagnosis of a nickel allergy includes examination of the skin for a rash, which is often edematous or erythematous; severe pruritus may cover the entire body. By screening who previously had such reaction (e.g. after wearing cheap nickel-containing jewelry), a diagnosis can be confirmed with a positive patch test. Medical management of the allergy includes both oral corticosteroids and antihistamines. If symptoms continue to progress after a trial of medical therapy, surgical removal of the nickel clip and replacement with a biologically inert, medical-grade titanium clip is recommended.
Since their inception in 1995, the use of Yasargil aneurysm clips composed of medical-grade titanium alloys has become increasingly widespread. Many of the major vascular centers in the United States have converted to titanium clips both to improve MRI compatibility and minimize metallic streak artifact on CT angiography (CTA) studies. Other manufacturers followed suit, offering titanium alloy clips as replacement for the older metal alloys. Titanium allergies have been reported in the medical literature, most commonly with dental implants.[14]
CONCLUSIONS
Amidst the 4-15% complication rates associated with clipping intracranial aneurysms, our case represents a life-threatening vasculitis caused by an allergic reaction to a nickel-containing aneurysm clip. Although such complications are rare in the literature, the 10% rate of nickel allergy in United States population hints that this type of complication should be considered in some of the 17,000 patients who undergo traditional aneurysm clipping. As we propose the routine use of medical-grade titanium clips for aneurysm clipping, cerebrovascular neurosurgeons should consider this potentially severe complication and screen appropriately whenever possible, especially in the setting of elective aneurysm repair.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2014/5/5/161/134813
Contributor Information
Andrew Grande, Email: grande@umn.edu.
Sanjeet Grewal, Email: grewalst@mail.uc.edu.
Ryan Tackla, Email: tacklard@email.uc.edu.
Andrew J. Ringer, Email: aringer@mayfieldclinic.com.
REFERENCES
- 1.Bederson JB, Awad IA, Wiebers DO, Piepgras D, Haley EC, Brott T, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke. 2000;31:2742–50. doi: 10.1161/01.str.31.11.2742. [DOI] [PubMed] [Google Scholar]
- 2.Benson MK, Goodwin PG, Brostoff J. Metal sensitivity in patients with joint replacement arthroplasties. Br Med J. 1975;4:374–5. doi: 10.1136/bmj.4.5993.374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Beth M. Nickel allergies. [Last accessed on 2006 Nov 03]. Available from: http://www.winter-branch.com/nickel-allergies.html .
- 4.Cerveny KA, Jr, Brodell RT. Blue jean button dermatitis. Nickel allergy presenting as a periumbilical rash. Postgrad Med. 2002;112:79–83. doi: 10.3810/pgm.2002.11.1354. [DOI] [PubMed] [Google Scholar]
- 5.Guglielmi G, Vinuela F, Dion J, Duckwiler G. Electrothrombosis of saccular an-eurysms via endovascular approach. Part 2: Preliminary clinical experience. J Neurosurg. 1991;75:8–14. doi: 10.3171/jns.1991.75.1.0008. [DOI] [PubMed] [Google Scholar]
- 6.International Study of Unruptured Intracranial Aneurysms (ISUIA) Investigators. Results of the International Study of Unruptured Intracranial Aneurysms. Lancet. 2003;362:103–10. [Google Scholar]
- 7.Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton JA, et al. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised trial. Lancet. 2002;360:1267–74. doi: 10.1016/s0140-6736(02)11314-6. [DOI] [PubMed] [Google Scholar]
- 8.Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, et al. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005;366:809–17. doi: 10.1016/S0140-6736(05)67214-5. [DOI] [PubMed] [Google Scholar]
- 9.Mortz CG, Lauritsen JM, Bindslev-Jensen C, Andersen KE. Nickel sensitization in adolescents and association with ear piercing, use of dental braces and hand eczema. The Odense Adolescence Cohort Study on Atopic Diseases and Dermatitis (TOACS) Acta Derm Venereol. 2002;82:359–64. doi: 10.1080/000155502320624096. [DOI] [PubMed] [Google Scholar]
- 10.Oh MY, Abosch A, Kim SH, Lang AE, Lozano AM. Long-term hardware-related complications of deep brain stimulation. Neurosurgery. 2002;50:1268–76. doi: 10.1097/00006123-200206000-00017. [DOI] [PubMed] [Google Scholar]
- 11.Ross IB, Warrington RJ, Halliday WC. Cell-mediated allergy to a cerebral aneurysm clip: Case report. Neurosurgery. 1998;43:1209–11. doi: 10.1097/00006123-199811000-00110. [DOI] [PubMed] [Google Scholar]
- 12.Rushing GD, Goretsky MJ, Gustin T, Morales M, Kelly RE, Jr, Nuss D. When it is not an infection: Metal allergy after the Nuss procedure for repair of pectus excavatum. J Pediatr Surg. 2007;42:93–7. doi: 10.1016/j.jpedsurg.2006.09.056. [DOI] [PubMed] [Google Scholar]
- 13.Simon SD, Koyama T, Cheng JS, Mericle RA. Medicare data reveal decline in number of craniotomies for aneurysm performed in the Medicare population. AANS Neurosurgeon. 2009;18:3. [Google Scholar]
- 14.Bilhan H, Bural C, Geckili O. Titanium hypersensitivity. A hidden threat for dental implant patients? N Y State Dent J. 2013;79:38–43. [PubMed] [Google Scholar]