

Abstract
Purpose
To assess and compare the value of FDG-PET to combined 111In-labeled leukocyte/99mTc-sulfur colloid bone marrow (WBC/BM) imaging for diagnosing infection in hip and knee prostheses.
Methods
In this prospective study, patients with painful hip or knee arthroplasty, who were scheduled to undergo clinical and diagnostic evaluation for prosthesis revision were included. They have been studied by using FDG-PET and 111In-labeled leukocyte/99mTc-sulfur colloid bone marrow scan. This study was IRB approved and HIPAA compliant. All patients provided written informed consent.
Results
A total of 134 hip and 87 knee prostheses, suspected of being either infected or non-infectious loosening were evaluated. All 221 prostheses underwent FDG-PET, whereas both WBC/BM imaging and FDG-PET was performed in 88 prostheses. The initial analysis of data from the WBC/BM images demonstrated somewhat results compared to those of FDG-PET scans on 88 patients. Also, some patients were not willing to undergo both procedures and therefore participate in this study. Therefore, a decision was made to eliminate WBC/BM imaging from the procedures for the remainder of this research study. This decision was reached partly due to the significant radiation dose delivered from labeled WBC as well as safety issues related to preparing these labeled cells. Final diagnosis was based on microbiological examinations of the surgical specimens in 125 prostheses and joint aspirations combined with the clinical follow-up of 6 months or more in 86 prostheses. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of FDG-PET in hip prostheses were 81.8%, 93.1%, 79.4%, and 94.0%, respectively and in knee prostheses were 94.7%, 88.2%, 69.2%, and 98.4% respectively. The sensitivity, specificity, PPV, and NPV of WBC/BM imaging in hip prostheses were 38.5%, 95.7%, 71.4%, and 84.6%, respectively and in knee prostheses were 33.3%, 88.5%, 25.0%, and 92.0%, respectively. In those cases that underwent both FDG-PET and WBC/BM imaging, there was a trend (P=0.0625) towards a higher sensitivity for FDG-PET in hip prostheses, whereas other comparisons did not show any significant differences between the two imaging modalities.
Conclusion
Based on this study, the diagnostic performance of FDG-PET scan in detecting infection in painful hip and knee prostheses is optimal for routine clinical application. Considering the complexity and costs of WBC/BM imaging and related safety issues associated with this preparation, FDG-PET appears to be an appropriate alternative for assessing these patients.
Keywords: Arthroplasty, FDG-PET, Infection, Prosthesis, WBC/BM imaging
Introduction
The accurate differentiation between prosthetic joint infection and aseptic loosening in the painful lower extremity prosthesis is a major clinical challenge. The clinical and economical implications are substantial taking into account that a large number of hip and knee arthroplasties are performed in the United States annually [1]. Combined 111In-labeled leukocyte (WBC)/99mTc-sulfur colloid marrow (BM) (WBC/BM) imaging is currently regarded as the method of choice for detecting infection in this setting, but suffers from several limitations [2-4]. The in vitro labeling process is labor intensive and involves direct handling of blood products, which carries the risks of contaminating the final product with lethal pathogens and potential for interpatient misadministration. A complete examination requires a BM scan to localize the sites of red marrow that can be a source of false positive results on labeled white blood cell scans. In addition, the results of this procedure are available only after 24-48 hours. Moreover, this procedure involves higher levels of radiation exposure on comparative dosimetry when using FDG-PET and FDG-PET/CT [2-4].
In recent years, 18F-fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) has shown great promise in the evaluation of infection and inflammation [5, 6]. FDG-PET has many practical advantages over WBC/BM imaging, including its routine availability in advanced societies, the requirement for only a single radiotracer injection, completion of the test within a brief period of time (in less than 2 hours), outstanding safety record (lack of pathogens in the final product based on existing FDA records), and substantially lower radiation exposure and costs. Moreover, PET provides superior spatial resolution compared to WBC/BM imaging, which may provide an advantage in managing these patients [4-6].
In recent literature, FDG-PET imaging has been proposed for detecting infections in orthopedic patients [5, 7-13]. The reported studies have shown promising but somewhat variable results [14]. These conflicting data are partly due to the small number of patients enrolled in such studies and variable diagnostic techniques and interpretation criteria employed in these studies [14]. Therefore, a prospective study with a large sample size and strict diagnostic criteria was required to determine its role in the setting of painful lower limb prosthesis.
The purpose of this prospective study was to assess and compare the value of FDG-PET to WBC/BM imaging for diagnosing infection in hip and knee prostheses.
Materials and Methods
Patient population
This Health Insurance Portability and Accountability Act-compliant prospective study was performed with institutional review board approval, and informed written consent was obtained from each patient prior to enrollment. Patients with painful hip or knee arthroplasty, who were scheduled to undergo clinical and diagnostic evaluation for prosthesis revision between 2/24/03-11/6/2008, were included. The following exclusion criteria were applied:
Patients who have another known etiology for pain in the prosthetic area (besides aseptic loosening or infection) such as dislocation or fracture of the prosthesis or bone, as determined by clinical examination and/or other investigations including conventional radiography.
Patients who have another significant medical, surgical, or psychiatric condition, currently uncontrolled by treatment.
Women who are lactating or pregnant as defined by a urine or serum β-HCG test obtained at screening and baseline.
Patients unable to attain a blood sugar level of or below 200 mg/dL.
Patients unable to give informed consent.
Imaging techniques
All patients enrolled in this study were required to undergo FDG-PET, while a subset of consecutive patients also underwent WBC/BM imaging in the beginning of this trial. The WBC/BM imaging procedure was initiated by drawing 50 ml of blood for labeling with 111Indium-oxine soon after the patient arrived in the facility. While the labeling process was ongoing, a BM scan of the joint prosthesis region was obtained. Immediately thereafter, an FDG-PET study was initiated and completed during this first visit. At the completion of the FDG-PET examination, labeled white blood cells were infused and the patient returned the next day for WBC imaging. This plan allowed a relatively time-effective schedule for the patients and also permitted acquiring optimal high quality imaging of the radiotracers administered to the patient.
FDG-PET imaging
The FDG-PET examination was performed on an Allegro PET scanner (ADAC Laboratories) approximately sixty minutes after the intravenous administration of 0.14mCi/kg of FDG with emission data acquired over the pelvis and the entire femur with successive overlapping axial frames. The transmission scan was performed in single acquisition mode using a 137Cs point source. Image segmentation was applied to the transmission image, which was then incorporated into a system-modeled attenuation correction during image reconstruction.
BM imaging
The bone marrow examination was performed on day 1, prior to FDG-PET, after intravenous administration of 15mCi (555 MBq) of 99mTc-labeled sulfur colloid. Fifteen minutes following injection, the patient was positioned in a dual-head scanner (Prism 2000, Picker) fitted with low energy all purpose collimators. Images of the joint prosthesis region were acquired over 20 minutes.
WBC imaging
White blood cells were labeled by following the standard procedures described in the literature [15]. After the completion of the BM and FDG-PET imaging studies, approximately 500 μCi of 111In-WBCs were administrated intravenously. The patients then returned 18-24 hours later for imaging purposes. A medium energy collimator was used for all 111Indium studies. Images of joint prosthesis areas were acquired by utilizing the photopeaks of 111Indium (174 keV and 247 keV with 15% energy window for each) over 30 minutes.
Image interpretation
Images from the two types of studies (FDG-PET and WBC/BM imaging) were interpreted separately and the readers (A.A. and H.Z., both experienced nuclear medicine physicians with more than three decades and one decade of experience in the specialty, respectively) were blinded with regard to the clinical information and the results from the different imaging modalities as well as from the results from the microbiological examination. After the final diagnostic criteria had been defined, the scans of at least 25 patients were read independently by the each of the two readers, and excellent agreement (i.e. not a single disagreement) was noted between the two readers. From then on, each FDG-PET scan and each WBC/BM scan was interpreted by either one of two readers, in a random order. Also, PET scans with discrepant results with the final diagnosis were re-reviewed which also revealed very high correlation with the original interpretation. This further demonstrated the reproducibility of the criteria employed for assessing PET scan findings.
FDG-PET criteria
The interpretation of the FDG-PET data generated from this study was based upon the predefined criteria that our group and other investigators have published in the literature [11, 12]. Special attention was paid to the uptake of FDG in the prosthesis-bone or the prosthesis-soft tissue interfaces. A study was called positive for infection prosthesis if increased FDG uptake was noted at the prosthesis-bone interface in the middle portion of the shaft of the hip prosthesis (Figures 1, 2, 3). A study was considered negative if FDG uptake was limited to the soft tissues, synovium, or adjacent only to the neck of the prosthesis (Figure 1).
Figure 1.

In this patient with bilateral hip prostheses, the maximum intensity projection image shows FDG uptake patterns in non-infected hip prosthesis and infected hip prosthesis. In the right non-infected hip prosthesis, some uptake of FDG is noted around the neck (arrow heads), while the bone-prosthesis interface appears without significant FDG uptake. In contrast, the left infected hip prosthesis reveals significant tracer concentration at the bone-prosthesis interface (arrows). In this particular patient, there is also significant activity in the tip of the prosthesis (dashed arrow).
Figure 2.

This maximum intensity projection image shows significant uptake of FDG in an irregular pattern in the upper half of the right femur, which were demonstrated to be located at the bone-prosthesis interface on the tomographic images. Again, this is a typical pattern for infected hip prosthesis.
Figure 3.
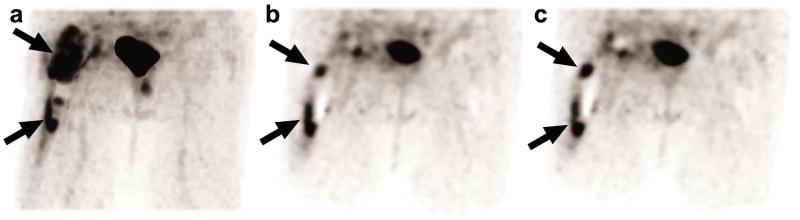
In this patient with proven infected right hip prosthesis, the maximum intensity projection image (a) shows intense uptake of FDG proximally with some extension to the lower segment of the insertion (arrows). Tomographic images (b, c) demonstrate clear bone-prosthesis interface uptake of FDG (arrows) which is typical of prosthetic joint infection.
For the patients with knee arthroplasty, only uptake at the bone/prosthesis interface was considered as being consistent with infection (Figure 4). Patients with no or minimal uptake in these locations were interpreted to have non-infected joints (Figure 5). Soft tissue/synovial uptake around the joint was not used as evidence for infection.
Figure 4.
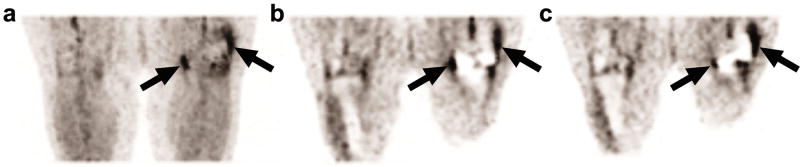
In this patient with proven infected left knee prosthesis, the maximum intensity projection image (a) reveals intense uptake of FDG in the medial and upper lateral aspect (arrows) of the prosthesis, which is typical of prosthetic joint infection. Tomographic images (b, c) show the exact locations of these sites at the bone-prosthesis interface (arrows).
Figure 5.

This tomographic image of uncomplicated and non-infected knee prostheses shows minimal uptake of FDG at the bone-prosthesis interfaces. This is the typical pattern noted in the non-infected knee prosthesis.
WBC/BM imaging criteria
Combined WBC and BM images were read as positive for infection if radiotracer activity was noted in peri-prosthetic region on the WBC images and no corresponding radiotracer activity was observed on the BM images. The combined scans were read as negative for infection if the radiotracer uptake distribution from the two techniques were similar and spatially congruent.
In the initial phase of the study we performed both FDG-PET and WBC/BM imaging in every patient enrolled; however, after the initial analyses from the data generated we realized the results from WBC-BM scans (in hip prostheses) were somewhat suboptimal compared to FDG-PET imaging findings. Also, some patients were not willing to undergo both procedures and therefore participate in this study. We should point out that many of these patients were referred to us from long distances. Therefore, performing both FDG-PET and conventional imaging techniques required either long traveling time or an overnight stay. Thus, we decided to pursue FDG-PET only for the remainder of the trial and base the merit of this technique on the final diagnosis reached by the attending physicians after surgical intervention and other test results.
Pathological/microbiological evaluation
In those patients who underwent surgical exploration, the final diagnosis was based upon microbiological results of the surgical specimens. Pathology reports (all sections were studied using standard staining techniques with hematoxylin and eosin) and the culture reports were generated by experienced pathologists and the microbiologists at the Institution. The diagnosis of infection was based upon either the detection of microorganisms in cultures or the findings of purulent fluid within the area of interest and the presence of neutrophilic infiltrates at the sites [16]. The type of microorganisms cultured were similar to that reported in the literature, namely staphylococcus and other gram positive cocci were the main causes of infection. The diagnostic criteria for infection in different imaging studies and pathological/microbiological evaluation have been tabulated in Table 1.
Table 1. Diagnostic criteria for prosthetic joint infection in different imaging studies and pathological/microbiological evaluation.
| Name of the test | Diagnostic criteria for prosthetic joint infection |
|---|---|
| FDG-PET | Study was called positive for infection if increased FDG uptake was noted at the prosthesis-bone interface in the middle portion of the shaft of the hip prosthesis. Study was considered negative if FDG uptake was limited to the soft tissues, or adjacent only to the neck of the prosthesis. For the patients with knee arthroplasty, only uptake at the bone/prosthesis interface was considered as being consistent with infection. Patients with no or minimal uptake in these locations were interpreted to have non-infected joints |
| WBC/BM imaging | WBC/BM scans were read as positive for infection if radiotracer activity was noted in peri-prosthetic region on the WBC images and no corresponding radiotracer activity was observed on the BM images. The combined scans were read as negative for infection if the radiotracer uptake distribution from the two techniques were similar and spatially congruent. |
| Pathological/microbiological evaluation | All pathologic sections were investigated using standard hematoxylin and eosin staining techniques. Sections were analyzed according to the criteria as described by Feldman et al. [16]: (1) presence of granulation tissue; (2) utilization of the five most cellular fields for final diagnosis, as determined on the basis of the number of polymorphonuclear (PMN) leukocytes; (3) cell count determination under 40-times magnification; (4) utilization of at least two samples of tissue; and (5) inclusion of only PMN leukocytes, identified within tissue rather than fibrin, with well-defined cytoplasmic borders. Frozen specimens with fewer than five PMN leukocytes per high-power field were considered aseptic, while specimens with at least ten PMN cells indicated infection. Specimens with five to nine PMN leukocytes raised suspicion for infection, leaving culture reports in this equivocal group to determine the final diagnosis. A permanent specimen was considered positive if five or more PMN leukocytes per high power field were noted. |
Statistical analysis
To compare FDG-PET and WBC/BM imaging, we constructed 2×2 tables comparing correct versus incorrect readings for both FDG-PET and WBC/BM imaging. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy, positive likelihood ratio (+LR) and negative likelihood ratio (-LR) of FDG-PET and WBC/BM imaging were calculated, along with 95% confidence intervals. In those cases that underwent both FDG-PET and WBC/BM imaging, sensitivity and specificity of the two imaging modalities were compared using McNemar's test [17]. Areas under the receiver operating characteristic (ROC) curves (AUCs) wre calculated, along with 95% confidence intervals. All analyses were done for hip and knee prostheses separately. Statistical analyses were executed using MedCalc Software (MedCalc, Mariakerke, Belgium).
Results
Number of cases, FDG-PET and WBC/BM scans, and reference standard
A total of 134 painful hip prostheses (77 in men, 57 in women; mean patient age: 57 years, age range: 18-84 years; bilateral prostheses in 5 cases) and 87 painful knee prostheses (35 in men, 52 in women; mean patient age: 57 years, age range: 32-83 years; bilateral prostheses in 6 cases) were enrolled in this prospective investigation. All 221 prostheses underwent FDG-PET, whereas WBC/BM imaging was performed only in 88 prostheses (59 hip prostheses and 29 knee prostheses). The analysis of the data from the first 88 patients revealed relatively high performance of FDG-PET over WBC/BM imaging for detection of infection. By considering the complexity of preparing radiolabeled WBC and substantial radiation exposure of sensitive organs such as the spleen, a decision was made to limit this research only to FDG-PET imaging for examining future patients enrolled. The mean numbers of years between hip arthroplasty and FDG-PET, knee arthroplasty and FDG-PET, hip arthroplasty and WBC/BM imaging, and knee arthroplasty and WBC/BM imaging were 5.8 years, 3.7 years, 3.7 years, and 6.4 years, respectively. Final diagnosis was based on microbiological examinations of the surgical specimens in 125 prostheses (87 hip prostheses and 38 knee prostheses) and joint aspirations combined with the clinical follow-up of 6 months or more in 96 prostheses (47 hip prostheses and 49 knee prostheses). The standard criteria were close observation for presence of infection and eventual failure of the inserted prosthesis. The lack of such outcomes was considered as evidence for other causes than infection as the underlying etiology of pain in this population. Based on the standard of reference, 52 of 221 cases (33 hip prostheses and 19 knee prostheses) proved to have periprosthetic infection.
Evaluation of hip arthroplasty
The sensitivity, specificity, PPV, NPV, and AUC of FDG-PET in hip prostheses were 81.8%, 93.1%, 79.4%, 94.0%, and 0.874, respectively (Table 2). The sensitivity, specificity, PPV, NPV, and AUC of WBC/BM imaging in hip prostheses were 38.5%, 95.7%, 71.4%, 84.6%, and 0.671, respectively (Table 2). In those cases that underwent both FDG-PET and WBC/BM imaging (Table 3), there was a trend (P=0.0625) towards a higher sensitivity for FDG-PET, whereas there was no significant difference (P=1.000) in specificity between the two imaging modalities.
Table 2. Overall diagnostic values of FDG-PET and WBC/BM imaging in hip prostheses.
| FDG-PET imaging | WBC/BM imaging | |
|---|---|---|
| Sensitivity | 81.8 (27/33) | 38.5 (5/13) |
| 95% Confidence Interval | 65.6-91.4 | (17.7-64.5) |
| Specificity | 93.1 (94/101) | 95.7 (44/46) |
| 95% Confidence Interval | 86.4-96.6 | (85.5-98.8) |
| Positive Predictive Value (PPV) | 79.4 (27/34) | 71.4 (5/7) |
| 95% Confidence Interval | 63.2-89.7 | (35.9-91.8) |
| Negative Predictive Value (NPV) | 94.0 (94/100) | 84.6 (44/52) |
| 95% Confidence Interval | 87.5-97.2 | (72.5-92.0) |
| Accuracy | 90.3 | 83.1 |
| 95% Confidence Interval | 83.5-94.7 | 73.8-88.6 |
| Positive Likelihood Ratio (+LR) | 11.8 | 8.84 |
| 95% Confidence Interval | 6.0-22.8 | 1.69-63.06 |
| Negative Likelihood Ratio (-LR) | 0.195 | 0.64 |
| 95% Confidence Interval | 0.09-0.36 | 0.49-0.92 |
| Area under the ROC curve | 0.874 | 0.671 |
| 95% Confidence Interval | 0.806-0.925 | 0.536-0.787 |
Table 3. Diagnostic values of FDG-PET and WBC/BM imaging in patients with hip prostheses who had undergone both studies.
| FDG-PET imaging |
WBC/BM imaging |
P-value | |
|---|---|---|---|
| Sensitivity | 76.9 (10/13) | 38.5 (5/13) | P=0.0625 |
| 95% Confidence Interval | (49.7-91.8) | (17.7-64.5) | |
| Specificity | 93.5 (43/46) | 95.7 (44/46) | P=1.0000 |
| 95% Confidence Interval | (82.5-97.8) | (85.5-98.8) | |
| Negative Predictive Value (NPV) | 76.9 (10/13) | 71.4 (5/7) | |
| 95% Confidence Interval | (49.7-91.8) | (35.9-91.8) | |
| Positive Predictive Value (PPV) | 93.5 (43/46) | 84.6 (44/52) | |
| 95% Confidence Interval | (82.5-97.8) | (72.5-92.0) |
Evaluation of knee arthroplasty
The sensitivity, specificity, PPV, NPV, and AUC of FDG-PET in knee prostheses were 94.7%, 88.2%, 69.2%, 98.4%, and 0.915, respectively (Table 4). The sensitivity, specificity, PPV, NPV, and AUC of WBC/BM imaging in knee prostheses were 33.3%, 88.5%, 25.0%, 92.0%, and 0.609, respectively (Table 4). In those cases that underwent both FDG-PET and WBC/BM imaging (Table 5), there were no significant differences in sensitivity and specificity between the two imaging modalities (P=0.500 and P=1.000, respectively), although it should be mentioned that the number cases available for statistical comparison of sensitivities was low.
Table 4. Overall diagnostic values of FDG-PET and WBC/BM imaging in knee prostheses.
| FDG-PET imaging | WBC/BM imaging | |
|---|---|---|
| Sensitivity | 94.7 (18/19) | 33.3 (1/3) |
| 95% Confidence Interval | 75.4-99.1 | (6.2-79.2) |
| Specificity | 88.2 (60/68) | 88.5 (23/26) |
| 95% Confidence Interval | 78.5-93.9 | (71.0-96.0) |
| Positive Predictive Value (PPV) | 69.2 (18/26) | 25.0 (1/4) |
| 95% Confidence Interval | 50.0-83.5 | (4.6-69.9) |
| Negative Predictive Value (NPV) | 98.4 (60/61) | 92.0 (23/25) |
| 95% Confidence Interval | 91.3-99.7 | (75.0-97.8) |
| Accuracy | 89.7 | 82.8 |
| 95% Confidence Interval | 81.3-91.8 | 76.2-93.5 |
| Positive Likelihood Ratio (+LR) | 8.1 | 2.8 |
| 95% Confidence Interval | 4.4-9.7 | 0.11-15.4 |
| Negative Likelihood Ratio (-LR) | 0.06 | 0.7 |
| 95% Confidence Interval | 0.003-0.29 | 0.15-1.16 |
| Area under the ROC curve | 0.915 | 0.609 |
| 95% Confidence Interval | 0.835-0.964 | 0.411-0.783 |
Table 5. Diagnostic values of FDG-PET and WBC/BM imaging in patients with knee prostheses who had undergone both studies.
| FDG-PET imaging |
WBC/BM imaging |
P -value | |
|---|---|---|---|
| Sensitivity | 100 (3/3) | 33.3 (1/3) | P=0.5000 |
| 95% Confidence Interval | (43.9-100) | (6.2-79.2) | |
| Specificity | 88.5 (23/26) | 88.5 (23/26) | P=1.0000 |
| 95% Confidence Interval | (71.0-96.0) | (71.0-96.0) | |
| Positive Predictive Value (PPV) | 50.0 (3/6) | 25.0 (1/4) | |
| 95% Confidence Interval | (18.8-81.2) | (4.6-69.9) | |
| Negative Predictive Value (NPV) | 100 (23/23) | 92.0 (23/25) | |
| 95% Confidence Interval | (85.7-100) | (75.0-97.8) |
Discussion
Over the past three decades, imaging with radiolabeled preparations has increasingly aided in the diagnosis of septic joint arthroplasty. Bone scanning combined with 67Gallium imaging was the first generation of such techniques introduced for this purpose. However, this combination was noted to have less then ideal accuracy in most clinical settings [18-22]. With the evolution of radiolabeled white cell methodologies, combined WBC/BM scintigraphy has become the imaging modality of choice for assessing patients with suspected infection in the transplanted prostheses [5,18,22]. However, this is a time consuming, technically demanding, and relatively expensive procedure (the entire process requires at least two days to be completed) with potentially harmful side-effects (related to the direct handling of blood products and the substantial radiation exposure). Therefore, in recent years efforts have been made to determine and validate the role of FDG-PET in this common and clinically challenging setting [5, 6]. Detection of infection by labeled WBC imaging is based upon the assumption that the administered cells will migrate to the sites of infection. Since most of the labeled leukocyte preparation consists of neutrophils, inflammatory/infectious processes with a predominantly neutrophilic infiltrate (acute infections) are likely to yield positive results [5, 6]. However, most infections associated with arthroplasties are sub-acute or chronic in nature [5, 6]. Consequently, the dominant inflammatory cells involved are monocytes and lymphocytes [5, 6]. In contrast, the uptake of FDG in the inflammatory cells reflects “in vivo labeling” of the existing and activated cells at the site of infection soon after the administration of the compound. This would indicate that FDG-PET might allow imaging a substantially larger population of cells, which are residing in the area of infection and inflammation. Therefore, in addition to considerable simplification of procedures associated with the WBC/BM imaging method, including the time required to complete the study, this approach may provide higher sensitivity for diagnosing infection in such settings. Furthermore, since FDG uptake does not rely upon leukocyte migration, treatment with antibiotics is less likely to affect its sensitivity in delineating the sites of infection [5]. Of interest, at the recent International Consensus Meeting on Periprosthetic Joint Infection, the above-mentioned disadvantages and limitations of labeled WBC imaging were acknowledged by world authorities in this field, and it was stated that alternative approaches should be explored in the near future.
Prior to undertaking this investigation, several reports on the utility of FDG-PET in the evaluation of painful lower extremity joint prostheses have appeared in the literature; these reports from various groups provided mixed results [14]. For example, Zhuang et al. [11] reported a sensitivity of 90% and a specificity of 89% for FDG PET in diagnosing infected lower limb prostheses. Vanquickenborne et al. [13] reported that analysis of PET images alone resulted in 88% sensitivity and 78% specificity. The authors concluded FDG-PET scans alone showed the same sensitivity as that of WBC/BM imaging, while the specificity was slightly higher for the latter method. In contrast, Love et al. [9] and Stumpe et al. [10] reported an overall low accuracy for this technique and concluded that FDG-PET cannot replace WBC/BM imaging for diagnosing infection of the failed prosthetic joint. Several factors can explain these discrepant results [7-13] in the reported efficacy of FDG-PET in evaluating hip arthroplasties.
One major contributing issue to these prior variable results is the lack of uniform criteria for interpreting the results generated by this technique by different investigators [14]. It is well known that non-specific FDG accumulation may be present around the head and neck portion of the prosthesis for several months (and possibly years) after surgery [12]. At present, the site and pattern of FDG accumulation appear to be more important than the intensity of uptake at these locations [5, 12]. While some investigators have relied upon FDG uptake estimated by calculation of standardized uptake value (SUV) score around the prosthesis to interpret the FDG-PET scans, others have considered the site and pattern as the primary base for this purpose [5, 12]. We believe that abnormal FDG uptake along the bone prosthesis interface in the middle portion of the shaft of the prosthesis is the most reliable indicator of periprosthetic infection [12]. The scans of the patients with discrepant results between FDG-PET and final diagnosis, were reanalyzed which revealed reproducible results and did not substantially change the original statistics from the initial readings. In addition, technical factors may contribute to the two discrepant reports in the literature [5, 7-13]. For example, Love et al. [9] used a very low quality system called coincidence PET (outdated by any standards even at the time when the study was carried out), as a result of which the diagnostic performance of FDG imaging was erroneously interpreted as being inferior to WBC/BM imaging by these investigators. To overcome these technical issues, we employed a standard PET instrument which utilized an external radionuclide source for attenuation correction. Our results clearly demonstrate that optimal methodologies with regard to the instrumentation employed and the interpretation criteria are essential for generating the desired results.
The limitations of this study include the following: only limited patients had both studies, the reason for which has been already explained. We believe the implication of small size of patients in patients with knee arthroplasty, who had both FDG-PET and WBC/BM imaging, will require this to be examined more critically to comment that FDG-PET can replace WBC/BM in patients with knee arthroplasty. However, we have to emphasize that relatively high performance of FDG-PET imaging in either hip or knee prosthesis infection in the first 88 patients resulted in deleting WBC/BM imaging from the protocol for the remainder of subjects enrolled in this study. Also, safety issues associated with radiolabeled white blood cells contributed to this decision. The present study data can also be used for a future meta-analysis. Finally, all FDG-PET examinations in this study were performed using a stand-alone PET system (using a 137Cs point source for transmission scanning and attenuation correction), whereas integrated PET/CT has become the standard method for PET scanning in most institutions. Metallic prosthetic replacements, such as hip or knee implants, are known to cause strong streaking artefacts in CT images, which may induce over- or underestimation of the activity concentration near the metallic implants when applying CT-based attenuation correction of PET images. However, with new metal artifact reduction methods, more accurate CT-based attenuation correction of PET images can be achieved and misinterpretation of tracer uptake can be prevented [23]. Moreover, our own experience has shown that integrated PET/CT performs as well as stand-alone PET in this setting (unpublished results). Therefore, state-of-the-art PET/CT equipment is expected to yield results that are at least equal to those presented in the present study.
In conclusion, in this study equivalent sensitivity and specificity (i.e. non-inferiority) was observed for FDG-PET compared to WBC/BM imaging for detecting prosthetic hip or knee joint infection. For this investigation, we used the criteria described by Zhuang et al. [11, 12] where increased uptake around the head or neck of the prosthesis is considered an expected finding on the FDG-PET scans who have hip prosthesis implants. Hence we believe knowledge of the typical patterns that are commonly observed following hip arthroplasty is required in interpreting the FDG-PET scans. We did not perform SUV based analysis and diagnosis, since other investigators have shown that SUV measurements cannot differentiate between infection and aseptic loosening reliably [24, 25]. With the introduction of additional data into the literature and the optimal experience gained by the readers of the FDG-PET images in the setting of complicated arthroplasties the role of this modality will be firmly established in the literature. These data demonstrate that FDG-PET can play an effective role in assessing patients with prosthesis implant where superimposed infection is suspected and also has value in excluding infection. We should emphasize that recent consensus guideline for assessing prosthetic joint infection does not include WBC-BM imaging for detecting infection in painful joints [26]. The conclusions drawn were partly reached based on the deficiencies that the orthopedics community worldwide has noted in this setting using this diagnostic test. In this scientific communication we have also described in great detail shortcoming of WBC-BM imaging in this complicated and difficult domain.
Acknowledgments
Funding Information: This research was supported by NIH grant R01-AR048241-04 (PI: Alavi, Abass). Therefore, this paper should be accessible by public at large.
Footnotes
Main Institution: Hospital of the University of Pennsylvania, Department of Radiology, Division of Nuclear Medicine, Philadelphia, Pennsylvania, 19104, United States
References
- 1.Del Pozo JL, Patel R. Clinical practice. Infection associated with prosthetic joints. N Engl J Med. 2009;361:787–794. doi: 10.1056/NEJMcp0905029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mulamba L, Ferrant A, Leners N, de Nayer P, Rombouts JJ, Vincent A. Indium-111 leucocyte scanning in the evaluation of painful hip arthroplasty. Acta Orthop Scand. 1983;54:695–697. doi: 10.3109/17453678308996613. [DOI] [PubMed] [Google Scholar]
- 3.Palestro CJ, Kim CK, Swyer AJ, et al. Total-hip arthroplasty: periprosthetic indium-111-labeled leukocyte activity and complementary technetium-99m-sulfur colloid imaging in suspected infection. J Nucl Med. 1990;31:1950–1955. [PubMed] [Google Scholar]
- 4.Kwee TC, Basu S, Torigian DA, et al. FDG-PET Imaging for diagnosing prosthetic joint infection: discussing the facts, rectifying the unsupported claims and call for evidence-based and scientific approach. Eur J Nucl Med Mol Imaging. 2013;40:464–466. doi: 10.1007/s00259-012-2319-1. [DOI] [PubMed] [Google Scholar]
- 5.Basu S, Chryssikos T, Moghadam-Kia S, et al. Positron emission tomography as a diagnostic tool in infection: present role and future possibilities. Semin Nucl Med. 2009;39:36–51. doi: 10.1053/j.semnuclmed.2008.08.004. [DOI] [PubMed] [Google Scholar]
- 6.Basu S, Zhuang H, Torigian DA, et al. Functional imaging of inflammatory diseases using nuclear medicine techniques. Semin Nucl Med. 2009;39:124–145. doi: 10.1053/j.semnuclmed.2008.10.006. [DOI] [PubMed] [Google Scholar]
- 7.Guhlmann A, Brecht-Krauss D, Suger G, et al. Chronic osteomyelitis: detection with FDG PET and correlation with histopathologic findings. Radiology. 1998;206:749–754. doi: 10.1148/radiology.206.3.9494496. [DOI] [PubMed] [Google Scholar]
- 8.De Winter F, van de Wiele C, Vogelaers D, et al. Fluorine-18 fluorodeoxyglucose-position emission tomography: a highly accurate imaging modality for the diagnosis of chronic musculoskeletal infections. J Bone Joint Surg Am. 2001;83-A(5):651–660. doi: 10.2106/00004623-200105000-00002. [DOI] [PubMed] [Google Scholar]
- 9.Love C, Marwin SE, Tomas MB, et al. Diagnosing infection in the failed joint replacement: a comparison of coincidence detection 18F-FDG and 111In-labeled leukocyte/99mTc-sulfur colloid marrow imaging. J Nucl Med. 2004;45:1864–1871. [PubMed] [Google Scholar]
- 10.Stumpe KD, Nötzli HP, Zanetti M, et al. FDG PET for differentiation of infection and aseptic loosening in total hip replacements: comparison with conventional radiography and three-phase bone scintigraphy. Radiology. 2004;231:333–341. doi: 10.1148/radiol.2312021596. [DOI] [PubMed] [Google Scholar]
- 11.Zhuang H, Duarte PS, Pourdehnad M, et al. The promising role of 18F-FDG PET in detecting infected lower limb prosthesis implants. J Nucl Med. 2001;42:44–48. [PubMed] [Google Scholar]
- 12.Zhuang H, Chacko TK, Hickeson M, et al. Persistent non-specific FDG uptake on PET imaging following hip arthroplasty. Eur J Nucl Med Mol Imaging. 2002;29:1328–1333. doi: 10.1007/s00259-002-0886-2. [DOI] [PubMed] [Google Scholar]
- 13.Vanquickenborne B, Maes A, Nuyts J, et al. The value of (18)FDG-PET for the detection of infected hip prosthesis. Eur J Nucl Med Mol Imaging. 2003;30:705–715. doi: 10.1007/s00259-002-1109-6. [DOI] [PubMed] [Google Scholar]
- 14.Kwee TC, Kwee RM, Alavi A. FDG-PET for diagnosing prosthetic joint infection: systematic review and metaanalysis. Eur J Nucl Med Mol Imaging. 2008;35:2122–32. doi: 10.1007/s00259-008-0887-x. [DOI] [PubMed] [Google Scholar]
- 15.McAfee JG, Thakur ML. Survey of radioactive agents for in vitro labelling of phagocytic leukocytes. I. Soluble agents. J Nucl Med. 1976;17:480–487. [PubMed] [Google Scholar]
- 16.Feldman DS, Lonner JH, Desai P, et al. The role of intraoperative frozen sections in revision total joint arthroplasty. J Bone Joint Surg Am. 1995;77:1807–1813. doi: 10.2106/00004623-199512000-00003. [DOI] [PubMed] [Google Scholar]
- 17.Altman DG. Comparing groups-categorical data. In: Altman DG, editor. Practical statistics for medical research. London: Chapman & Hall; 1991. pp. 229–276. [Google Scholar]
- 18.Palestro CJ, Love C. Radionuclide imaging of musculoskeletal infection: conventional agents. Semin Musculoskelet Radiol. 2007;11:335–352. doi: 10.1055/s-2008-1060336. [DOI] [PubMed] [Google Scholar]
- 19.Gemmel F, Dumarey N, Palestro CJ. Radionuclide imaging of spinal infections. Eur J Nucl Med Mol Imaging. 2006;33:1226–1237. doi: 10.1007/s00259-006-0098-2. [DOI] [PubMed] [Google Scholar]
- 20.Yapar Z, Kibar M, Yapar AF, et al. The efficacy of technetium-99m ciprofloxacin (Infecton) imaging in suspected orthopaedic infection: a comparison with sequential bone/gallium imaging. Eur J Nucl Med. 2001;28:822–830. doi: 10.1007/s002590100555. [DOI] [PubMed] [Google Scholar]
- 21.Kraemer WJ, Saplys R, Waddell JP, et al. Bone scan, gallium scan, and hip aspiration in the diagnosis of infected total hip arthroplasty. J Arthroplasty. 1993;8:611–616. doi: 10.1016/0883-5403(93)90008-r. [DOI] [PubMed] [Google Scholar]
- 22.McCarthy K, Velchik MG, Alavi A, et al. Indium-111-labeled white blood cells in the detection of osteomyelitis complicated by a pre-existing condition. J Nucl Med. 1988;29:1015–1021. [PubMed] [Google Scholar]
- 23.Abdoli M, de Jong JR, Pruim J, et al. Reduction of artefacts caused by hip implants in CT-based attenuation-corrected PET images using 2-D interpolation of a virtual sinogram on an irregular grid. Eur J Nucl Med Mol Imaging. 2011;38:2257–2268. doi: 10.1007/s00259-011-1900-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Reinartz P, Mumme T, Hermanns B, Cremerius U, Wirtz DC, Schaefer WM, Niethard F-, Buell U. Radionuclide imaging of the painful hip arthroplasty: positron-emission tomography versus triple-phase bone scanning. J Bone Joint Surg Br. 2005 Apr;87(4):465–70. doi: 10.1302/0301-620X.87B4.14954. [DOI] [PubMed] [Google Scholar]
- 25.van der Bruggen W, Bleeker-Rovers CP, Boerman OC, Gotthardt M, Oyen WJ. PET and SPECT in osteomyelitis and prosthetic bone and joint infections: a systematic review. Semin Nucl Med. 2010 Jan;40(1):3–15. doi: 10.1053/j.semnuclmed.2009.08.005. [DOI] [PubMed] [Google Scholar]
- 26.Zmistowski B, Della Valle C, Bauer TW, et al. Diagnosis of Periprosthetic Joint Infection. J Arthroplasty. 2013 Dec 15; doi: 10.1016/j.arth.2013.09.040. pii: S0883-5403(13)00721-3. Epub ahead of print. [DOI] [PubMed] [Google Scholar]