

Abstract
Background:
Today, much attention has been paid to the patient role as the central factor in the management of their own health. It is focused on the issue that the patient has a more critical role compared with the health-care provider in controlling the patient own health. defines health literacy as the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions.
Objective:
The objective of this study was to determine health literacy, health status, healthcare utilization and the relationship between them in 18 - 64 years old people in Isfahan.
Structure and Design:
This study was a descriptive analytical survey, which was conducted on 300 subjects of 18-64 years old in Isfahan with Multi-stage sampling method proportional to selected sample size.
Materials and Methods:
For collecting the data, questionnaire adapted from CHAP (Consumer Assessment of Healthcare Providers and Systems) health literacy questionnaire was used. Health status was measured based on an assessment of the physical and mental health over the past 6 months by 5° Likert scale. Data analysis was performed by using SPSS 18, descriptive statistics, Chi-square test and multivariate analysis of variance.
Results:
There was no significant correlation between health literacy, health status and healthcare utilization. Utilization was less in the urban area No. 6 of the city. In the bachelor's degree group, the health status was lower than the other groups in these cases: Older ages, married, women, large family size, undergraduates, and urban area No. 14.
Conclusions:
Due to the average prevalence of health literacy in 18-64 years old individuals in Isfahan and low- healthcare utilization, the followings are recommended: Necessity of more attention to the issue of health literacy, improving the physician-patient relationship and community awareness, whether through health promotion programs or media for the optimum use of available resources.
Keywords: Healthcare utilization, health literacy, health status
INTRODUCTION
Recently, much attention has been paid to the patient role as the central factor in the management of their own health. Words such as “centrality placement of the patient,” “diseases related to lifestyle,” “patient actions,” and “patient empowerment,” emphasis on this issue that the patient has a more critical role, comparing with the health-care provider in controlling his/her own health. This issue shows that the patient as an informed individual must participate in their health-care decisions.[1] Modern health and medical systems have created a range of different consumer health. Since, the self-management of health and medical care is grown; the people are looking for new roles to obtain information in order to understand their rights and accountability to adopt decisions about health concern for themselves and others. Subset of such a request is to accept that skills and knowledge.[2] Nevertheless, It seems that some of the patients have less knowledge of health and medical information. Studies have shown that 40-80% of medical information received by the patient is forgotten quickly and half of the remaining information is incorrect.[1] Health literacy the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. These items were included: Ability to understand instructions on prescription drug bottles, medical education brochures, consent forms, ability to use medical complex systems,[3] reading and listening skills, analysis, decision-making and the ability to apply these skills on the health status, not necessarily connected to the years of education or public reading.[4] World Health Organization (WHO) definition of health literacy is “Cognitive and social skills, and the ability of individuals to access the understanding and usage of the existing information in order to promote and maintain the good health.”[5] The issue of health literacy is clearly expressed in the map view of the health system in Islamic Republic of Iran at the 2025 horizon viewpoint. The Islamic Republic of Iran in 2025 will be a healthy and empowered society in accomplishment of 20-year vision. People in the community will enjoy health literacy (the ability to access information, analysis and decision-making power in the health field) and the desired level of the social capital.[6] In the goals of 2010 healthy people, it is presented that “health literacy is increasingly helping people to assess health information.”[7] The consequences of low-health literacy occur both directly and indirectly. Direct effects include indications or lack of medication errors. Indirect effects are more difficult to measure but may encompass issues such as insurance, having access to health-care services and poor health behaviors.[3] Low-health literacy can lead to social and economic disadvantages and may stop completely engaging people in the community and achieve their life goals.[5] The economic impact of low-health literacy, in addition to impact on people, its economic consequences also occur in the society.[5,8] National Academy of Geriatric Society of America has estimated that excess costs in health-care due to low-health literacy was about 73 billion dollars in 1998[8,9] which the amount included $ 30 billion for illiterates and 43 billion dollars for people with marginal health literacy.[3] Among adults who remain in hospital for more than one night, those with low-health literacy compared with those who have higher levels of health literacy, there is a 6% chance of staying in hospital for more than 2 days.[10] Other studies have shown that educated people use less emergency services; hospitalized more frequently, have less compatibility with the drugs, and have fewer benefits from preventive services.[5] Many studies have shown that low-health literacy is associated with weak health status and little knowledge about the prevention and treatment of diseases.[8,10,11,12] The individual features and behavioral patterns influence health status. However, continuous measurements show significant differences in terms of environmental, social, and economic conditions.[1] Health status is a general concept. This concept is beyond the presence or absence of the disease.[7] Health assessment by a person or self-rated health is an internationally recognized indicator. This index is used extensively for the measurement of health status in public health research and epidemiology. In fact, the health status assessment with an answer to a single question by the “WHO” and the “Euro-Reeves Organization” by conducting a project undertaken by the European Union in order to co-ordinate the health concept has been considered at the individual and the population level as one of the best indicators of measuring the health.[11] In other words, the measures of health status by themselves are predictor of consequences and health risks throughout life.[12] Undoubtedly, the process that health literacy affects health status is included:
Communicative competencies of health and medical care consumers, i.e., patients,
communication competencies of health and medical care service providers,
structural elements of messages, which affect understanding and the ability to use them,
the ability of navigability of the health system.[13]
Health literacy have a basic role in modern citizenship.[14] Despite the great importance of health literacy, this topic has received little attention in Iran. The need to address this issue and its dimensions can be used as an effective tool to help planners, administrators, and trustees. Little researches in this area are indicative of low-health literacy in Iran.[4,15] Even with regard to knowledge of health, comprehensive national studies that include aspects of health in literature review were less accessible. Due to the above description, necessity of conducting a study is quite evident in order to determine the health literacy status associated with health status and benefits from the services. Given that so far, no study has been carried out in Iran to assess health literacy, health status, and healthcare utilazition in the age range of 18-64 years. The present study was carried out for determining the relationship between health literacy, health status, and healthcare utilazition in the mentioned people in Isfahan in 2011.
MATERIALS AND METHODS
This study was a descriptive analytical survey and the used tool for collecting data was the Consumer Assessment of Healthcare Providers and Systems (CHAP) health literacy questionnaire,[16] which is one of the most prestigious questionnaires that have been validated as well. In this study at the first step, the questionnaire was translated and after checking out, the questions were selected based on the used concepts and variables in research hypothesis. According to the characteristics of our culture, the final questionnaire included 30 questions. In order to assess health literacy in the area of communication, the response range had 4° and it was scored from 1 to 4. Then, the sum was divided by the number of related questions and the mean was obtained. After designing the questionnaire prior to its final implementation, face validity was assessed first by some specialists in the fields of medicine, sociology, and health management. Afterwards, in a pilot study, the questionnaire was distributed among the 30 members of the community and due to the variance of the responses, the required changes applied to the questions. Again, the questionnaires were distributed among 30 people. Finally, the validity and reliability were confirmed. Hence, we used the Cronbach's alpha co-efficient and the reliability was assessed as good, for the items above 0.75. Health status was measured according to physical self-assessment and mental health over the past 6 months in a five-grade Likert scale from very high to very low. The mode of scoring was from 1 to 5. In this case, the total scores of the questions were divided in to the number of questions and were reported as mean scores of healthcare utilization. The people were asked in six domains (six questions), which included the number of visits to the general practitioner, number of visits to physician,[17] number of visits to the clinic or physician office, visits to Emergency Departments, the rate of using diagnostic services (laboratory, imaging, ultrasound, etc.) in the past 3 months and the rate of hospitalization in the past year. The responses range was from 0 to 5. The study population was 18-64 years old people of Isfahan. Among them, 300 subjects were selected with the test power of 84 and confidence level of 95% by multi-stage sampling method. For this purpose, the classified map of the city was produced. Among the 14 urban areas of Isfahan the three districts were randomly selected. These regions included urban area No. 4, urban area No. 6 and urban area No. 14. Due to the number of samples, 300 participants were divided equally between the three regions. Then, within each region, some neighborhoods (blocks) were selected randomly. The number of houses in each block was divided in to 10 and the number of distance within each block was approximately seven. Therefore, that, from the southeast of the desired block and in clockwise direction, the jump has started and the seventh house after that was selected as the next sample. Method of inquiry was door to door. By asking the home residents, in case of wishing to respond, if one of the residents was in the age range of our target, the questionnaire was completed by interview. In the absence of desired terms in each of the samples, the house would be deleted and the adjacent house was selected. Upon the completion of the data collection and performing the research, all necessary information has been verified and after making computer codes notebook based on the measured levels, the desired variables and items were coded and extracted. Data were analyzed by using SPSS software version18. Thus, all information was transferred to computer and necessary changes were made to indexes. Data were analyzed using both descriptive and inferential statistics. Descriptive statistics used frequency distribution tables and in evaluation of the relationships of the variables, crosstab tables descriptive statistics were used. Multivariate analysis of variance, Chi-square, Kendall and P-significance tests were used at the inference level.
RESULTS
Demographic
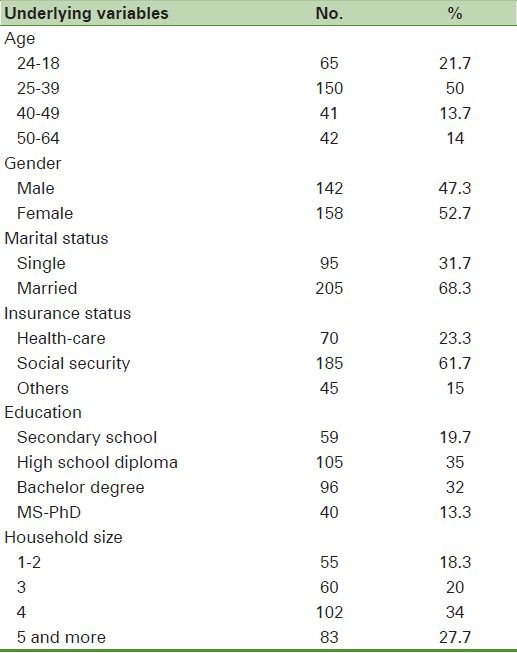
Table 1 shows the demographic characteristics of the studied samples. The results showed that 47.3% of the subjects were male and 52.7% were female. Subjects had a mean age of 33.93 ± 11.54. 68.3% of the subjects were married. Household size of most of the studied subject was 4 (34%). 19.7% of the subjects had secondary school education, 35% were high school graduates, 32% had a bachelor's degree, and 13.3% had MS or PhD. In terms of insurance coverage, 23.3% had health insurance, 61.7% social insurance, and 15% other insurances. The majority of the subjects (61.7%) were covered by social insurance [Table 1].
Table 1.
Demographic characteristics of the studied samples
Health literacy
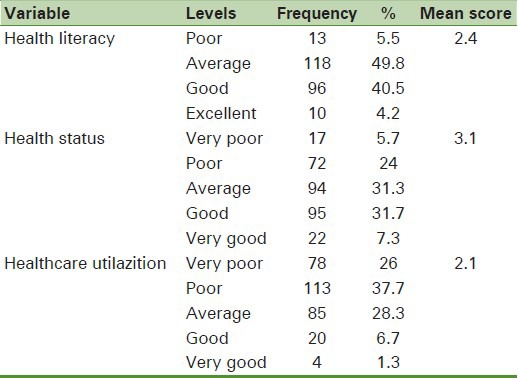
The results of the present study showed that the health literacy mean score in adults of Isfahan was 2.4 out of 4 and at the average level. About 49.8% of adults had average health literacy. The mean score of health status was 3.1 out of 5 and at the good level. The mean score of healthcare utilization was 2.1 out of 5, which would assessed as weak [Table 2].
Table 2.
Frequency distribution of health literacy, health status and Healthcare utilazition
The relationship between health literacy score with healthcare utilizationand health status in terms of demographic variables and insurance type
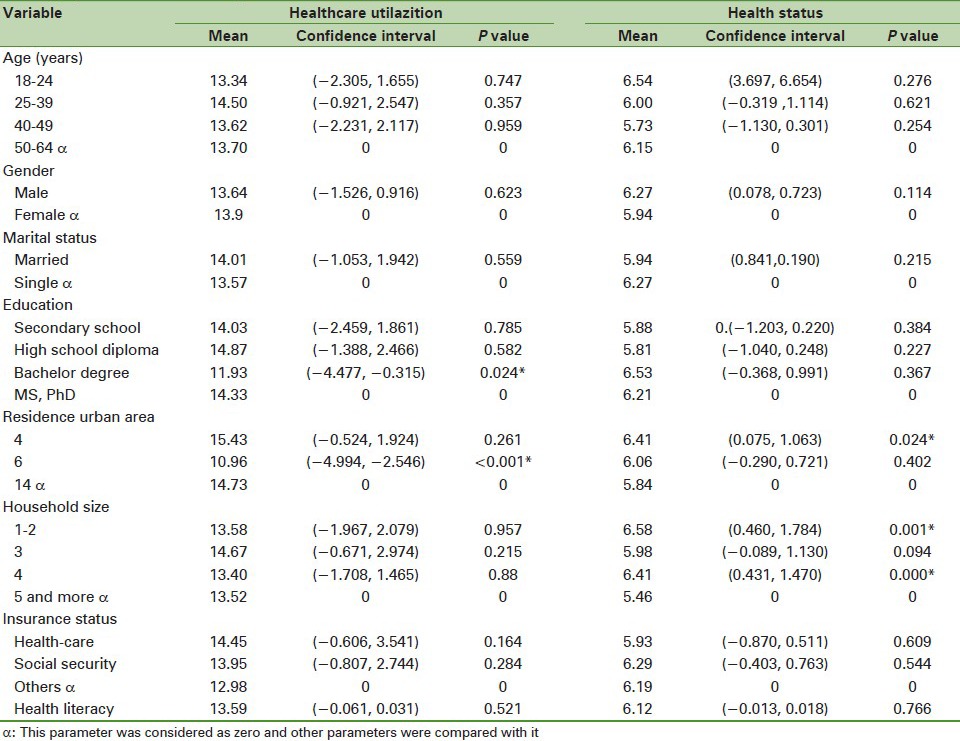
These variables were analyzed using multivariate ANOVA: Age, gender, education, household size, region of residence, marital status, type of insurance, health literacy score, healthcare utilization score, and health status score. The results are presented in Table 3. Based on the results in Table 3, there was no significant statistical relationship between health literacy, health status, and healthcare utilization. Educational level and area of residence were effective in the healthcare utilization of the people from the health services. healthcare utilization in urban area No. 6 and in undergraduate group were lower. household size was effective in the health status of people. The health status was lower in these subjects than other groups: Older people, married people, women, upper household size, secondary-school education group, and urban area No. 14.
Table 3.
The relationship between health literacy with Healthcare utilazition and health status in terms of demographic variables and type of insurance
The relationship between health literacy levels with healthcare utilazition
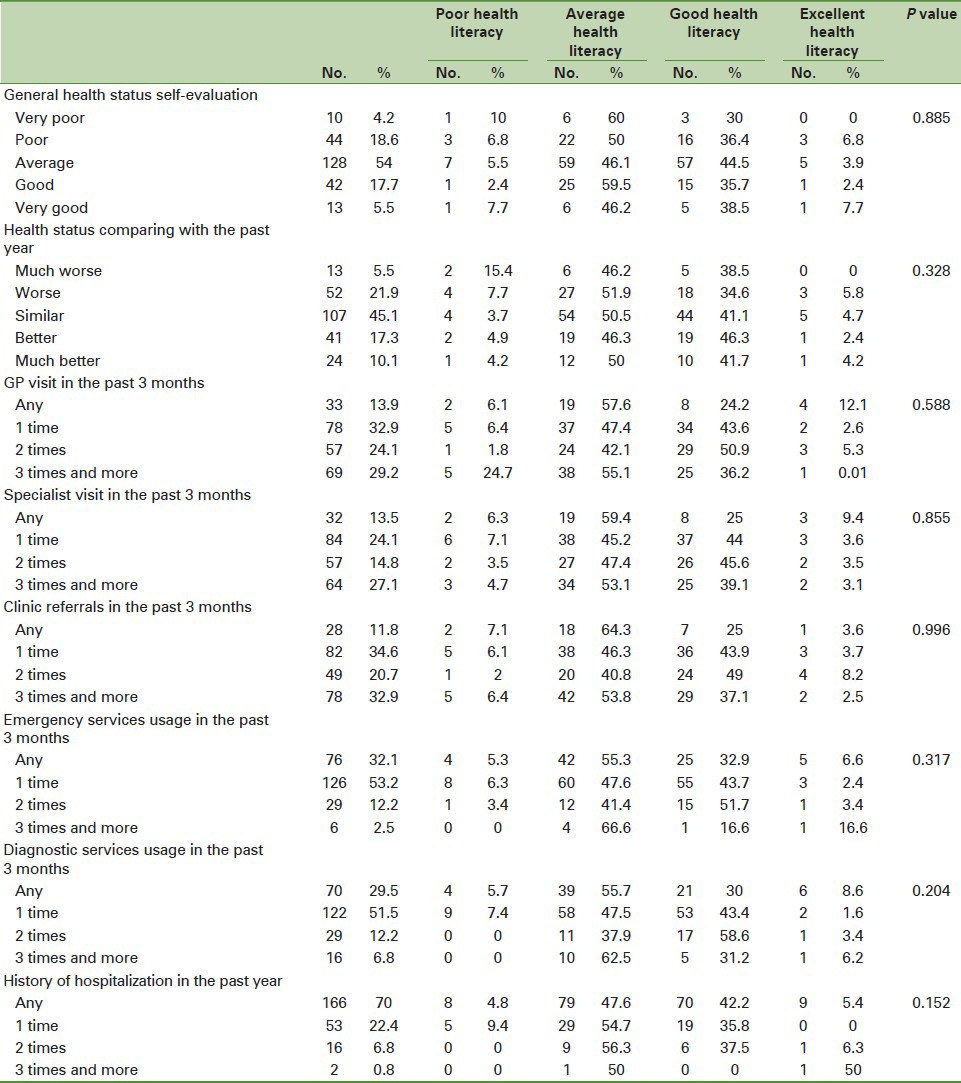
According to the results in Table 4, in the poor health literacy levels, these items were found: More than three visits to the general practitioner (24.7%), one visit to a specialist (7.1%), one visit to the emergency department (6.3%), one-time use of diagnostic services (7.4%) in the past 3 months and a history of hospitalization (9.4%) over the past year. Some of them had no visit to the clinic (7.1%). These results were not statistically significant. In the average level of health literacy, most people did not visit a general practitioner (57.6%), specialist (59.4%), and clinic (64.3%). The following items were also observed: More than three times referrals to the Emergency Department (66.6%), more than three times using the diagnostic services (62.5%) during the last 3 months and two previous hospitalizations (56.3%) during the past year. In the good health literacy levels in most people, these items were observed: Two visits to a general practitioner (50.9%), twice visits to specialist (45.6%), two visits to clinic (49%), two visits to the Emergency Department (51.7%), two applications of diagnostic services (58.6%) during the last 3 months. They had no history of hospitalization (56.3%) during the past year. There was no statistically significant relationship. Based on the results in Table 4, in the higher levels of health literacy, most people did not visit a general practitioner (12.1%) and specialist (9.4%) during the last 3 months without any use of diagnostic services (58.6%) in this period. Most of the people had these items: Twice visits to clinic (8.2%), more than three times visits to the Emergency Department (16.6%) during the last 3 months and more than three times of hospitalization (50%) during the past year. There was no statistically significant relationship. In this section, Chi-square and Kendall statistical tests showed no significant correlation between the health literacy with the number of visits to general practitioner, specialist, clinic, Emergency Department, diagnostic services, and admission to the hospital.
Table 4.
Relationship between general health status healthcare utilization with health literacy in adults of Isfahan
The relationship between health literacy levels and the health status
Based on the results in Table 4, in the poor health literacy levels, most people have stated their own health status as poor (6.8%) and for most people; their health status compared with past year evaluated worse (15.4%), which was not significant. In the average level of health literacy, most people have well noted their own health (46.2%) and they better assessed their health status compared with past year (46.3%). In the good health literacy levels, most people have stated their health as moderate (44.5%) and they better assessed their health status compared with past year (46.3%). At the higher levels of health literacy, most of them stated their own health status very good (7.7%) and for most people; their health status compared with past year evaluated worse (5.8%), which was not statistically significant. In this section, Kendall and Chi-square statistical tests showed no significant correlation between levels of health literacy and health status [Table 4].
DISCUSSION
The findings of the present study showed the mean age of participants was 33.93 ± 0.1. 47.3% of the subjects were male and 52.7% were female. These items were also obtained: The mean score of health literacy was 2.4 and at the average level, the mean score of health status was 3.1 and at the good level, the mean score healthcare utilazition was 2.1 and at the poor level. There was no significant correlation between health literacy, health status, and healthcare utilazition. Educational level and area of residence were effective on people healthcare utilazition. These healthcare utilazition were less in urban area No. 6 and also in the bachelor's degree group. Household size was effective in the health status of people: Qlder people married people, women, upper household size, secondary-school degree group, and urban area No. 14. The results indicated that there was no significant relationship between health literacy level and physician visit. The results were consistent with other studies that showed no significant correlation between health literacy levels and out-patient visits to physicians.[18,19,20] However, in some studies, there was a significant correlation between the health literacy level and the use of health services,[9,15,21,22] which was not consistent with this study. In Nancy et al. study, one time physician's visit was not associated with health literacy,[23] which was consistent with the present study. Due to the differences in the studied population in the mentioned studies and the present study, the results could be different. Because the characteristics of each community health system, awareness level of people and provided training were effective in the benefits from the services. These factors could provide the difference field of the studies’ results. According to the study of David et al., inadequate health literacy had very low, or no relationship between the total numbers of out-patient visits among people covered by managed care Medicare.[24] In the Walker et al. study and in the study of Raeisi et al. achieved a positive relationship between health literacy and probability of visit to a physician.[15,22] In the study of Lee et al., there was a negative relationship between the health literacy levels and out-patient visits.[25] The results of this study were consistent with other researches, which have studied the younger people and the uninsured patients. Their findings showed that there were not any independent relationships between the health literacy with the number of out-patient visits as reported by the patients themselves during the past 3 months.[9,20] The results of another study were also consistent with the findings of the present study. In that study were shown that in Los Angeles, health literacy levels were not related to the number of physician visits in the past 3 months. However, in Antalya, the patients with inadequate health literacy compared with patients with adequate health literacy, had more visits to the physician in the past 3 months (69% vs. 61.2%). They also met the physician for two or more times (44.4% vs. 36.9%). However, in this study, after excluding the impact of other variables on health literacy, there was no difference between the usages of out-patient care due to the levels of health literacy.[9] The results of Nancy et al. study showed that out-patient services had less significant association with higher health literacy. In fact, the numbers of out-patient admissions were reduced by increasing health literacy,[23] which was not consistent with our study. Many of out-patient visits were not due to the real cause of disease, but they have been carried out according to undue concerns of the patients and their families or the suggestions of the community, the media and even the health system. However, by increasing the health literacy, the amount of unnecessary out-patient visits has been reduced. In the present study, there was no significant correlation between health literacy levels and referring to emergency departments. This result has been confirmed in other studies.[15,25] In the study of Lee et al., there was no significant relationship between health literacy levels and emergency department referrals.[25] However, in other studies, this relationship was significant.[20,22] It should be noted that these studies have used different tools to measure health literacy. This makes it difficult to compare their results with the present study. In the study of Cho et al., emergency departments’ visits have been decreased dramatically by increasing health literacy. Increasing health literacy was associated with a 60% reduction in emergency department referrals.[18] People with inadequate health literacy scores were more willing to receive emergency services.[26] In the study of David et al., people with inadequate and average health literacy compared with those with adequate health literacy were more likely to visit emergency departments. The referrals to emergency department were as the followings: 21.8% of those with adequate health literacy, 27.6% of those with average health literacy, and 30.4% of those with inadequate health literacy. This trend was also statistically significant,[24] whereas in our study, there was no significant difference in emergency department referrals in various levels of health literacy. This fact shows that in our country, health literacy has not an important role for referring to emergency department. Perhaps the reason is easy access to emergency services, because the people, even for ordinary diseases, such as colds, in any time, day or night, ensure that they are able to use the available city emergency services or the hospitals’ emergency departments. In addition, 15% of those with adequate health literacy, 15.3% of those with average health literacy and 17% of those with inadequate health literacy had an emergency department visit. 6.8% of those with adequate health literacy, 12.3% of those with average health literacy and 13.4% of those with inadequate health literacy had two or more referrals to emergency department.[24] There was no significant relationship between health literacy levels and hospitalization in the present study, but the results of Walker study showed a significant inverse relationship between health literacy and frequency of hospitalization. For example, people with lower levels of health literacy compared with those with higher levels of health literacy had more frequent hospital admissions.[22] This significant relationship has also been obtained in a number of other studies.[9,15,21] In the study of Baker et al., it was shown that those with average health literacy (33.9%) and inadequate (34.9%) compared with those with adequate health literacy (26.7%) had more likely to stay in hospital. It was a significant relationship. Those with average health literacy (17.8%) and inadequate (19.9%) compared with those with adequate health literacy (14%) were more likely to have had two or more hospitalizations. This relationship was significant. People with inadequate health literacy (52%) had more likely to stay in hospital.[9] However, the impact of inadequate health literacy on hospitalization rate was dependent on factors such as the characteristics of the patients and the health-care system. In particular, inadequate health literacy is higher for the people who face management barriers to obtain caring.[9] In Los Angeles, literacy level was not significantly associated with hospitalization.[21] It could be noted that some indicators (in total), show the benefits of the health system, such as: The number of physician visits, emergency department visits and hospitalizations. In this study, we found no significant relationship generally between the levels of health literacy and the benefits, which was consistent with the findings of Lee et al. study.[25] Using the out-patient visits is one of the earliest indicators of access to health and medical care. Total number of out-patient visits is a partial index for accessing to care. There are greater barriers in this regard such as lack of health insurance, which usually seen in fewer out-patient visits. The results of the study showed that inadequate health literacy was not considered as a major obstacle to access to health and medical care. This result was consistent with the previous studies, which those with inadequate health literacy and those with adequate health literacy expressed the same access to care problems.[20] The results showed that the relationship between literacy and health did not justify using less health-care. In any case, it could say that patients with low-literacy use fewer services compared to the required level. Patients with low-literacy may receive ineffective caring and because they do not fully understand the health-care providers guidance. Therefore, may be they need to have more visits in order to achieve the same therapeutic target.[9] In this study, we found no significant correlation between the mean score of health literacy and health status. This lack of communication could be due to this fact that health status is some sort of self-evaluation health report by the people. However, in health literacy, we have investigated about the scope of the patient-physician relationship. Other studies have confirmed this lack of communication.[9,27] A study was conducted among African Americans and Latinas and showed that there was no connection between these two.[27] However, this correlation has been reported significant in many studies.[5,8,9,11,22,26,28,29,30,31,32] In the study of Wolf et al., people with inadequate health literacy levels have reported significantly less mean than their own mental and physical health. The relationship between inadequate health literacy increases the weaker physical health.[31] In another study it has been reported that people with higher levels of health literacy had more information about their health status. Overall, there is a direct correlation between health literacy and health status.[22] In adult Medicare population, inadequate health literacy was associated with weak physical functioning and mental health.[26,31] A study was conducted on adult Japanese showed that poor health literacy was associated with weak physical and mental health status.[29] Inadequate health literacy was significantly correlated with weak mental health self-report. This finding is surprising, because most studies have shown significant relationship between health literacy and self-reported health status.[25] In the study of Raeisi et al., people with higher health literacy better assessed their general health status.[15] Inadequate health literacy strongly influence on patient knowledge, self-care in heart disease, health status and risk of hospitalization.[21]
CONCLUSIONS
Findings from this study have significant impact in improving the communication skills of providers and recipients of services, state of health and effective use of resources. The end result can be the improvement of public health. Due to the results of this study, which showed that the average prevalence of health literacy in the adults of Isfahan and low-benefit from health services. It is clear that more attention to health literacy and improving the physician-patient relationship. It is recommended the public awareness through health promotion programs or media for optimal use of available resources. One of the limitations of this study was self-reporting of the responses and collected information. It is likely, the individuals evaluated their own health status mentally and it was not an ongoing objective process for all of the respondents. Further researches in the field of health literacy can check these items as well: Race, ethnicity, cultural traditions and their impact on health literacy, health status and benefit from the health services. It is suggested that in future studies to review the health literacy in different diseases. By investigating the effects of mass media in improving, the health behaviors can help to improve those behaviors and thus, promoting the health. The relationship between health literacy and self-reported health status should be interpreted with caution. Self-reported health status is only a single item for measuring general health perceptions. Therefore, it is recommended to study the details of health status. In addition, personal questions and health status measures in patients with low-literacy should be checked for validity, in order to be sure that differences in self-reported health status is not due to differences in the method of response among patients with low-literacy and patients with adequate literacy.[9]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.North Carolina: North Carolina department of health and human services: The North Carolina Institute of Medicine; 2007. Just what did the doctor order? Addressing low health literacy in North Carolina. [Google Scholar]
- 2.Tsai TI, Shoou-Yih D, Lee, Yi-Wen Tsai, Ken N, Kuo . J Health Commun. The George Washington University; 2009. Methodology and validation of health literacy scale development in Taiwan; pp. 1–26. [DOI] [PubMed] [Google Scholar]
- 3.Report on the Council of Scientific Affairs, Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs. American Medical Association. 1999 [PubMed] [Google Scholar]
- 4.Tehrani Bani-Hashemi A, et al. Health Literacy in five provinces of the country and its influencing factors. J Med Educ Develop Center. 1386;4:1–9. [Google Scholar]
- 5.Kickbusch I, Wait S, Daniela M. Navigating health: The role of health literacy. European Public Health Centre. Gastein Health Declaration. 2005:1–22. [Google Scholar]
- 6.Montazeri A, Goshtasebi A, Vahdaninia M. Educational inequalities in self-reported health in a general Iranian population. BMC Res Notes. 2008;1:50. doi: 10.1186/1756-0500-1-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Washington, DC: Public Health Service US Department of Health and Human Service; 1998. Healthy People 2010 Objectives: Draft for Public Comment. [Google Scholar]
- 8.Williams MV, Baker DW, Parker RM, Nurss JR. Relationship of functional health literacy to patients› knowledge of their chronic disease. A study of patients with hypertension and diabetes. Arch Intern Med. 1998;158:166–72. doi: 10.1001/archinte.158.2.166. [DOI] [PubMed] [Google Scholar]
- 9.Baker DW, Parker RM, Williams MV, Clark WS, Nurss J. The relationship of patient reading ability to self-reported health and use of health services. Am J Public Health. 1997;87:1027–30. doi: 10.2105/ajph.87.6.1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Report on the Council of Scientific Affairs. Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs, American Medical Association. JAMA. 1999 Feb 10; [PubMed] [Google Scholar]
- 11.Gazmararian JA, Baker DW, Williams MV, Parker RM, Scott TL, Green DC, et al. Health literacy among Medicare enrollees in a managed care organization. JAMA. 1999;281:545–51. doi: 10.1001/jama.281.6.545. [DOI] [PubMed] [Google Scholar]
- 12.Netherlands, Copenhagen: WHO Regional Office for Europe. World Health Organization, Statistics; 1996. Health interview surveys: Towards international harmonization of methods and instruments, WHO Regional Publications, European Series. [PubMed] [Google Scholar]
- 13.Manderbacka K, Kåreholt I, Martikainen P, Lundberg O. The effect of point of reference on the association between self-rated health and mortality. Soc Sci Med. 2003;56:1447–52. doi: 10.1016/s0277-9536(02)00141-7. [DOI] [PubMed] [Google Scholar]
- 14.Rubin DL, Parmer J, Freimuth V, Kaley T, Okundaye M. Associations between older adults› spoken interactive health literacy and selected health care and health communication outcomes. J Health Commun. 2011;16:191–204. doi: 10.1080/10810730.2011.604380. [DOI] [PubMed] [Google Scholar]
- 15.Raeisi M, Mostafavi F, Hasanzade A, Sharifirad GR. The relationship between health literacy, health status and healthy behaviors among elderly in Isfahan. Iran J Health Syst Res. 2011;4:469–80. [Google Scholar]
- 16.About the CAHPS Item Set for Addressing Health Literacy. CAHPS Clinician & Group Survey and Reporting. 2009:1–8. [Google Scholar]
- 17.Ebadifardazar F, Rezapour A, Abbasibroujeni P, Safari H, Moeeninaeeni M. Utilization of health care services in the state of Isfahan. Hospital J. 1390;10:1–10. [Google Scholar]
- 18.Cho YI, Lee SY, Arozullah AM, Crittenden KS. Effects of health literacy on health status and health service utilization amongst the elderly. Soc Sci Med. 2008;66:1809–16. doi: 10.1016/j.socscimed.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 19.Arozullah AM, Lee SY, Khan T, Kurup S, Ryan J, Bonner M, et al. The roles of low literacy and social support in predicting the preventability of hospital admission. J Gen Intern Med. 2006;21:140–5. doi: 10.1111/j.1525-1497.2005.00300.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Baker DW, Gazmararian JA, Williams MV, Scott T, Parker RM, Green D, et al. Health literacy and use of outpatient physician services by Medicare managed care enrollees. J Gen Intern Med. 2004;19:215–20. doi: 10.1111/j.1525-1497.2004.21130.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Baker DW, Gazmararian JA, Williams MV, Scott T, Parker RM, Green D, et al. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am J Public Health. 2002;92:1278–83. doi: 10.2105/ajph.92.8.1278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Walker J, Pepa C, Gerard PS. Assessing the health literacy levels of patients using selected hospital services. Clin Nurse Spec. 2010;24:7–31. doi: 10.1097/NUR.0b013e3181c4abd0. [DOI] [PubMed] [Google Scholar]
- 23.Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: An updated systematic review. Ann Intern Med. 2011;155:97–107. doi: 10.7326/0003-4819-155-2-201107190-00005. [DOI] [PubMed] [Google Scholar]
- 24.Nielsen-Bohlman L, Panzer AM, Kindig DA. Institute of Medicine of the National Academies. NW, Washington: National Academies Press; 2004. Health literacy: A prescription to end confusion; pp. 1–2. 500 Fifth St. [PubMed] [Google Scholar]
- 25.Lee SY, Tsai TI, Tsai YW, Kuo KN. Health literacy, health status, and healthcare utilization of Taiwanese adults: Results from a national survey. BMC Public Health. 2010;10:614. doi: 10.1186/1471-2458-10-614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hardie NA, Kyanko K, Busch S, Losasso AT, Levin RA. Health literacy and health care spending and utilization in a consumer-driven health plan. J Health Commun. 2011;16:308–21. doi: 10.1080/10810730.2011.604703. [DOI] [PubMed] [Google Scholar]
- 27.Guerra CE, Shea JA. Health literacy and perceived health status in Latinos and African Americans. Ethn Dis. 2007;17:305–12. [PubMed] [Google Scholar]
- 28.Jovic-Vranes A, Bjegovic-Mikanovic V, Marinkovic J. Functional health literacy among primary health-care patients: Data from the Belgrade pilot study. J Public Health (Oxf) 2009;31:490–5. doi: 10.1093/pubmed/fdp049. [DOI] [PubMed] [Google Scholar]
- 29.Tokuda Y, Doba N, Butler JP, Paasche-Orlow MK. Health literacy and physical and psychological wellbeing in Japanese adults. Patient Educ Couns. 2009;75:411–7. doi: 10.1016/j.pec.2009.03.031. [DOI] [PubMed] [Google Scholar]
- 30.Kutner M, Greenberg E, Jin Y, Paulsen C. The Health Literacy of America's Adults. Results From the 2003. National Assessment of Adult Literacy [Google Scholar]
- 31.Wolf MS, Gazmararian JA, Baker DW. Health literacy and functional health status among older adults. Arch Intern Med. 2005;165:1946–52. doi: 10.1001/archinte.165.17.1946. [DOI] [PubMed] [Google Scholar]
- 32.Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Viera A, Crotty K, et al. Health literacy interventions and outcomes: An updated systematic review. Evid Rep Technol Assess (Full Rep) 2011;11:1–232. [PMC free article] [PubMed] [Google Scholar]