

Abstract
Background
Alcohol dependence is associated with poor decision-making under ambiguity, that is, when decisions are to be made in the absence of known probabilities of reward and loss. However, little is known regarding decisions made by individuals with alcohol dependence in the context of known probabilities (decision under risk). In this study, we investigated the relative contribution of these distinct aspects of decision making to alcohol dependence.
Methods
Thirty recently detoxified and sober asymptomatic alcohol-dependent individuals, and thirty healthy control participants were tested for decision-making under ambiguity (using the Iowa Gambling Task), and decision-making under-risk (using the Cups Task and Coin Flipping Task). We also tested their capacities for working memory storage (Digit-span Forward), and dual-tasking (Operation-span Task).
Results
Compared to healthy control participants, alcohol-dependent individuals made disadvantageous decisions on the Iowa Gambling Task, reflecting poor decisions under ambiguity. They also made more risky choices on the Cups and Coin Flipping Tasks reflecting poor decision-making under risk. In addition, alcohol-dependent participants showed some working memory impairments, as measured by the dual tasking, and the degree of this impairment correlated with high-risk decision-making, thus suggesting a relationship between processes sub-serving working memory and risky decisions.
Conclusion
These results suggest that alcohol dependent individuals are impaired in their ability to decide optimally in multiple facets of uncertainty (i.e., both risk and ambiguity), and that at least some aspects of these deficits are linked to poor working memory processes.
Keywords: Addiction, alcohol, decision-making, ambiguity, risk, working memory
Introduction
Alcohol dependent individuals exhibit poor decision making as reflected by their continued alcohol use despite encountering problems directly linked to these drinking habits (APA, 2013). This aberrant profile of decision-making has been further evidenced in laboratory settings, through, for instance, the use of the Iowa Gambling Task (IGT; Bechara et al., 1994). A key feature of the IGT is that participants have to forgo short-term benefits for long-term benefits, a process that is presumably severely hampered in substance (e.g. drugs, alcohol, tobacco) and non-substance addictions (e.g. gambling) (Noël et al., 2013). For instance, a high proportion of alcohol-dependent patients detoxified and abstinent from alcohol for a few weeks (e.g. Kornreich et al., 2013; Noël et al., 2007) or even for several years (Fein et al., 2004) make more choices than healthy participants that bring immediate reward, but then lead to more severe delayed punishment. These findings highlight that impaired decision-making process measured by the IGT does not recover over time, i.e., after abstinence from using alcohol and may impact on the risk of relapse even after months and years.
One limitation of these findings is that they cannot be generalized to the general spectrum of situations of decision-making under uncertainty. Indeed, depending on the quality of information available for elaborating a decision, decisional context could be totally ambiguous because of the absence of any useful information to anticipate a given outcome or a risk could be estimated, because of either provided to the decision-maker (e.g., one chance in two to win) or calculated through practice (e.g. Kahneman and Tversky 1979). The IGT represents a complex task, for which a number of cognitive and affective processes are involved (e.g., working memory, episodic memory, inhibition, mental flexibility, automatic emotional activation during the deliberation phase; Dunn et al., 2006). Even though in the latter trials of the IGT (e.g., from trials 60 to 100; Brand et al, 2006; Brevers et al., 2012) the subject may acquire some sense of the probabilities of reward and loss, thus requiring mental calculation, working memory, the knowledge of these probabilities is not explicit and remains largely unknown (notion of ambiguity), thus requiring an decision-maker to rely more on intuition and emotion than on the logic (Bechara et al., 1997). Other tasks are more direct measures of risk taking because probabilities of reward and loss are simply given to the participant (e.g., the Cups task, Levin et al., 2007; the Coin Flipping Task, Tom et al., 2007). So far, only one study has examined decision-making under risk in alcohol-dependent individual (Bowden-Jones et al., 2005) using the Cambridge Gambling Task (Rogers et al., 1999), which provides choices with explicit probabilities of risk, i.e., it measures decisions under risk. The study found alcohol-dependent individuals exhibit a stubborn preference for options featuring high but uncertain rewards instead of options featuring lower but certain rewards (Bowden-Jones et al., 2005).
In light of the limited research, further studies were needed in order to provide a close contrast between impairments of decision-making under ambiguity and under risk in alcohol dependence, as both situations decision-making under risk account for poor decision-making outside of the laboratory. As an example of decision-making under risk, an alcohol-dependent has to reach a metro-station and has to choose between a short-length walk but with plenty of alcohol-liquor stores throughout (low physical effort but high risk of relapse) or a longer but “alcohol-safe” path. As an example of decision-making under ambiguity, an alcohol-dependent has to decide whether to go or not to a party, he has to take into account that he want to meet his friends (who are supportive with regard to his alcohol problem) but that he also might have to resist to different alcohol-proposals made by individuals who are not aware of his alcohol-problem.
In addition, based on this theoretical distinction and on the literature showing that alcohol-dependent individuals exhibit a number of cognitive impairments affecting distinct domains of executive functioning (for a review, see Noël et al., 2010), a number of hypotheses could be put forward. Indeed, deteriorations in emotional and/or rational processes could alter differently decision-making. For instance, because it does not offer explicit rules on probabilities, decision-making under ambiguity has to be made through the reactivation of previous experiences of rewards and losses (Brand et al, 2006; Krain et al., 2006). By contrast, making a decision under risk, which offers explicit rules for reinforcement and punishment, would involve both the integration of pre-choice emotional processes and rational analytical system aspects that require the capacity to represent a dilemma, maintain and organize information in working memory, strategically plan and execute a response, and to evaluate the efficacy of the solution (Brand et al, 2006; Krain et al., 2006). This idea is supported by data showing that advantageous decision-making under risk (Starcke et al., 2011), but not under ambiguity (Turnbull et al., 2005), is lowered when subjects have to take a decision while concurrently performing a secondary task (random number generation), which is known to load on executive resources (Baddeley and Della Sala, 1996). Neuroimaging data also support this distinction. Indeed, on the one hand, decision-making under ambiguity and under risk may be associated with activity in the orbito-frontal and the ventromedial prefrontal cortex with regard to the use of feedback to improve decision-making (Paulus et al., 2001). On the other hand, decision-making under risk, but not under ambiguity, depends on the integrity of the dorsolateral prefrontal loop (Brand et al., 2006). These regions are critical for the exercise of executive control (Kerr and Zelazo, 2004; Starcke et al., 2011), which is also considered a specific process of working memory (Baddeley and Della Sala, 1996).
Importantly, neuropsychological studies have repeatedly highlighted that alcohol dependence is associated with impaired executive functioning, including working memory, planning, and flexibility (e.g. Blume et al., 2005; Doa-Castellana et al., 1998; Noël et al., 2001). These disorders constrain the possibilities of flexible changes of action strategies, reduce behavior control and suppress psychosocial adaptation abilities, which might in turn impair decision-making under risk.
The aim of this study was to examine the capacity of alcohol-dependent individuals to make decisions under risk and under ambiguity. We hypothesized that, as compared with healthy controls, alcohol-dependent individuals exhibit a disadvantageous decision-making profile in both decision-making under risk and under ambiguity. In addition, we hypothesized that advantageous decision-making under risk is associated with the capacity to maintain and organize information in working memory (as an estimation of executive processes), for which alcohol-dependent individuals are impaired.
Methods
Participants and recruitment
Thirty recently detoxified alcoholic and thirty healthy controls participated in the study. All subjects were adults (> 18 years old).
Alcohol dependent participants were recruited for this study from the Alcohol Detoxification Program of the Psychiatric Institute, Brugmann Hospital, Free University of Brussels, Brussels, Belgium. Participants had to meet Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM–IV; American Psychiatric Association, 1994) criteria for alcohol dependence (made by Paul Verbanck, a board-certified psychiatrist). Reasons for exclusion were other current DSM–IV Axis I diagnoses, a history of significant medical illness, head injury resulting in a loss of consciousness for longer than 30 minutes that might have affected the central nervous system, use of other psychotropic drugs or substances that influence cognition, and overt cognitive dysfunction. Subjects were examined after they had abstained from alcohol for a minimum of 18 days and at least 5 days after a standard detoxification period. The detoxification regimen consisted of B vitamins and decreasing doses of sedative medication (diazepam). All received complete medical, neurological, and psychiatric evaluations prior to enrolment in the study.
Participants from the control group were recruited by word of mouth from the community. Before being enrolled in the study, controls were first asked to complete a brief pre-screening tool estimating drug and alcohol use. Control participants were excluded if they reported to consume drugs within the past twelve months. With regard to alcohol consumption, controls were asked: (1) to estimate the maximum consecutive number of days they had consumed an alcohol beverage within the past 10 years; (2) to estimate the average quantity per days consumed; and (3) to report the type of alcohol beverage. Quantity and type of alcohol beverage were indexed with pictures (i.e., half pint of beers; half-pint of strong beers; 175ml glass of wine; 25ml glass of spirit; 275ml bottle of alcopops). We excluded subjects who consumed more than 54g/day of alcohol (i.e., four half pints of beers; two half pints of strong beers; two 175ml glasses of wine; three 25ml glasses of spirit; three 275ml bottles of alcopops) for longer than 30 days.
Current clinical status
Current clinical status was rated with the Beck Depression Inventory (Beck et al., 1967) and the Spielberger State–Trait Anxiety Inventory (STAI; Spielberger, 1993). The number of cigarettes per day was also included to control from some nicotine effects on cognitive processing (e.g., sustained attention; Heishman, 1998).
Decision making tasks
Decision making under ambiguity: the Iowa Gambling Task. (Bechara et al., 1994)
Because this task does not provide any information about the probabilities of reward or loss, nor the value of a given reward or loss, it is thought that this task taxes primarily the process of decision-making under ambiguity. In the IGT, participants sat in front of four decks of cards that were identical in appearance, except for their labels A, B, C and D. They were told that the game involved a long series of pack selections and wagers and that the goal was to earn as much money as possible. Participants were informed that each trial would consist of (1) a pack selection and (2) the turning over of one card from the selected pack to reveal the yield. Participants were informed that they were free to switch between decks at any time, and as often as desired. The net outcome of choosing from either decks A or B was a loss of five times the average per ten cards (referred to as disadvantageous decks), and the net outcome of choosing from either decks C or D was a gain of five times the average per ten cards (referred to as advantageous decks). The total number of trials was set at 100 card selections. The dependent measure for advantageous choice was the number of cards picked from the advantageous decks in each block of 20 cards.
Decision making under risk: the Coin Flipping Task
This task is an adaptation of a decision making task developed by Tom, Fox, Trepel, and Poldrack (2007), and it was used in this study to examine decision making under risk with fixed probabilities. Participants decided whether to accept or reject mixed gambles that offered a 50/50 chance of either gaining a given amount of money, or losing another amount. To encourage participants to reflect on the subjective attractiveness of each gamble rather than to rely on a fixed decision rule, we asked them to indicate one of four responses to each gamble (strongly accept, weakly accept, weakly reject, and strongly reject). The size of the potential gain and loss were manipulated independently, with gains ranging from €10 to €40 (in increments of €2), and losses ranging from €5 to €20 (in increments of €1), resulting in 256 random trials. The dependent measure of the Coin Flipping Task was the participant's gamble acceptance for six computed win/loss ratio that include trials in which (1) potential gain equal the potential loss, trials where potential gain was maximum (2) twice, (3) twice point five, (4) thrice, (5) four times or (6) eight times the amount of the potential loss. These ranges were chosen because previous studies indicate that people are, on average, roughly twice as sensitive to losses as to gains (i.e. loss aversion; Kahneman and Tversky, 1979). Thus, we expected that this range of gambles would elicit a wide range of attitudes, from strong acceptance to indifference to strong rejection.
The Cups Task (Levin et al., 2007)
This task investigates decision-making under risk with both known probability and known value of reward and loss. This task includes a Gain domain, which consists of gain trials, with a choice between a sure gain and a gamble with a possible larger gain or no gain, and a Loss domain, which consists of loss trials with a choice between a sure loss and a gamble with a possible larger loss or no loss.
For both Gain and Loss domains trials, subjects were required to choose between the risky and the safe option. The safe option is to win or lose €1 for sure, whereas the risky option in the Gain domain could lead to a probability (0.20, 0.33, or 0.50) of a larger win (€2, €3, or €5) or could lead to no win. In the Loss domain, a risky choice could lead to a probability (0.20, 0.33, or 0.50) of losing more (€2, €3, or €5) or could lead to losing nothing. Probability levels and amounts of possible win or loss vary between trials. Hence, the expected value (EV) for the risky option shifts from more favourable to less favourable (see Table 1).
Table 1.
Expected value (EV) for the risky option on Gain and Loss domain of the Cups task according to probability level (P) and amount (in euro).
| Gain domain | Loss domain | |||
|---|---|---|---|---|
| P | € | P | € | |
| Risk advantageous EV | 0.33 | 5 | 0.20 | 3 |
| 0.50 | 3 | 0.33 | 2 | |
| Risk equal EV | 0.20 | 5 | 0.20 | 5 |
| 0.33 | 3 | 0.33 | 3 | |
| 0.50 | 2 | 0.50 | 2 | |
| Risk disadvantageous EV | 0.20 | 3 | 0.33 | 5 |
| 0.33 | 2 | 0.50 | 3 | |
On each trial, an array of 2, 3, or 5 cups is shown on one side of the screen, with the possible gain or loss shown on top. This array is identified as the risky side where selection of one cup out of the total number of cups will lead to a designated number of euros gained (or lost) whereas a selection of the other cups will lead to no gain (or no loss). After participants made the choice, the gamble was resolved immediately, allowing them to experience the consequence of the risky or safe choice.
Gain and loss domains were presented as two separate blocks of 27 random trials, counterbalanced in order across participants in each group. There were 3 trials for each combination of domain, probability, and outcome magnitude. When the participant completed all 54 trials, their total amount won appeared on the screen. The dependent measure was the number of risky choices at each of three EV level (risk advantageous, risk equal, risk disadvantageous; see Table 1) for both the Gain and the Loss domains.
Working memory
Working memory was assessed using two tasks: (1) the Digit span task (forward), which is a widely used neuropsychological test that quickly evaluates working memory capacity by determining the maximum length of numbers that participants can serially recall; and (2) the Operation-span Task (Ospan; Turner and Engle, 1989), which is a dual-tasking in which subjects are requested to solve mathematical operations while simultaneously remembering a set of unrelated words. The Ospan score was calculated according to the partial credit unit scoring procedure (PCU; Conway et al., 2005).
Procedure
The ethical review board of the Brugmann Hospital approved the study and written informed consent was obtained from all participants. Participants were tested individually in a quiet room, located at the Medical Psychology Laboratory, Brugmann Hospital. The order of test presentation was counterbalanced. No significant correlations between administration order and performance were present. Participants received €20 for their participation. Controls were asked to avoid alcohol consumption for the prior 24 hours.
Results
Demographics and current clinical status
A description of demographic variables and current clinical status is presented in Table 2. The alcohol and the control were similar in terms of age and years of education. Chi square analyses revealed no differences in the distribution of male and female participants and the distribution of level of education. Depression was higher in alcohol dependents than in controls, t(59) = -6.99, p < 0.001. Compared with controls, state and trait anxiety was higher in the alcohol group, t(59) = -2.40, p < 0.05; t(59) = -3.89, p < 0.001, respectively. The average number of cigarettes smoked per day was higher in alcohol-dependent individuals than in controls, t(59) = -3.43, p < 0.01. Importantly, we observed no significant correlation between current clinical status (depression, state and trait anxiety, cigarettes per day) and performances on decision-making and working memory tasks. Moreover, chi-square and correlation analyses showed that age, sex, level of education (types and years) had no significant impact on performances on decision-making and working memory tasks (all p > .05).
Table 2.
Demographical data and standard deviations for normal controls and alcohol dependents participants.
| Control | Alcohol | Test Statistics | |
|---|---|---|---|
| n | 30 | 30 | |
| Age (SD) | 41.53(10.21) | 44.48(11.69) | t(59) = -1.03, ns |
| Male/Female | 24/6 | 22/8 | X2(1,60) = 0.37, ns |
| Education % (n) | X2(1,60) = 3.38, ns | ||
| Vocational Degree | 6.6(2) | 16.6(5) | |
| High-School Degree | 3.3(1) | 9.9(3) | |
| Bachelor Degree | 70.0(21) | 63.3(19) | |
| Master Degree | 20.0(6) | 10.0(3) | |
| Education (years) | 15.10(2.16) | 14.06(2.63) | t(59) = 1.66, ns |
| Employed full time % (n) | 83.3(25) | 50.0(15) | X2(1,60) = 7.50, p < 0.01 |
| BDI | 2.13(2.49) | 10.50(6.06) | t(59) = -6.99, p < 0.001 |
| STAI-E | 30.20(9.48) | 37.57(13.88) | t(59) = -2.40, p < 0.05 |
| STAI-T | 35.97(7.41) | 45.03(10.32) | t(58) = -3.89, p < 0.001 |
| Cigarettes/Day | 1.74(5.96) | 13.36(16.86) | t(54) = -3.43, p < 0.01 |
| Alcohol drink/Day | 0.94(1.17) | 15.13(4.56) | t(59) = -10.59, p < 0.001 |
| Abstinence (day) | / | 22.07(3.49) | |
| Alcohol dependence duration (year) | / | 19.57(7.17) | |
| Number of times entering an alcohol detoxification program | / | 2.31(1.67) |
Note. Values shown are the mean and standard deviations on each measure. Degrees of freedom differ due to missing data. BDI = Beck Depression Inventory, STAI-E = State version of the State-Trait Anxiety Inventory, STAI-T = Trait version of the State-Trait Anxiety Inventory. Alcohol drink/Day = average number of alcohol drink per day during the past 12 months (aloohol group: 12 months before entering the detoxification program; control group: 12 months before participatig to the study).
Performance on decision-making under ambiguity: Iowa Gambling Task
A repeated measures ANOVA was performed, with group (control vs. alcohol) as a between-subjects factor; block (5 blocks of 20 trials) as a within subjects factor; and the net score of advantageous choice, (C + D), as the dependent measure. This analysis revealed a group effect, group F(1, 59) = 4.64, p < .05, η2 = .07, indicating that the control group performed better than the alcohol group; and a Group × Block interaction, F(4, 56) = 8.88, p < .001, η2 = .13, indicating that task performance increased over time in the control but not in the alcohol group and that controls performed better than alcohol-dependent participants on stage three, four and five of the IGT (see Figure 1).
Figure 1.
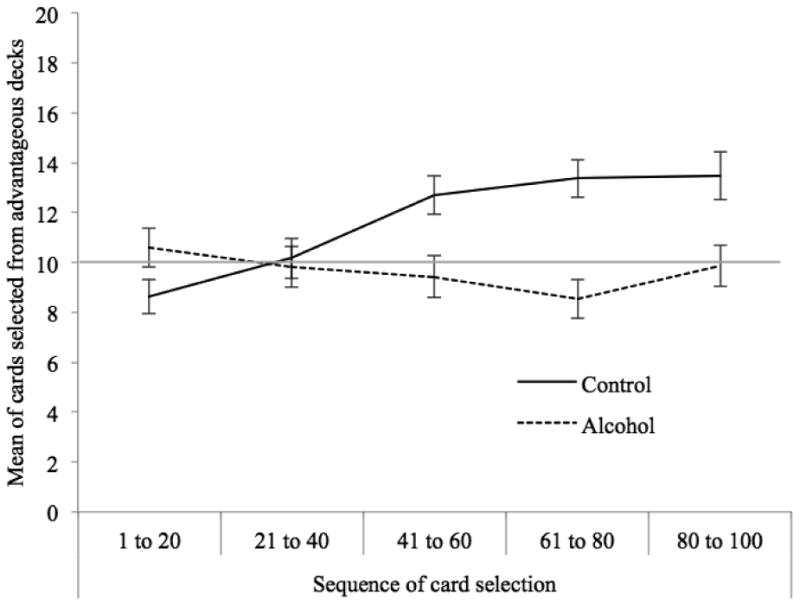
Means of the total number of cards selected from the advantageous decks for each stage of 20 card choices on the Iowa Gambling Task by the control and the alcohol groups, with 10 indicating no preference for advantageous or disadvantageous decks. Error bars are the standard errors of the mean.
Performance on decision-making under risk: Coin Flipping Task (CFP)
A repeated measures ANOVA was performed, with group as the between-subjects factor; ratio of potential win/loss (6 ratio) as the within subjects factor; and the participant's acceptance score, as the dependent measure. Results of the CFP are presented in Figure 2. This analysis revealed an effect of ratio, F(5, 55) = 92.02, p < .001, η2 = .61, indicating that risk acceptance is dependent of ratio of potential win/loss; and a group X win/loss ratio interaction, F(5, 55) = 4.26, p < .01, η2 = .07, indicating that, compared with controls, alcohol dependent participants displayed elevated acceptance to gamble for trials in which potential gain equals the potential loss, and trials in which potential gain was maximum 2 or 2.5 times the amount of the potential loss (see Figure 2).
Figure 2.
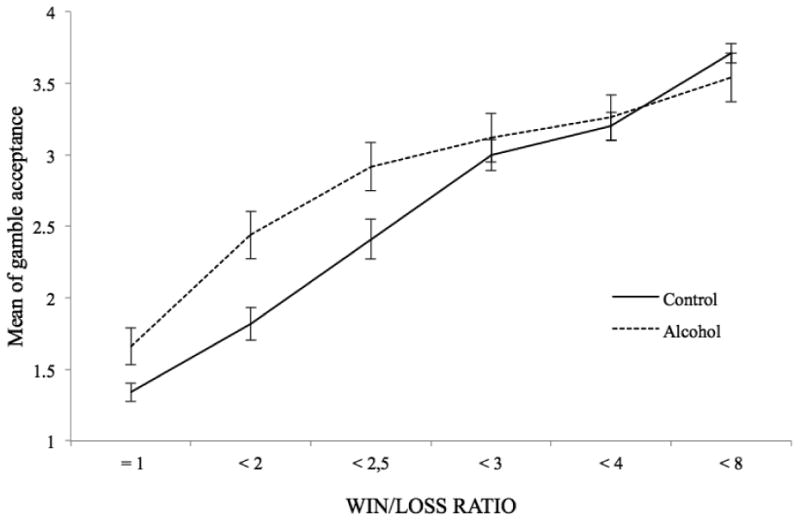
Means of gamble acceptance according to each combination of gains and losses (WIN/LOSS ratio) by controls and alcohol-dependent participants.
Performance on decision-making under risk: Cups task
We conducted a 3 (EV level) X 2 (domain: gain or loss) X 3 (group) repeated measures analyses of variance to compare the groups' risk taking as a function of EV differences between choice options in each domain. Results of the Cups task are presented in Figure 3. We found a main effect of EV, F(2, 58) = 96.68, p < .001, η2 = .63, indicating that risk taking is dependent of EV level; a main effect of Domain, F(2, 58) = 4.69, p = .05, η2 = .08, indicating that risk taking is lower in the loss domain; and a main group effect, F(1, 59) = 4.83, p < .05, η2 = .08, indicating that alcohol-dependent participants displayed elevated risk taking as compared with controls. Additional pairwise comparison revealed that alcohol-dependent took more risk than controls on the risk-equal and risk-disadvantageous conditions of the gain domain only (see Figure 3).
Figure 3.
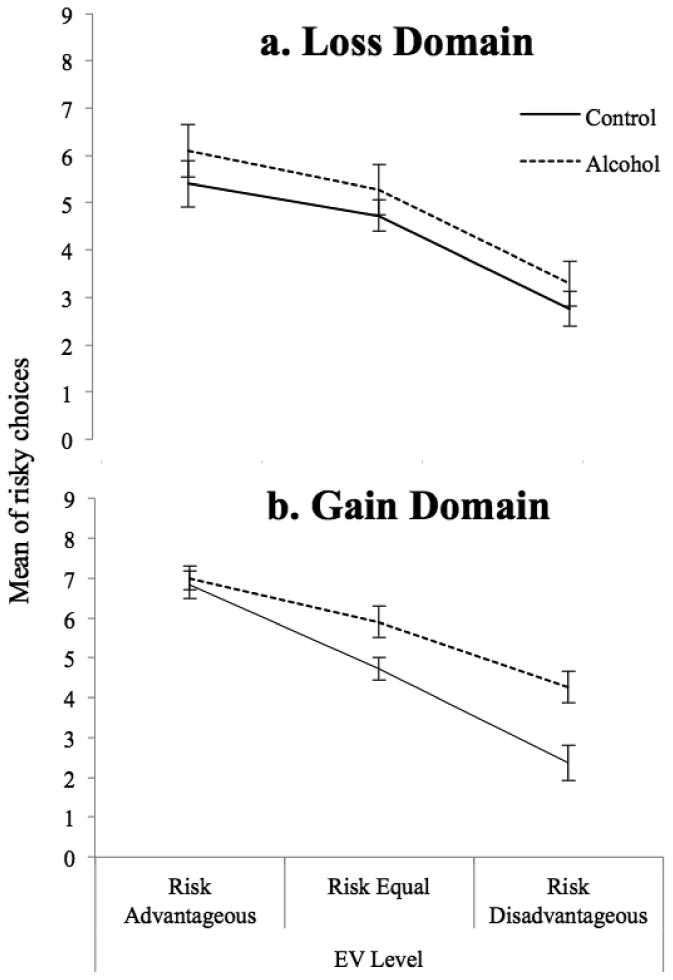
Means of risky choices in (a) the Loss and (b) the Gain domain, as a function of subject group (alcohol; control) and Expected-Value (EV) level (Risk Advantageous trials; Risk Equal expected value trials; Risk Disadvantageous trials). Subjects received nine gain trials and nine loss trials for each of the three EV levels.
Performance on working memory
The alcohol group (M = 11.28; SD = 1.72) did not differ from the control group (M = 10.76; SD = 1.56), in terms of maximum length of numbers serially recalled on the Digit span task (forward), t(57) = -1.20, p > 0.05. On the Ospan task, control participants (M = 0.79; SD = 0.13) obtained significantly higher PCU scores than alcohol-dependent participants (M = 0.55; SD = 0.25), t(59) = 4.70, p < .001. In other words, alcohol-dependent individuals performed were impaired on dual tasking (i.e., Ospan) but not on verbal storage (i.e., Digit span task).
Correlations between decision-making and working memory
We performed correlations between the results of the decision-making tasks and working memory (maximum length of numbers serially recalled on the Digit span task; Ospan PCU scores) to determine whether a relationship existed between working memory functioning and decision-making. Separate correlation analyses were conducted for the alcohol dependence (n = 30) and the control (n = 30) groups. In the control group, performance on the Ospan task was negatively correlated with risky choices during the risk-disadvantageous conditions of the Cups task for the gain domain only, r(30) = -0.41, p < 0.05. We also observed significant correlations between the last two blocks of IGT trials (from trials 61 to 80 and from trials 81 to 100) and performance on the Ospan, r(30) = 0.41, p < 0.05; r(30) = 0.37, p < 0.05, respectively. In the alcohol-dependence group, performance on the Ospan task was negatively correlated with risky choices during the risk-disadvantageous conditions of the Cups task for both the loss and gain domains, r(30) = -0.40, p < 0.05; r(30) = -0.42, p < 0.05, respectively. No other significant correlation was observed.
Discussion
This study was the first to examine the quality of decision-making under varying levels of uncertainty (i.e. ranging from decision-making under ambiguity to decision-making under risk) in alcohol-dependent individuals. The key findings of the present study are as follows: First, compared to healthy controls, alcohol-dependent participants exhibited disadvantageous decision-making under ambiguity, and they choose more risky options that led to negative outcomes during decision-making under risk. Second, alcohol-dependent individuals were impaired on dual tasking as reflected by poor scores on the Ospan task, and these scores correlated with high-risk decision-making.
In the present study, the capacity of decision-making under risk was estimated with the Coin Flipping Task (Tom et al., 2007) and the Cups Task (Levin et al., 2007). We observed that alcohol-dependent individuals took more risky decisions than healthy controls on these two tasks. More specifically, on the CFT, alcohol-dependent participants showed a greater acceptance to gamble than healthy controls under high-risk trials, that is, when the potential gain equals the potential loss and when the gain was maximum 2 or 2.5 times the amount of the potential loss. In a similar way, on the Cups Task, alcohol-dependent individuals took more risk than controls on the risk-equal and risk-disadvantageous conditions of the gain domain, that is, in situations characterized by low or moderate rewards expected value. These results suggest that individuals suffering from an addiction to alcohol are more prone to take risky choice than controls in high-risk situations. Importantly, between-groups differences were found on the gain, but not the loss domain of the Cups task, which suggests that loss sensitivity is not impaired in alcohol-dependent individuals.
In the alcohol-dependence group, risk taking during the risk-disadvantageous conditions of the Cups task (for both the loss and gain domains) was negatively correlated with performance on the Ospan task, for which alcohol-dependent participants were impaired. In other words, alcohol-dependents' impairment in both storing and manipulating information in working memory is associated with high-risk decision-making. These results are in line with previous findings showing that advantageous decision-making under risk is associated with intact executive processes (Brand et al. 2008; Brand et al., 2009; Brevers et al., 2012; Starcke et al., 2011). One possible explanation for this result is that a larger working memory processing capacity may facilitate attention shifting during decision-making from more salient rewards (e.g., option featuring high but uncertain reward during the Cups task), to less salient/risky outcomes (e.g., option featuring low but certain reward during the Cups task) (Finn, 2002; Finn and Hall, 2004; Oberauer, 2002). Indeed, because lower salient information is more difficult to retain in working memory, those with a high working memory capacity could more easily retain both high and lower salient information in mind, while those with low working memory capacity have greater difficulty retaining low salient information (Finn, 2002; Finn et al., 2002; Hinson et al., 2003). Hence, alcohol-dependent individuals may be more prone to taking high-risk choices because of their lowered capacity to manage the interference effects induced by immediate, highly salient information in working memory. Notably, we did not observe a significant relationship between the Ospan and the Coin Flipping Task. One explanation is that the Coin Flipping Task may be less demanding on working memory than the Cups Task. Indeed, the Cups Task involves options featuring both changing win/loss ratios and win/loss probabilities whereas the Coin Flipping Task involves options featuring changing win/loss ratios but a fixed 50/50 probability.
With regard to decision-making under ambiguity, we observed that the alcohol-dependent group choose more often disadvantageous decks than advantageous decks throughout the IGT, that is, they preferred options that bring immediate reward, but then lead to more severe delayed punishment. This result is in line with previous studies showing that recently detoxified alcohol-dependent individuals display an aberrant profile of decision-making on the IGT (e.g. Mazas et al., 2000; Noël et al., 2007). Interestingly, in healthy controls, we observed a correlation between the last two blocks of IGT trials (from trials 60 to 100) and performance on the Ospan. This result seems surprising when referred to the literature advancing that the IGT taps essentially into emotional processes, that is, aspects of decision-making that are predominately influenced by affect and emotion (e.g. Bechara et al., 1994, 1997, 2000). Nevertheless, several recent findings suggest that not all aspects of the IGT are equal at detecting “emotional” decision-making processes. Consistent with this view, performances on working memory (e.g. Brevers et al., 2012) and cognitive flexibility (Brand et al., 2007; Iudicello et al., 2013) have been associated with performance of healthy controls in the latter stages of the IGT. Hence, these results suggest that executive processes may be involved in the latter trials of the IGT. One explanation for these findings is that, across trials, the IGT may vary according to its level of uncertainty (Brand et al., 2006). More specifically, selections during the last block of trials may be referred as decision-making under risk (i.e. situations of decision-making in which probabilities of reward and loss are known) because participants should have experienced the different win/loss contingencies enough to hypothetically know which decks are risky and which are not. By contrast, because there has not been time for a participant to experience any of the win/loss contingencies during early deck choices, the first blocks of the IGT refer to decision-making under ambiguity (i.e. situations of decision-making in which probabilities of reward and loss are unknown). With regard to the alcohol-dependent group, no significant correlation was found between the IGT and the Ospan. These findings suggest that impaired IGT performance in the alcohol-dependent participants is independent from their deficit in working memory. To a broader extent, these results are in line with theoretical accounts, which advance that before elaborate decontextualized problem-solving abilities and other related cognitive skills can begin to be enacted, the ability to control emotional reactions and inhibit basic behavioral impulses is required first (Barkley, 1997; Giancola et al., 2012; Sonuga-Barke et al., 2002). More specifically, alcohol dependence may be underlined by powerful impulsive motivational-habit machinery directed at high, short-term rewards (e.g. disadvantageous decks on the IGT), which could possibly interfere or “hijack” the top-down reflective mechanisms necessary for triggering alarming signals about future outcomes (Noël et al., 2013; Verdejo-Garcia and Bechara, 2009). Put differently, exaggerate impulsive incentive processes directed at high-uncertain rewards would hamper further elaborated decontextualized problem-solving abilities. Further studies are needed in order to confirm that impaired executive processes do not impact IGT performance in alcohol-dependent individuals. One option would be to increase the number of IGT trials (e.g. from 100 to 120) and to examine the association between these later trials and several measures of executive function, including working memory, and planning and cognitive flexibility. Additional studies are also needed in order to better estimate the impact of impulsive incentive process on top-down reflective processes. One direction for future studies would be to measure autonomic arousal during functional magnetic resonance imaging (fMRI) scanning (for a review on how integrating fMRI with psychophysiological measurements during the IGT, see Wong et al., 2011), which would complement behavioral findings in providing a more comprehensive understanding on the physiological and neural mechanisms underlying impaired decision-making in alcohol dependence.
In summary, recently detoxified alcohol-dependent individuals were impaired in making their decisions under risk and under ambiguity, with an impaired executive component of working memory associated only with high-risk decision-making. This study extends our knowledge about impairments of decision-making under uncertainty in alcohol-dependence.
Acknowledgments
Dr Damien Brevers is a Post-Doctoral Research Scholar supported by the National Institute of NIDA R01 DA16708 (A.B.). Dr Xavier Noël is Research Associate of the Belgian Scientific Fund of Research (F.R.S./FNRS).
Contributor Information
Damien Brevers, Email: dbrevers@ulb.ac.be, brevers@usc.edu.
Antoine Bechara, Email: bechara@usc.edu.
Axel Cleeremans, Email: axcleer@ulb.ac.be.
Charles Kornreich, Email: charles.kornreich@chu-brugmann.be.
Paul Verbanck, Email: paul.verbanck@chu-brugmann.be.
Xavier Noël, Email: xnoel@ulb.ac.be.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th. American Psychiatric Publishing; Arlington: 2013. [Google Scholar]
- Baddeley A, Della Sala S. Working memory and executive control. Philos Trans R Soc Lond. 1996;351:1397–1404. doi: 10.1098/rstb.1996.0123. [DOI] [PubMed] [Google Scholar]
- Barkley R. Attention deficit/hyperactivity disorder, self-regulation, and time: Towards a more comprehensive theory. J Develop Behav Pediatrics. 1997;18:271–279. [PubMed] [Google Scholar]
- Bechara A, Damasio AR, Damasio H. Emotion, decision making and the orbitofrontal cortex. Cereb Cortex. 2000;10:295–307. doi: 10.1093/cercor/10.3.295. [DOI] [PubMed] [Google Scholar]
- Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. 1994;50:7–15. doi: 10.1016/0010-0277(94)90018-3. [DOI] [PubMed] [Google Scholar]
- Bechara A, Damasio H, Tranel D, Damasio AR. Deciding advantageously before knowing the advantageous strategy. Science. 1997;275:1293–1294. doi: 10.1126/science.275.5304.1293. [DOI] [PubMed] [Google Scholar]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- Blume AW, Schmaling KB, Marlatt GA. Memory, executive cognitive function, and readiness to change drinking behavior. Addict Behav. 2005;30:301–314. doi: 10.1016/j.addbeh.2004.05.019. [DOI] [PubMed] [Google Scholar]
- Bowden-Jones H, McPhillips M, Rogers R, Hutton S, Joyce E. Risk-taking on tests sensitive to ventromedial prefrontal cortex dysfunction predicts early relapse in alcohol dependency: a pilot study. J Neuropsychiatry Clin Neurosci. 2005;17:417–420. doi: 10.1176/jnp.17.3.417. [DOI] [PubMed] [Google Scholar]
- Brand M. Does the feedback from previous trials influence current decisions? A study on the role of feedback processing in making decisions under explicit risk conditions. J Neuropsychol. 2008;2:431–443. doi: 10.1348/174866407x220607. [DOI] [PubMed] [Google Scholar]
- Brand M, Labudda K, Markowitsch HJ. Neuropsychological correlates of decision-making in ambiguous and risky situations. Neural Networks. 2006;19:1266–1276. doi: 10.1016/j.neunet.2006.03.001. [DOI] [PubMed] [Google Scholar]
- Brand M, Recknor EC, Grabenhorst F, Bechara A. Decisions under ambiguity and decisions under risk: correlations with executive functions and comparisons of two different gambling tasks with implicit and explicit rules. J Clin Exp Neuropsychol. 2007;29:86–99. doi: 10.1080/13803390500507196. [DOI] [PubMed] [Google Scholar]
- Brand M, Laier C, Pawlikowski M, Markowitsch HJ. Decision-making with and without feedback: the role of intelligence, strategies, and cognitive styles. J Clin Exp Neuropsychol. 2009;31:967–981. doi: 10.1080/13803390902776860. [DOI] [PubMed] [Google Scholar]
- Brevers D, Cleeremans A, Goudriaan AE, Bechara A, Kornreich C, Verbanck P, Noël X. Decision making under ambiguity but not under risk is related to problem gambling severity. Psychiatry Res. 2012;200:568–574. doi: 10.1016/j.psychres.2012.03.053. [DOI] [PubMed] [Google Scholar]
- Conway AR, Kane MJ, Bunting MF, Hambrick DZ, Wilhelm O, Engle RW. Working memory span tasks: A methodological review and user's guide. Psychon Bull Rev. 2005;12:769–786. doi: 10.3758/bf03196772. [DOI] [PubMed] [Google Scholar]
- Dao-Castellana MH, Samson Y, Legault F, Martinot JL, Aubin HJ, Crouzel C, Feldman L, Barrucand D, Rancurel G, Feline A, Syrota A. Frontal dysfunction in neurologically normal chronic alcoholic subjects: metabolic and neuropsychological findings. Psychol Med. 1998;28:1039–1048. doi: 10.1017/s0033291798006849. 1998. [DOI] [PubMed] [Google Scholar]
- Dunn BD, Dalgleish T, Lawrence AD. The somatic marker hypothesis: A critical evaluation. Neurosci Biobehav Rev. 2006;30:239–271. doi: 10.1016/j.neubiorev.2005.07.001. [DOI] [PubMed] [Google Scholar]
- Fein G, Klein L, Finn P. Impairment on a simulated gambling task in long-term abstinent alcoholics. Alcohol Clin Exp Res. 2004;28:1487–91. doi: 10.1097/01.alc.0000141642.39065.9b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finn PR. Motivation, working memory, and decision making: A cognitive-motivational theory of personality vulnerability to alcoholism. Behav Cogn Neurosci Rev. 2002;1:183–205. doi: 10.1177/1534582302001003001. [DOI] [PubMed] [Google Scholar]
- Finn PR, Hall J. Cognitive ability and risk for alcoholism: short-term memory capacity and intelligence moderate personality risk for alcohol problems. J Abnorm Psychol. 2004;113:569–581. doi: 10.1037/0021-843X.113.4.569. [DOI] [PubMed] [Google Scholar]
- Finn PR, Mazas C, Justus A, Steinmetz JE. Early-onset alcoholism with conduct disorder: Go/No-Go learning deficits, working memory capacity, and personality. Alcohol Clin Exp Res. 2002;26:186–206. [PubMed] [Google Scholar]
- Finn PR, Rickert ME, Miller MA, Lucas J, Bogg T, Bobova L, Cantrell H. Reduced Cognitive Ability in Alcohol Dependence: Examining the Role of Covarying Externalizing Psychopathology. J Abnorm Psychol. 2009;118:100–116. doi: 10.1037/a0014656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- First MB, Spitzer RL, Gibbon M, Williams JW. Structured Clinical Interview for DSM–IV–TR Axis I Disorders, Research Version, Non-patient Edition (SCID-I/NP) Biometrics Research New York State Psychiatric Institute; New York: 2002. [Google Scholar]
- Giancola PR, Godlaski AJ, Roth RM. Identifying Component-Processes of Executive Functioning that Serve as Risk Factors for the Alcohol-Aggression Relation. Psychol Addict Behav. 2012;26:201–211. doi: 10.1037/a0025207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heishman SJ. What aspects of human performance are truly enhanced by nicotine? Addiction. 1998;93:317–320. doi: 10.1080/09652149835864. [DOI] [PubMed] [Google Scholar]
- Hinson JM, Jameson TL, Whitney P. Impulsive decision making and working memory. J Exp Psychol Learn Mem Cogn. 2003;29:298–306. doi: 10.1037/0278-7393.29.2.298. [DOI] [PubMed] [Google Scholar]
- Iudicello JE, Woods SP, Cattie JE, Doyle K, Grant I. Risky decision-making in HIV-associated neurocognitive disorders (HAND) Clin Neuropsychol. 2013;27:256–275. doi: 10.1080/13854046.2012.740077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kahneman D, Tversky A. Prospect Theory: An Analysis of Decision under Risk. Econometrica. 1979;47:263–292. [Google Scholar]
- Kerr A, Zelazo PD. Development of “hot” executive function: the children's gambling task. Brain Cogn. 2004;55:148–157. doi: 10.1016/S0278-2626(03)00275-6. [DOI] [PubMed] [Google Scholar]
- Kornreich C, Brevers D, Ermer E, Hanak C, Verbanck P, Campanella S, Noël X. Polysubstance dependent patients display a more utilitarian profile in moral decision-making than alcohol-dependent patients, depressive patients and controls. Drug Alcohol Depend. 2013;132:434–440. doi: 10.1016/j.drugalcdep.2013.03.005. [DOI] [PubMed] [Google Scholar]
- Krain AL, Wilson AM, Arbuckle R, Castellanos FX, Milham MP. Distinct neural mechanisms of risk and ambiguity: a meta-analysis of decision making. NeuroImage. 2006;32:477–484. doi: 10.1016/j.neuroimage.2006.02.047. [DOI] [PubMed] [Google Scholar]
- Levin I, Weller J, Pederson A, Harshman L. Age-related differences in adaptive decision-making: sensitivity to expected value in risky choice. Judgment Decision Making. 2007;2:225–233. [Google Scholar]
- Mazas CA, Finn PR, Steinmetz JE. Decision making biases, antisocial personality, and early-onset alcoholism. Alcohol Clin Exp Res. 2000;24:1036–40. [PubMed] [Google Scholar]
- Noël X, Bechara A, Brevers D, Verbanck P, Campanella S. Alcoholism and the Loss of Willpower: A Neurocognitive Perspective. J Psychophysiol. 2010;24:240–248. doi: 10.1027/0269-8803/a000037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Noël X, Brevers D, Bechara A. A neurocognitive approach to understanding the neurobiology of addiction. Curr Opin Neurobiol. 2013;23:632–638. doi: 10.1016/j.conb.2013.01.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Noël X, Bechara A, Dan B, Hanak C, Verbanck P. Response inhibition deficit is involved in poor decision making under risk in nonamnesic individuals with alcoholism. Neuropsychol. 2007;21:778–786. doi: 10.1037/0894-4105.21.6.778. [DOI] [PubMed] [Google Scholar]
- Noël X, Van der Linden M, Schmidt N, Sferrazza R, Hanak C, Le Bon O, De Mol J, Pelc I, Verbanck P. Supervisory attentional system in nonamnesic alcoholic men. Arch Gen Psychiatry. 2001;58:1152–1158. doi: 10.1001/archpsyc.58.12.1152. [DOI] [PubMed] [Google Scholar]
- Oberauer K. Access to information in working memory: Exploring the focus of attention. J Exp Psychol: Learn Mem Cogn. 2002;28:411–421. [PubMed] [Google Scholar]
- Rogers RD, Owen AM, Middleton HC, Williams EJ, Pickard JD, Sahakian BJ, Robbins TW. Choosing between small, likely rewards and large, unlikely rewards activates inferior and orbital prefrontal cortex. J Neurosci. 1999;19:9029–9038. doi: 10.1523/JNEUROSCI.19-20-09029.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sonuga-Barke E, Dalen L, Daley D, Remington B. Are planning, working memory, and inhibition associated with individual differences in preschool ADHD symptoms? Develop Neuropsychol. 2002;21:255–272. doi: 10.1207/S15326942DN2103_3. [DOI] [PubMed] [Google Scholar]
- Spielberger C. Manual for the State-Trait Anxiety Inventory: STAI (Eorm I) Consulting Psychologists Press; Palo Alto, CA: 1983. [Google Scholar]
- Starcke K, Pawlikowski M, Wolf OT, Altstötter-Gleich C, Brand M. Decision-making under risk conditions is susceptible to interference by a secondary executive task. Cognitive Processing. 2011;12:177–182. doi: 10.1007/s10339-010-0387-3. [DOI] [PubMed] [Google Scholar]
- Tom SM, Fox CR, Trepel C, Poldrack RA. The neural basis of loss aversion in decision-making under risk. Science. 2007;315:515–518. doi: 10.1126/science.1134239. [DOI] [PubMed] [Google Scholar]
- Turnbull OH, Evans CE, Bunce A, Carzolio B, O'Connor J. Emotion based learning and central executive resources: an investigation of intuition and the Iowa gambling task. Brain Cogn. 2005;57:244–247. doi: 10.1016/j.bandc.2004.08.053. [DOI] [PubMed] [Google Scholar]
- Turner ML, Engle RW. Is working memory capacity task dependent? J Mem Lang. 1989;28:127–154. [Google Scholar]
- Verdejo-Garcia A, Bechara A. A somatic marker theory of addiction. Neuropharmacol. 2009;56:48–62. doi: 10.1016/j.neuropharm.2008.07.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong SW, Xue G, Bechara A. Integrating fMRI with psychophysiological measurements in the study of decision-making. J Neurosci Psychol Economics. 2011;4:85–94. doi: 10.1037/a0023525. [DOI] [PMC free article] [PubMed] [Google Scholar]