

Abstract
First Responders (FR) present at Ground Zero within the first 72-hr after the WTC (World Trade Center) collapse have progressively exhibited significant respiratory injury. The majority (>96%) of WTC dusts were >10 μm and no studies have examined potential health effects of this size fraction. This study sought to develop a system to generate and deliver supercoarse (10–53 μm) WTC particles to a rat model in a manner that mimicked FR exposure scenarios. A modified Fishing Line generator was integrated onto an intratracheal inhalation (ITIH) system that allowed for a bypassing of the nasal passages so as to mimic FR exposures. Dust concentrations were measured gravimetrically; particle size distribution was measured via elutriation. Results indicate that the system could produce dusts with 23 μm MMAD at levels up to ≥ 1200 mg/m3. To validate system utility, F344 rats were exposed for 2-hr to ≈100 mg WTC dust/m3. Exposed rats had significantly increased lung weight and levels of select tracer metals 1-hr post-exposure. Using this system, it is now possible to conduct relevant inhalation exposures to determine adverse WTC dusts impacts on the respiratory system. Furthermore, this novel integrated Fishing Line-ITIH system could potentially be used in the analyses of a wide spectrum of other dusts/pollutants of sizes previously untested or delivered to the lungs in ways that did not reflect realistic exposure scenarios.
Keywords: World Trade Center, WTC, dust, Fishing Line, Generator, Intratracheal Inhalation
Introduction
The World Trade Center (WTC) collapse on September 11, 2001 (hereafter termed 9/11) claimed thousands of victims. The event not only resulted in an immediate devastating loss of life, but has given rise to health effects that have taken years to manifest. The collapse itself was an unprecedented environmental disaster that resulted in the discharge of an expansive dust-laden plume containing thousands of tons of pulverized masonry, glass, and building debris that eventually deposited over the greater New York area (Lioy, et al., 2002; McGee, et al., 2003). Though there were no explicit measures of air quality immediately after the collapse, extrapolations from airborne PM levels allowed for estimates to be generated, ranging from >5000 μg/m3 at Ground Zero in the first hours after the collapse to < 1600 μg/m3 thereafter, with intermittent spikes and declines dependent on site activity (Landrigan, et al., 2004; Lorber, Gibb, Grant, Pinto, Pleil and Cleverly, 2007). Thus, a huge number of people were potentially exposed to perilous aerosolized WTC dusts, particularly on-scene First Responder (FR) emergency personnel (e.g., firefighters, police, rescue personnel, construction\utility workers), and civilians involved in clean-up/rescue efforts in the days (as well as weeks and months) after 9/11.
WTC dust exposure was routinely high among the populations that were present at the time of the collapse and those who remained at Ground Zero for sustained periods during the first 72-hr afterward. Accordingly, of the many populations likely to have inhaled WTC dusts on 9/11 or the first days thereafter, it would seem that FR would have been most at risk to manifest adverse health effects (Banauch, et al., 2005; Edelman, et al., 2003; Herbert, et al., 2006; Landrigan, et al., 2004; Lioy, et al., 2002; Prevention), 2002; Webber, et al., 2009). Among one set of FR, the Fire Department of New York (FDNY), 16% were present at the time of the collapse and 69% arrived during the next 48-hr (Feldman, et al., 2004); the WTC dust exposure status of ≈85% of these (and other FR) was declared moderate-to-high ((CDC), 2004; Banauch, et al., 2003; Prezant, et al., 2002). Furthermore, a majority of firefighters at the Main Pile 9/11–9/13 rarely/never wore respiratory protection; Prezant et al. (2002) first reported 76–93% non-usage rates while Feldman et al. (2004) later cited lower (but still worrisome) rates of 35–74%. A similar survey of non-firefighter volunteers indicated that only ≈20% (in cohort of 1150) had access to/used respirators in the period from 9/11–9/13((CDC), 2004; Antao, et al., 2011; Wheeler, et al., 2007). Consequently, FR and others may have been exposed for up to 12–16 hr/d to unprecedented concentrations of fine, coarse, and supercoarse WTC particles without adequate protection. Compounding this with the continuous re-suspension of settled dusts and increased mouth breathing as a result of physical activity on the pile further increased the risk that WTC dust particles - particularly those with large aerodynamic diameters (i.e., >2.5 μm; coarse and/or supercoarse) - could have been entrained in the lungs of the FR. Consequently, over the past decade, studies have reported findings indicative of upper and lower respiratory diseases/dysfunction in a large percentage of exposed FR (Banauch, et al., 2005; Buyantseva, et al., 2007; de la Hoz, et al., 2008; Herbert, et al., 2006; Mendelson, Roggeveen, Levin, Herbert and de la Hoz, 2007; Oppenheimer, et al., 2007; Prezant, 2008; Rom, et al., 2010; Salzman, Moosavy, Miskoff, Friedmann, Fried and Rosen, 2004; Szeinuk, Padilla and de la Hoz, 2008; Wheeler, et al., 2007). Moreover, significant associations have been (and even still continue to be) established between arrival time at Ground Zero and reductions in pulmonary function, increased incidence/severity of persistent airway hyperactivity/asthma, sarcoid-like granulomatous pulmonary disease (SLGPD), and most recently, cancer (albeit not in the lungs specifically) ((CDC), 2004; Izbicki, et al., 2007; Kim, et al., 2012; Nolan, et al., 2011; Prevention), 2002; Prezant, et al., 2002; Skloot, et al., 2004; Weakley, et al., 2011; Weiden, et al., 2010; Zeig-Owens, et al., 2011).
To discern the etiology of pulmonary health effects associated with exposure to these WTC dusts, it is critical to first understand their fundamental properties. The dispersed WTC dust was a heterogeneous mix of varying sizes, shapes, densities, and composition derived from an amalgamation of sources from/within the buildings. In regard to size, 1.5% of the dusts (by mass) collected at or around Ground Zero from 9/11–9/13 had an aerodynamic diameter of ≤ 2.5 μm (fine), ≈ 0.5% had 2.5–10 μm diameters (coarse), and the majority (>96%) had a diameter ≥ 10 μm (supercoarse; with 58% of this fraction being >53 μm) (Lioy, et al., 2002; Offenberg, et al., 2003). In regard to composition, several contaminants in the WTC dusts believed to pose adverse health effects were identified by the US Environmental Protection Agency (US EPA) and other researchers, i.e., metals (e.g., nickel, chromium, lead), polychlorinated biphenyls, dioxins, asbestos, volatile organic compounds (VOC), polycyclic aromatic hydrocarbons (PAHs), and synthetic vitreous fibers (SVF) ((USGS), Clark, Plumlee, Meeker and Swayze, 2002; Gavett, 2003; Lioy, et al., 2002; Lowers, Meeker, Lioy and Lippmann, 2009; McGee, et al., 2003; Offenberg, et al., 2003; Olson, Norris, Landis and Vette, 2004; United States Environmental Protection Agency (US EPA), 2002; United States Environmental Protection Agency (US EPA), 2003).
Despite the fact that the majority of the WTC dusts were comprised of particles with >10 μm diameters, the few in vivo studies performed thus far to evaluate health effects used only the fine fraction (Gavett, 2003). Consequently, these attempts to broadly assess WTC dust-related health effects were severely limited in scope, as they did not consider effects from exposures to the larger particles in the dusts. Admittedly, larger particles are generally dismissed in regard to inhalation risk and exposure assessment as they are often deemed `toxicologically irrelevant' due to their inherent particle dynamics (i.e. substantial settling velocity, limited suspension in an aerosol, and poor airway infiltration efficiency) as well as innate physiological mechanisms that promote filtration of larger particles (nasal turbidity, mucosal membranes, etc.).
Nonetheless, we would contend that the inclusion of larger diameter particles is essential to accurately assess the health effects of particles that were likely entrained at Ground Zero. This is because: (A) High airborne particle densities (i.e., ~96% of particles >10 μm) were present at Ground Zero in the initial days after the collapse; (B) the chemistries of the dusts, including pH, were size-related (i.e., particles >10 μm were highly alkaline) (Landrigan, et al., 2004; Lioy, et al., 2002) – a fact that could contribute to impairment of many inherent protective mechanisms in the respiratory tract (Clary-Meinesz, Mouroux, Cosson, Huitorel and Blaive, 1998; Gaafar, Girgis, Hussein and el-Nemr, 1992; Holma, Lindegren and Andersen, 1977; Toren, Brisman, Hagberg and Karlsson, 1996); (C) continuous re-suspension of debris/particulate matter as a result of pile activity (i.e. construction equipment, vehicle/foot traffic, etc.) (Landrigan, et al., 2004); (D) a general lack of/non-use of respirators for long periods likely resulted in workers being exposed to very high doses of dusts (Feldman, et al., 2004; Prezant, et al., 2002); and, (E) heavy mouth breathing during labor at Ground Zero would have resulted in significant bypass of nasal filtering and increased risk of larger particle entrainment into the trachea/airways. Thus, a lack of consideration of the effects from supercoarse particles appears to have been an unintentional but critical oversight in earlier studies; this implies that we still lack an accurate portrait of the wide spectrum of effects from the particles that were actually present in the air at Ground Zero.
Accordingly, the goal of this study was to accurately simulate Ground Zero exposure conditions in regard to particle size distributions as well as mode of exposure. Specifically, a system was designed to deliver coarse and supercoarse fractions of `parent' (hereafter defined as unfractionated, apart from initial sieving to remove supersize debris, >53 μm) WTC dusts to an animal model at representative concentrations and in a scenario that would mimic FR mouth breathing; a secondary goal was to do this exposure in an efficient manner that maximized preservation of precious WTC dust stocks. Ultimately, the WTC dusts atmospheres were generated via a Fishing Line system that was based on an original design by Ledbetter et al. in 1998 (Ledbetter, Killough and Hudson, 1998). The generation device was, in turn, interfaced with an intratracheal inhalation (ITIH) system designed by Oberdörster and colleagues (Hesterberg, et al., 1996; Oberdorster, Cox and Gelein, 1997) so that in situ responses to coarse/supercoarse dust particles could ultimately be assessed.
Materials and Methods
WTC Dusts
WTC dusts were collected at representative sites on/around the Main Pile at Ground Zero during September 12–13, 2001 after the collapse of WTC Buildings 1–7 (as described by Maciejczyk and colleagues (Maciejczyk Polina, Zeisler Rolf, Hwang, Thurston George and Chen Lung, 2005). All samples were stored in airtight containers in the dark at room temperature in order to minimize any potential light, heat, or ambient gas-induced changes in original physicochemical properties. Because large debris (e.g., glass\metal shards, stones, carpet fragments) that would never be drawn into the lungs was also present in the collected samples, parent WTC dusts per se could not be used. The collected dusts were sieved to yield all particles of diameters ≤ 53 μm (i.e., WTC53-) for use in the Fishing Line generator + ITIH exposure system. Details about preparation of first-sieve (i.e., WTC53-) materials, as well as on the inherent chemical and physical properties of each of the various size fractions isolated from the original dusts have been previously reported (Gavett, 2003; Lioy, et al., 2002; McGee, et al., 2003).
WTC Dust Atmosphere Generator
WTC dust atmospheres were generated via a custom-built Fishing Line system based on an original design developed by Ledbetter and colleagues at the USEPA to generate nanoparticle atmospheres in inhalation studies (Ledbetter, Killough and Hudson, 1998). The modified design here (Figure 1) was developed to efficiently utilize `intact' WTC53- particles to generate a representative WTC dust atmosphere. The general principle of this system was one wherein a cotton string was pulled through a particle-filled reservoir to allow particles to loosely adhering to it. The string then passed into a `discharge head' where filtered air blew the particles off and into a mixing chamber that served as the exposure interface.
Figure 1.

String Generator Setup modified from Ledbetter et al. [(Ledbetter, Killough and Hudson, 1998)]).
A fixed amount (≈ 7 g) of WTC dust (WTC53-) was loaded into a 1/4” OD (outer diameter) Tygon tube reservoir (length = 4.20 in; inner diameter = 0.375 in). The base of the reservoir was fitted with a custom made 0.38” OD stainless steel cylinder, internally threaded to secure an embedded rubber septum needed to allow only the string (100% Mercerized Cotton, Size 10, DMC Corporation, Kearny, NJ) to freely pass and reduce fugitive dust from escaping the reservoir. String for the generator was stored on fishing reels (Penn Model 109 M; Penn Fishing Tackle Mfg., Philadelphia, PA); during generation, the string progressed from a supply reel, through the reservoir, and toward a take-up reel. The speed at which string passed through the reservoir was controlled via a variable speed motor (DC gear motor, dedicated speed control, NEMA, Austin, TX). To agitate the dust in the reservoir (to prevent settling/allow for maximal opportunity to adhere to passing string), the reservoir was continuously compressed/relaxed by pneumatic hammers at frequent intervals; frequency was increased depending on string speed (i.e., 4 sec off/0.1 sec on) using a time-delayed, repeat-cycle relay.
All dilution air required for dust generation was composed of a mixture of filtered air and Isoflurane (ISO; IsoFlo, Abbott Laboratories, North Chicago, IL) in O2 carrier gas (2.5% final concentration after mixing with air). Temperature and relative humidity of the dilution air was continuously measured to avoid conditions that could promote particle agglomeration. All air was passed through a denuder assembly (consisting of Purafil for NOx and O3, citric acid-coated annular glass denuders for NH3, and activated charcoal for further removal of reactive gases) prior to combination with the ISO or dust. Total flow rates of ≈ 10 LPM (using and air/ISO carrier) were used for all particle generations.
All generated dust atmospheres were assessed gravimetrically using Teflon filters (47 mm, 0.2 μm pore Type FG; Millipore, Bedford, MA). All filters were weighed on a Mettler-Toledo microbalance (1 μg sensitivity; Model MT5, Hightown, NJ) in an environmentally controlled facility (maintained at 20–23°C and 38–42% relative humidity) before and after sampling. All samples were obtained by flow-pass collection for fixed periods of time during dust generation. As there was no commercial instrument able to determine size distributions of the WTC dust atmospheres (due to supercoarse content), an elutriator was built to measure distribution.
Mode of Exposure
All rats here were exposed to WTC53- dusts via intratracheal inhalation (ITIH) in an integrated system originally designed by Oberdörster et al. at the University of Rochester School of Medicine (Elder, et al., 2005; Hesterberg, et al., 1996; Oberdorster, Cox and Gelein, 1997; Osier and Oberdorster, 1997). This system allows for particles, including those with da >2.5 μm, to circumvent the rat nasal region so that the particles are introduced into (and deposited within) the lungs in a manner most representative of FR exposure to particles via mouth breathing.
For the studies, male F344 rats (8-wk-old) were purchased from Harlan Labs (Frederick, MD). On arrival, the rats were placed in polycarbonate cages with corncob bedding in a facility maintained at 23°C with a 30–50% relative humidity and 12-hr interval light/dark cycle, and allowed to acclimate for 1 wk prior to use. All rats had ad libitum access to Purina Lab Chow and filtered water. All animal procedures were conducted under an animal protocol approved by New York University Institutional Animal Care and Use Committee (IACUC).
To perform an ITIH exposure, each rat was anaesthetized in a dedicated knockout box using 5% ISO (for 5 min) generated by an EZ-150C system (EZ Systems Corp., Palmer, PA). The rat then had its trachea cannulated with an 18-G Insyte catheter (Becton Dickinson, Sandy, UT) fitted with a plastic collar (from 200 μl pipette tip; ICN Biomedicals, Solon, OH); the collar assured that particles did not escape up the trachea during exposure. The open end of the catheter was then attached to a port on the ITIH system (Figure 2) and mechanical ventilation thereafter sustained at 60 breaths/min (0.5 sec inhale:0.5 sec exhale) using a timer-activated solenoid valve. Dust/air/ISO (now 2.0–2.5% due to dilution) mixture was then delivered at a maximum pressure of 15–20 cm H2O (average 17.5; regulated via water column\monitored via Magnehelic differential-pressure-gauge); excess air was vented off the system via a water column. To maintain body temperature (continuously monitored via rectal probe; Physitemp Instruments, Clifton, NJ), each rat was kept on a covered heating pad for the duration of exposure. Blood O2 levels were also checked during exposure using a Pulse Oximeter (Nonin Medical Inc., Minneapolis, MN).
Figure 2.
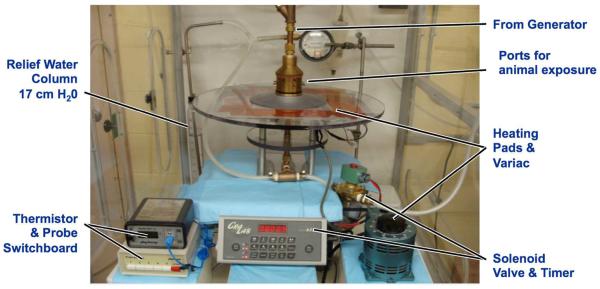
ITIH Setup (modified from Oberdörster et al. [Hesterberg, et al., 1996; Oberdorster, Cox and Gelein, 1997)]).
Confirmation of WTC dust delivery
To verify the system ability to deposit WTC particles in the lungs, a separate study was done in which rats were exposed once (for 81 min) to WTC53- dusts (WTC treatment group, n = 6), ISO only (2.5% in carrier O2 gas, ISO group, n = 3), or nothing (Naïve group, n = 3). For this study, an atmosphere of ≈ 100 mg WTC dust/m3 was used. This dose was chosen as a conservative estimate to model a rat exposure corresponding to one likely to have occurred in a representative mouth-breathing FR exposed to ≈ 750 mg WTC dust/m3 at Ground Zero during the 9/11–13/01 period (Geyh, et al., 2005).
Within 1 hr after the exposure, each rat (dust, ISO, or naïve) was sacrificed via intraperitoneal injection with Sleepaway® (≈ 500 mg/kg; Fort Dodge Animal Health, Fort Dodge, IA) and exsanguination. The trachea (from collar-point down) and lungs were removed en bloc, blot dried and weighed. All samples were then frozen and held at −80°C until analyzed. Procedures used in our NIEHS Center Analytical Core were applied to determine lung levels of aluminum (Al), antimony (Sb), and titanium (Ti); these metals were selected as potential markers of WTC dust exposure in that unlike other metals that might be found in the lungs, they could be attributable only to WTC dust (Maciejczyk Polina, Zeisler Rolf, Hwang, Thurston George and Chen Lung, 2005; McGee, et al., 2003). Briefly, each sample was placed in a Teflon beaker with 2.5 ml of a hydrochloric/hydrofluoric acid (HCl:HF, 7:3 [v/v]) mixture. One ml ultrapure HNO3 was then added and the sample heated at 95°C for 2 hr. After cooling, 1.08 ml boric acid solution was added (for quenching) and the sample then analyzed via ICPOES (inductively coupled plasma optical emission spectrometry; Model Optima 4300D, Perkin Elmer, Norwalk, CT). Instrument sensitivity was ≈ 1 ppt for Al and Sb and 0.1 ppt for Ti. All reagents used were reagent grade and acids were Fisher Optima Grade; materials used to generate standard curves (5-point calibration along with standard blank to assure accurate baseline) for analyses were NIST traceable. All dilutions (reagents and standards) were made up fresh in 18 MΩ H2O. To assure no metal contamination occurred, all glassware was washed in microsoap solution, rinsed in 18 MΩ H2O, soaked in 20% HNO3 overnight, and then rinsed in 18 MΩ H2O.
From the ICPOES values, the amount of WTC dust that was delivered/deposited in the lungs during the exposure was calculated. Values for total amounts of Ti, Al, and Sb in the lungs were each divided by their corresponding relative amounts in samples of `intact' dust that were analyzed in parallel. From this calculation (i.e., X μg Al/[Y μg Al/mg WTC dust]), the total amount of dust (i.e., mg dust, in each case as a function of individual metal) was calculable.
Statistics
All data in the “Confirmation of WTC dust delivery” study were analyzed by one-way analysis of variance (ANOVA) with exposure group (naïve, ISO only, or WTC dust/ISO) as the main factor. Prior to performing ANOVA, all data was tested to assure assumptions of normality and homogeneity of variance were met. Dixon and Grubbs analyses were used to screen for outliers (Taylor, 1990). Statistical significance in all cases was considered at p < 0.05. All analyses were performed using Prism software (V5.0, GraphPad Soft-ware Inc., San Diego, CA).
Results
WTC dust size characteristics
Sieving of WTC parent dusts revealed that the majority of the dust mass was composed of coarse and supercoarse particles – corroborating previously published findings (Lioy et al., 2002). Specifically, size distribution analyses showed that >95% of the dust mass collected at/near Ground Zero was of an aerodynamic diameter ≥10 μm, with the majority (56%) being >53 μm (>WTC53); particles with 10–53 μm (WTC10–53), 2.5–10 μm (WTC2.5–10), or ≤ 2.5 μm (WTC2.5) diameters comprised 42, 0.5, and 1.5% of the total mass, respectively.
The mass median aerodynamic diameter (MMAD) of the < 53 μm WTC dust for this study was confirmed via horizontal elutriation to be 23 μm (σg = 1.45). The elutriator consisted of a rectangular box constructed entirely of inert/nonconductive material (layered corrugated cardboard) (internal length, 1.2 m; width, 7.6 cm; height, 6.4 cm). The device housed 17 filter holders in a uniform plane flush along its base, each accommodating a single quartz filter that would capture particles settling from a uniform ≈13 LPM stream of dust and whose masses would then be assessed gravimetrically in the environmentally controlled microbalance room. These materials were used in all system validations, characterizations, and confirmation exposure experiments.
Generation of WTC particles
WTC dust atmospheres were generated using a modified Fishing Line system. Modifications were specifically made to suit the use of larger (supercoarse) particle sizes and longer-term animal model exposures. Of the various parameters tested during system construction (including orientation of Tygon dust reservoir, string speed, discharge air flow), string speed was found to be the most critical variable. As shown in Figure 3, string speed was positively and linearly correlated to increased dust delivery and airborne concentrations. Values ranged from an average of 3.2 mg dust delivered (equates to ≈ 33 mg dust/m3) at a speed of 0.5 RPM to 96.7 mg (equates to ≈ 1095.99 mg dust/m3) at 9.5 RPM.
Figure 3.

Range of utility of WTC oriented String Generator system. Measurements ranged from an output of atmospheres as low as 33 mg/m3 up to ≈1100 mg/m3. Data shown are mean ± SEM. Best+fit value of slope derived from linear regression = 116.2 [± 2.6].
Confirmation of ITIH System Utility for WTC Dust Exposures
Rats here were expected to be exposed to ≈ 100 mg WTC dust/m3 (dust + 2.5% ISO [in O2 carrier gas]) via the ITIH system. During the 81 min period for this one study (as opposed to a normal 2-hr regimen), the rats remained anesthetized and were mechanically ventilated (60 breath/min [0.5 sec for inhale/0.5 sec for exhale]. The rats were euthanized within 1-hr post-exposure and had their lungs removed for measure of lung weight and metal analyses.
The concentration of each WTC-dust generated atmosphere was initially verified by passive filter sampling at the tip of a dedicated insyte tube before and after each exposure. Those measures indicated an atmosphere of ≈ 94 [± 13] mg dust/m3 had been generated for exposure. However, if based solely on filter measures, for a 100 mg/m3 atmosphere and based on a flow rate of 0.67 LPM out of the insyte, in the 81 min exposure, ≈ 55 L of air/dust mixture and a total of 5.43 mg dust should have been delivered to each rat. It was highly unlikely the rats received >50 L in an exposure; thus, we determined that calculations of the atmosphere delivered to the rats would have to be based on system/rat lung parameters [i.e., lung volume, lung capacity, RV, FVC, EEV, volume inflation at 17.5 cm H2O, 60 bpm setting]. Using this approach, a total of 18.87 L air/dust mixture was calculated to have been inhaled in 81 min (27.94 L in 2-hr) and a total of 1.88 mg dust introduced to each rat (≈ 2.79 mg dust for 2 hr). By extrapolating from levels of Ti and Al found in the lungs of each exposed rat (see below), it was calculated that a total of 2.00 (± 0.20) mg dust had been deposited as a result of the 18.87 L of air/dust delivered in this 81 min period. This meant that the actual level of dust the rats were exposed to was 106 mg/m3, well within the range predicted based on measures of the filter measurement. We thus conclude that post-insyte filter measures provided acceptable estimates of atmospheres delivered to the rats in the ITIH system.
While body weights were not statistically different among treatment groups, the results in Figure 4 illustrate that there was a significant increase in lung/trachea weights in rats exposed to WTC dust via ITIH. Specifically, within 1-hr of the single 81-min exposure, lung weights of the WTC rats had significantly increased to ≈1.28 g compared to ISO and naïve rat weights of 1.16 (p < 0.01) and 0.98 (p < 0.0001), respectively. Compared against the naïve rats, this represented a 30% increase due to dust exposure. Oddly, use of ISO anesthetic itself led to an 18% increase in weight; even so, there was a >10% increase in weight even beyond that related to any ISO effect (i.e., due to dust itself). We surmise that delivery of the large amount of dust in the short timeframe - as well as the initial prolonged exposure to ISO faced by rats in this single exposure - was sufficient to induce edema/other changes that contributed to increases in lung/tracheal weights. Analyses are underway to clarify if these/other factors might underlie the weight changes. We are also seeking to clarify if the ISO-induced effect is `lost' by the time of a second exposure (i.e., 24 hr later) or is a novel continuous post-exposure effect not previously reported in the literature.
Figure 4.

Lung weight within 1-hr after the single (81 min) exposure. WTC vs. Air/ISO, p < 0.01; WTC vs. Naïve p < 0.0001. Body weights were not statistically different among treatment groups. Data shown are mean ± SEM.
Lung Metal Burden Analysis
The lungs of exposed rats were analyzed for metal content to allow us to extrapolate to total dust delivery values. Analyses of lung/tracheal tissues clearly revealed significant changes in lung metal burdens due to the WTC dust exposure. Particularly, the data showed that two of three originally hypothesized metal markers (e.g., Sb, Al, Ti) seemed to be good surrogates for WTC exposure. Analyses of tissue samples from rats in the 81-min exposure study revealed that levels of marker Al and Ti were significantly higher in WTC dust-exposed rats than in ISO control and naïve rats. Mean lung levels of Al and Ti were respectively 42.8 (± 6.7) and 5.2 (± 0.9) μg; ISO and naïve rat samples were uniformly below levels of detection. On a per-gram tissue basis, the WTC rat values translated to respectively 33.7 (± 5.4) and 4.1 (± 0.1) μg/g.
In the WTC dusts used in the exposures, total Al and Ti levels averaged 21.4 (± 0.9) and 2.6 (± 0.1) μg/g dust. Additional analyses revealed that in these dusts, only negligible amounts of Ti and only 2.8% of all Al was soluble. Results for Sb were found to be too close to background levels to permit any clear determination of levels present. This outcome was likely attributable to the fact that the majority of Sb in WTC dusts is associated with the fine (WTC2.5) fraction and that that WTC2.5 is only at a very low in presence in the dusts used in the exposures. Nonetheless, based on these values, and the levels of Al and Ti present in the lung/trachea tissue samples, it was calculated that rats received - depending on whether basing the estimate on μg Al/mg dust or μg Ti/mg dust − 2.001 (± 0.310) or 2.004 (± 0.330) mg dust as a result of the 81 min exposure. We conclude from this data that use of either metal is a good marker of WTC dust exposure and that the ITIH system can successfully deliver the precious dusts into the lungs of our rat models.
Discussion
The few in vivo studies performed thus far to examine WTC dust-related health effects did not utilize exposures that accurately reflected conditions on-site in the early days after 9/11. Specifically, these studies used fine fractions (≤ 2.5 μm) of the WTC dusts; in reality, such sizes only constituted ≤ 4% of the total WTC dust by mass (Gavett, 2003; Lioy, et al., 2002; McGee, et al., 2003). In actuality, supercoarse particles (>10 μm) comprised ≥ 96% of the dusts at sites on/around Ground Zero. In addition, these early studies employed methods of exposure that were either non-representative (i.e., intratracheal instillation, oropharyngeal aspiration) or only optimal for smaller size particles (i.e., nose-only inhalation). Any study that sought to perform exposures to WTC dusts in manners comparable to those experienced by FR at Ground Zero would have to take into account the significant amounts of mouth-breathing that occurred for prolonged periods (during heavy labor) and the fact that rats/mice are obligate nose-breathers. As such, with the latter as models for toxicology studies, use of a nose-only approach would be inefficient for the supercoarse WTC particles; filtration/entrapment in nasal passages would be certain and any attempt to correlate dust dose level to toxicologic effects unreliable.
With these challenges in mind, the purpose of this study was to develop a system capable of generating and administering supercoarse WTC particles in a manner that `best' mimicked exposure scenarios faced by FR at Ground Zero on 9/11 and the days immediately thereafter. Essentially, the system should allow these larger diameter particles to circumvent the nasal regions in rat models, thereby introducing them directly into the lungs. Such an approach would permit a more accurate delivery of these dusts and allow Investigators to better correlate dust dose level to any potential toxicological effects that are observed following the exposure(s).
To preserve our precious (i.e., limited) Ground Zero dust stock, a bulk WTC dust sample obtained one block east of the WTC building complex (Cortlandt Street), with chemical and physical characteristics similar to dust located at the collapse pile (albeit with exclusion of > 53 μm fragments that are beyond any capacity for respiratory entrainment), was used in all dust characterization and system validation experiments. However, experiments pertaining to confirmation of the utility of the system via actual WTC dust rodent exposures were conducted using samples collected at Ground Zero (specifically, Liberty Street and Church St.). Like all the other dust samples collected during 9/11–13/2001 by members of our laboratories, these samples were designated as “unique” in that they were present prior to a significant rain on 9/14/01 that altered the physicochemical properties of any dusts present thereafter on or around Ground Zero.
Fishing Line WTC-dust generator
With the new Fishing Line WTC-Dust Generator system, there was a positive association between generation efficiency and increased flow rates. Initial system characterization was done at 15 LPM. This was subsequently lowered to 10 LPM to accommodate the Isoflurane/O2 mixture required for the rats while on the ITIH system (see below) during a WTC dust exposure. In all iterations, the system was pressurized to maintain a maximum displacement of 17.5–20.0 cm water with every `pulse' delivery of dust. Generation at 10 LPM provided a suitable balance between dust generation efficiency and tolerability of the exposed rats. This was a critical variable in that any induction of ventilatory stress could have led to unintended adverse outcomes in the rats' lungs that would confound subsequent interpretation of any dust-induced toxic effects. Thus, it was clear this novel system could be used to deliver WTC dusts to the anesthetized rat hosts without introducing undue artifactual pathologies due to any pressure variations.
ITIH exposure apparatus
To avoid nasal filtration of the aerosolized particles, intratracheal intubation was essential to deliver the generated (mainly) supercoarse particles (WTC10–53) to the lower respiratory tract. The ITIH component (see Figure 2) originally designed by Oberdörster and colleagues - once integrated with the Fishing Line Generator - was essential to enable particle (in conjunction with anesthetic) delivery under controlled breathing conditions (60 bpm). Average flow rates at the exposure ports were 1.019 LPM (at 15 LPM generation flow) and 0.615 (at 10 LPM); thus, particle delivery at each port could be made scalable (in conjunction with the generator) and distributed in a fairly uniform fashion across all ports.
Confirmation of utility of system in actual WTC dust exposures
Rationale of proposed concentrations
Rats were exposed to atmospheres extrapolated from those encountered by mouth-breathing FR during 9/11–9/13. Dusts levels that were used were determined using the Multiple Path Particle Deposition Model program (MPPDep Version 1.11, CIIT, Research Triangle Park, NC; RIVM, Bilthoven, Netherlands). Actual values were based on presumptive 250–1000 mg WTC dust/m3 Ground Zero atmospheres likely encountered by FR (Lorber, Gibb, Grant, Pinto, Pleil and Cleverly, 2007). For each concentration, conversions were made to generate rat equivalents (based on dose per surface area of trachea, bronchial, and alveolar regions of respiratory tracts of both human and rat). Using equations outlined in Jarabek et al. (2005), and since these are polydisperse atmospheres, this meant atmospheres bearing 33, 66, or 99 mg WTC dust/m3 (of aerodynamic diameter ≤ 53 μm) would need to be generated for each 2-hr rat exposure to correspond to exposures that FR facing atmospheres of 250, 500, or 750 mg WTC dust/m3, respectively, underwent during continuous 4-hr periods on/near Ground Zero. This 4-hr value was only deemed representative of a “reference” exposure in 2011 by Mayor Bloomberg's WTC Medical Working Group (L. Gibbs, 2011).
As was shown in the current studies, both the insyte filter data and the extrapolated dust lung burden data from the 81-min proposed 100 mg dust/m3 exposure study gave rise to comparable estimates of actual exposure atmospheres (94–106 mg dust/m3). Ongoing studies in our laboratories using lower exposure levels (i.e., 33 mg dust/m3) for 2-hr periods have yielded similar `predictive' results (Sisco et al., unpublished data). This reproducibility of these types of outcomes with both low and high levels of generated WTC dusts clearly indicates that the Fishing Line-ITIH system can reliably deliver these precious particles to anesthetized rat hosts.
Marker metals
Composition analyses previously showed that WTC dusts with MMAD of ≤ 2.5 (WTC2.5) contained: ppt levels of Sb, Al, calcium (Ca), copper (Cu), magnesium (Mg), iron (Fe), sulfur (S), and silicon (Si); ppm levels of Ti, cadmium (Cd), and zinc (Zn); and, only traces of chromium (Cr), nickel (Ni), lead (Pb), and vanadium (V). In comparison, WTC2.5–10 and WTC10–53 particles contained increasingly higher levels of each metal (except Sb that decreased). Those studies strongly suggested to us three metals in particular, e.g., Sb, Al, and Ti, could be excellent signature components (markers) to indicate host WTC dust exposure. This is in contrast to other metals (such as Ca, Zn, or Fe) that have elevated innate background levels in the lungs.
The present studies found that a single exposure to the WTC dusts led to significant increases in lung/tracheal levels of both Al and Ti; Sb levels were not reliable - an outcome likely related to the fact that the fine fraction was only a very small part of the dust samples used in the exposures here. Further, when the values for Al and Ti burdens in the tissues and the dust samples were concurrently utilized to estimate total dust exposures by the rats, each metal led to a value that was within 5 μg of the other. That data clearly show that use of either metal was a good marker of WTC dust exposure in the rat models exposed via ITIH. Ongoing studies with lower doses of the WTC dusts seek to confirm these findings. It is hoped ultimately that this information will be useful to clinicians to verify identities of those truly exposed to the dusts on-site/in residential areas around Ground Zero as well as to gain a better handle on if the WTC dusts are still trapped in the lungs of FR and other individuals even after all these years.
Conclusions
Overall, the Fishing Line WTC-Dust Generator and integrated ITIH apparatus created here has a potential for a wide variety of applications due to several advantages it has that are not found in/with existing generating methods (i.e., Wright dust feeder, fluidized bed, etc.). This is moreover true in the context of situations wherein there exists a need for high efficiency aerosolization of a large range of aerodynamically sized heterogeneous particles and limitations on the amount of sample available for use. Thus, the novel system here could prove useful particularly for studies that would use precious\limited materials apart from WTC dusts, such as novel nanomaterials, bioagents, moon dusts, etc.
In the more than 10 years since the disaster in Manhattan, there has been an increased recognition of the potential health impact from exposures to and entrainment of the coarse/supercoarse portions of the WTC dusts by FR (see Welden et al. [2010] and Xu et al. {2011]). Accordingly, a Fishing Line-ITIH system was created for the purpose of exposing animal models to such materials and subsequent analyses of dust-induced effects in situ. Based on the results presented here, it is clear now this novel system can be a valuable tool for us and other Investigators to use in our goal of trying to obtain a better understanding of the various lung pathologies that could arise in animal models exposed to the earliest WTC dusts - at representative levels and in scenarios that mimic FR exposures during the now-deemed critical 9/11–13/01 period.
Acknowledgements
This work was supported entirely by funding from CDC/NIOSH grant RO1OH008280 and in part, by NIEHS Center Grant ES00260 and pre-doctoral training grant for Joshua Vaughan from NIEHS (T32 ES007324-12). The Authors declare no conflicts of interest. The authors are alone responsible for the content and writing of the paper.
References
- (CDC) C.f.D.C.a.P. Physical health status of World Trade Center rescue and recovery workers and volunteers - New York City, July 2002-August 2004. MMWR Morbidity and mortality weekly report. 2004;53(35):807–812. [PubMed] [Google Scholar]
- (USGS) U.S.G.S. Clark R, Plumlee G, Meeker G, Swayze G. USGS Fact Sheet 050-02. 2002. Environmental Studies of the World Trade Center Area, New York City, After September 11, 2001. [Google Scholar]
- Antao VC, Pallos LL, Shim YK, Sapp JH, 2nd, Brackbill RM, Cone JE, et al. Respiratory protective equipment, mask use, and respiratory outcomes among World Trade Center rescue and recovery workers. American journal of industrial medicine. 2011;54(12):897–905. doi: 10.1002/ajim.21009. [DOI] [PubMed] [Google Scholar]
- Banauch GI, Alleyne D, Sanchez R, Olender K, Cohen HW, Weiden M, et al. Persistent hyperreactivity and reactive airway dysfunction in firefighters at the World Trade Center. American journal of respiratory and critical care medicine. 2003;168(1):54–62. doi: 10.1164/rccm.200211-1329OC. [DOI] [PubMed] [Google Scholar]
- Banauch GI, Dhala A, Alleyne D, Alva R, Santhyadka G, Krasko A, et al. Bronchial hyperreactivity and other inhalation lung injuries in rescue/recovery workers after the World Trade Center collapse. Critical care medicine. 2005;33(1 Suppl):S102–106. doi: 10.1097/01.ccm.0000151138.10586.3a. [DOI] [PubMed] [Google Scholar]
- Buyantseva LV, Tulchinsky M, Kapalka GM, Chinchilli VM, Qian Z, Gillio R, et al. Evolution of lower respiratory symptoms in New York police officers after 9/11: a prospective longitudinal study. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. 2007;49(3):310–317. doi: 10.1097/JOM.0b013e318032256e. [DOI] [PubMed] [Google Scholar]
- Clary-Meinesz C, Mouroux J, Cosson J, Huitorel P, Blaive B. Influence of external pH on ciliary beat frequency in human bronchi and bronchioles. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 1998;11(2):330–333. doi: 10.1183/09031936.98.11020330. [DOI] [PubMed] [Google Scholar]
- de la Hoz RE, Shohet MR, Chasan R, Bienenfeld LA, Afilaka AA, Levin SM, et al. Occupational toxicant inhalation injury: the World Trade Center (WTC) experience. International archives of occupational and environmental health. 2008;81(4):479–485. doi: 10.1007/s00420-007-0240-x. [DOI] [PubMed] [Google Scholar]
- Edelman P, Osterloh J, Pirkle J, Caudill SP, Grainger J, Jones R, et al. Biomonitoring of chemical exposure among New York City firefighters responding to the World Trade Center fire and collapse. Environmental health perspectives. 2003;111(16):1906–1911. doi: 10.1289/ehp.6315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elder A, Johnston C, Gelein R, Finkelstein J, Wang Z, Notter R, et al. Lung inflammation induced by endotoxin is enhanced in rats depleted of alveolar macrophages with aerosolized clodronate. Experimental lung research. 2005;31(6):527–546. doi: 10.1080/019021490944223. [DOI] [PubMed] [Google Scholar]
- Feldman DM, Baron SL, Bernard BP, Lushniak BD, Banauch G, Arcentales N, et al. Symptoms, respirator use, and pulmonary function changes among New York City firefighters responding to the World Trade Center disaster. Chest. 2004;125(4):1256–1264. doi: 10.1378/chest.125.4.1256. [DOI] [PubMed] [Google Scholar]
- Gaafar H, Girgis R, Hussein M, el-Nemr F. The effect of ammonia on the respiratory nasal mucosa of mice. A histological and histochemical study. Acta oto-laryngologica. 1992;112(2):339–342. doi: 10.1080/00016489.1992.11665429. [DOI] [PubMed] [Google Scholar]
- Gavett SH. World Trade Center fine particulate matter--chemistry and toxic respiratory effects: an overview. Environmental health perspectives. 2003;111(7):971. doi: 10.1289/ehp.111-1241533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geyh AS, Chillrud S, Williams DL, Herbstman J, Symons JM, Rees K, et al. Assessing truck driver exposure at the World Trade Center disaster site: personal and area monitoring for particulate matter and volatile organic compounds during October 2001 and April 2002. Journal of occupational and environmental hygiene. 2005;2(3):179–193. doi: 10.1080/15459620590923154. [DOI] [PubMed] [Google Scholar]
- Herbert R, Moline J, Skloot G, Metzger K, Baron S, Luft B, et al. The World Trade Center disaster and the health of workers: five-year assessment of a unique medical screening program. Environmental health perspectives. 2006;114(12):1853–1858. doi: 10.1289/ehp.9592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hesterberg TW, McConnel EE, Miiller WC, Chevalier J, Everitt J, Thevenaz P, et al. Use of lung toxicity and lung particle clearance to estimate the maximum tolerated dose (MTD) for a fiber glass chronic inhalation study in the rat. Fundamental and applied toxicology : official journal of the Society of Toxicology. 1996;32(1):31–44. doi: 10.1006/faat.1996.0104. [DOI] [PubMed] [Google Scholar]
- Holma B, Lindegren M, Andersen JM. pH effects on ciliomotility and morphology of respiratory mucosa. Archives of environmental health. 1977;32(5):216–226. doi: 10.1080/00039896.1977.10667285. [DOI] [PubMed] [Google Scholar]
- Izbicki G, Chavko R, Banauch GI, Weiden MD, Berger KI, Aldrich TK, et al. World Trade Center “sarcoid-like” granulomatous pulmonary disease in New York City Fire Department rescue workers. Chest. 2007;131(5):1414–1423. doi: 10.1378/chest.06-2114. [DOI] [PubMed] [Google Scholar]
- Kim H, Herbert R, Landrigan P, Markowitz SB, Moline JM, Savitz DA, et al. Increased rates of asthma among World Trade Center disaster responders. American journal of industrial medicine. 2012;55(1):44–53. doi: 10.1002/ajim.21025. [DOI] [PubMed] [Google Scholar]
- L. Gibbs TF, Aldrich TK, Cohen MD, Difede J, Gelberg KH, Greene C, Kleinman EJ, Landrigan PJ, Leinhardt RR, Prezant D, Raju R, Reibman J, Sadler P, Slone MS, Thorpe L, World Trade Center Medical Working Group . 2011 Annual Report on 9/11 Health. 2011. [Google Scholar]
- Landrigan PJ, Lioy PJ, Thurston G, Berkowitz G, Chen LC, Chillrud SN, et al. Health and environmental consequences of the world trade center disaster. Environmental health perspectives. 2004;112(6):731–739. doi: 10.1289/ehp.6702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ledbetter AD, Killough PM, Hudson GF. A low-sample-consumption dry-particulate aerosol generator for use in nose-only inhalation exposures. Inhalation Toxicol. 1998;10(3):239–251. [Google Scholar]
- Lioy PJ, Weisel CP, Millette JR, Eisenreich S, Vallero D, Offenberg J, et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environmental health perspectives. 2002;110(7):703–714. doi: 10.1289/ehp.02110703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorber M, Gibb H, Grant L, Pinto J, Pleil J, Cleverly D. Assessment of inhalation exposures and potential health risks to the general population that resulted from the collapse of the World Trade Center towers. Risk analysis : an official publication of the Society for Risk Analysis. 2007;27(5):1203–1221. doi: 10.1111/j.1539-6924.2007.00956.x. [DOI] [PubMed] [Google Scholar]
- Lowers HA, Meeker GP, Lioy PJ, Lippmann M. Summary of the development of a signature for detection of residual dust from collapse of the World Trade Center buildings. Journal of exposure science & environmental epidemiology. 2009;19(3):325–335. doi: 10.1038/jes.2008.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maciejczyk Polina B, Zeisler Rolf L, Hwang J-S, Thurston George D, Chen Lung C. Urban Aerosols and Their Impacts. Vol. 919. American Chemical Society; 2005. Characterization of Size-Fractionated World Trade Center Dust and Estimation of Relative Dust Contribution to Ambient Particulate Concentrations; pp. 114–131. [Google Scholar]
- McGee JK, Chen LC, Cohen MD, Chee GR, Prophete CM, Haykal-Coates N, et al. Chemical analysis of World Trade Center fine particulate matter for use in toxicologic assessment. Environmental health perspectives. 2003;111(7):972–980. doi: 10.1289/ehp.5930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendelson DS, Roggeveen M, Levin SM, Herbert R, de la Hoz RE. Air trapping detected on end-expiratory high-resolution computed tomography in symptomatic World Trade Center rescue and recovery workers. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. 2007;49(8):840–845. doi: 10.1097/JOM.0b013e3180d09e87. [DOI] [PubMed] [Google Scholar]
- Nolan A, Naveed B, Comfort AL, Ferrier N, Hall CB, Kwon S, et al. Inflammatory Biomarkers Predict Airflow Obstruction After Exposure to World Trade Center Dust. Chest. 2011 doi: 10.1378/chest.11-1202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oberdorster G, Cox C, Gelein R. Intratracheal instillation versus intratracheal-inhalation of tracer particles for measuring lung clearance function. Experimental lung research. 1997;23(1):17–34. doi: 10.3109/01902149709046045. [DOI] [PubMed] [Google Scholar]
- Offenberg JH, Eisenreich SJ, Chen LC, Cohen MD, Chee G, Prophete C, et al. Persistent organic pollutants in the dusts that settled across lower Manhattan after September 11, 2001. Environmental science & technology. 2003;37(3):502–508. doi: 10.1021/es025730g. [DOI] [PubMed] [Google Scholar]
- Olson DA, Norris GA, Landis MS, Vette AF. Chemical Characterization of Ambient Particulate Matter near the World Trade Center: Elemental Carbon, Organic Carbon, and Mass Reconstruction. Environmental science & technology. 2004;38(17):4465–4473. doi: 10.1021/es030689i. [DOI] [PubMed] [Google Scholar]
- Oppenheimer BW, Goldring RM, Herberg ME, Hofer IS, Reyfman PA, Liautaud S, et al. Distal airway function in symptomatic subjects with normal spirometry following World Trade Center dust exposure. Chest. 2007;132(4):1275–1282. doi: 10.1378/chest.07-0913. [DOI] [PubMed] [Google Scholar]
- Osier M, Oberdorster G. Intratracheal inhalation vs intratracheal instillation: differences in particle effects. Fundamental and applied toxicology : official journal of the Society of Toxicology. 1997;40(2):220–227. doi: 10.1006/faat.1997.2390. [DOI] [PubMed] [Google Scholar]
- Prevention) C.C.f.D.C.a. Injuries and illnesses among New York City Fire Department rescue workers after responding to the World Trade Center attacks. MMWR Morbidity and mortality weekly report. 2002;51(Spec No):1–5. [PubMed] [Google Scholar]
- Prezant DJ, Weiden M, Banauch GI, McGuinness G, Rom WN, Aldrich TK, et al. Cough and bronchial responsiveness in firefighters at the World Trade Center site. The New England journal of medicine. 2002;347(11):806–815. doi: 10.1056/NEJMoa021300. [DOI] [PubMed] [Google Scholar]
- Prezant DJ. World Trade Center Cough Syndrome and its treatment. Lung. 2008;186(Suppl 1):S94–102. doi: 10.1007/s00408-007-9051-9. [DOI] [PubMed] [Google Scholar]
- Rom WN, Reibman J, Rogers L, Weiden MD, Oppenheimer B, Berger K, et al. Emerging exposures and respiratory health: World Trade Center dust. Proc Am Thorac Soc. 2010;7(2):142–145. doi: 10.1513/pats.200908-092RM. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salzman SH, Moosavy FM, Miskoff JA, Friedmann P, Fried G, Rosen MJ. Early respiratory abnormalities in emergency services police officers at the World Trade Center site. Journal of occupational and environmental medicine / American College of Occupational and Environmental Medicine. 2004;46(2):113–122. doi: 10.1097/01.jom.0000111612.68916.d0. [DOI] [PubMed] [Google Scholar]
- Skloot G, Goldman M, Fischler D, Goldman C, Schechter C, Levin S, et al. Respiratory symptoms and physiologic assessment of ironworkers at the World Trade Center disaster site. Chest. 2004;125(4):1248–1255. doi: 10.1378/chest.125.4.1248. [DOI] [PubMed] [Google Scholar]
- Szeinuk J, Padilla M, de la Hoz RE. Potential for diffuse parenchymal lung disease after exposures at World Trade Center Disaster site. The Mount Sinai journal of medicine, New York. 2008;75(2):101–107. doi: 10.1002/msj.20025. [DOI] [PubMed] [Google Scholar]
- Toren K, Brisman J, Hagberg S, Karlsson G. Improved nasal clearance among pulp-mill workers after the reduction of lime dust. Scandinavian journal of work, environment & health. 1996;22(2):102–107. doi: 10.5271/sjweh.117. [DOI] [PubMed] [Google Scholar]
- United States Environmental Protection Agency (US EPA) EPA/600/R-02/002A. 2002. Exposure and Human Health Evaluation of Airborne Pollution from the World Trade Center Disaster (External Review Draft) [Google Scholar]
- United States Environmental Protection Agency (US EPA) O.o.I.G. Evaluation Report Report No 2003-P-00012. 2003. EPA's Response to the World Trade Center Collapse: Challenges, Successes, and Areas for Improvement. [Google Scholar]
- Weakley J, Webber MP, Gustave J, Kelly K, Cohen HW, Hall CB, et al. Trends in respiratory diagnoses and symptoms of firefighters exposed to the World Trade Center disaster: 2005–2010. Preventive medicine. 2011;53(6):364–369. doi: 10.1016/j.ypmed.2011.09.001. [DOI] [PubMed] [Google Scholar]
- Webber MP, Gustave J, Lee R, Niles JK, Kelly K, Cohen HW, et al. Trends in respiratory symptoms of firefighters exposed to the world trade center disaster: 2001–2005. Environmental health perspectives. 2009;117(6):975–980. doi: 10.1289/ehp.0800291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiden MD, Ferrier N, Nolan A, Rom WN, Comfort A, Gustave J, et al. Obstructive airways disease with air trapping among firefighters exposed to World Trade Center dust. Chest. 2010;137(3):566–574. doi: 10.1378/chest.09-1580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wheeler K, McKelvey W, Thorpe L, Perrin M, Cone J, Kass D, et al. Asthma diagnosed after 11 September 2001 among rescue and recovery workers: findings from the World Trade Center Health Registry. Environmental health perspectives. 2007;115(11):1584–1590. doi: 10.1289/ehp.10248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeig-Owens R, Webber MP, Hall CB, Schwartz T, Jaber N, Weakley J, et al. Early assessment of cancer outcomes in New York City firefighters after the 9/11 attacks: an observational cohort study. Lancet. 2011;378(9794):898–905. doi: 10.1016/S0140-6736(11)60989-6. [DOI] [PMC free article] [PubMed] [Google Scholar]