

Abstract
Background:
There is limited evidence about the chronic pelvic pain syndrome (CPPS) treatment by shockwave therapy, and the aim of this study was to evaluate the effect of extracorporeal shockwave therapy on CPPS due to non bacterial prostatitis in a long-term period.
Materials and Methods:
In a follow-up survey, 40 patients with CPPS (that were randomly distributed into the treatment or sham groups were evaluated at 16, 20, and 24 weeks. In the treatment group, patients were treated by extracorporeal shock wave therapy (ESWT) once a week for 4 weeks by a protocol of 3000 impulses, 0.25 mJ/m2 and 3 Hz of frequency. 0.05 mJ/m2 were added in each week. In the sham group, the same protocol was applied, but with the probe being turned off. The follow-up assessments were done by visual analog scale for pain and National Institutes of Health-developed Chronic Prostatitis Symptom Index (NIH-CPSI). Data were compared using independent t-test or analysis of variences.
Results:
Three patients did not complete the study protocol, 37 patients were evlauated (19 patients in treatment and 18 patients in the sham group). At week 24, the mean of pain score, urinary score, quality-of-life and NIH-CPSI score between two groups were not statistically different.
Conclusion:
Although, ESWT therapy as a safe and effective therapy in CPPS in short-term follow-up has been established, its long-term efficacy was not supported by this study.
Keywords: Chronic pelvic pain syndrome, extracorporeal shock wave therapy, long-term, treatment
INTRODUCTION
Chronic prostatitis is a common complaint among adult males with the prevalence of the condition reported at 10%.[1] Chronic prostatitis is more commonly associated with nonbacterial causes;[1] however, there have been studies that have shown that some cases of chronic prostatitis are not correctly labeled as nonbacterial and as a result strict criteria should be met if the diagnosis of nonbacterial chronic prostatitis is to be made.[2] Chronic nonbacterial prostatitis (CNBP) is the leading cause of chronic pelvic pain syndrome (CPPS) in males[3] with some considering these entities the same in male populations;[4] the diagnosis of this condition is made when there is persistent genito-urinary pain originating from the prostate for more than 3 months with no evidence of infection present.[5] The patients affected by CNBP usually complain from pain and/or discomfort in the rectal or perianal region with some degree of voiding problems.[6] These patients are usually evaluated using the National Institutes of Health-Chronic Prostatitis Symptom Index questionnaire (NIH-CPSI), physical examination, urodynamic studies combined with a complete urinary bacterial workup,[5,7] the four glass test is also used to further distinguish the subtypes of chronic prostatitis.[8]
Despite being a common condition with significant adverse effects on the quality-of-life (QOL) of the patients, the etiologies, pathogenesis and treatment of this condition have remained problematic and elusive.
The etiology of CNBP remains elusive, but some have noted similarities between this condition and interstitial cystitis.[9] Different pathological processes have been implicated in the pathogenesis of this condition including recurrent infections and prolonged abstinence[10,11] In regards to treatment of the condition a multitude of different approaches have been attempted over the years; although, there has been no conclusive evidence in support of any of these approaches.[12] As a general advice, it has been suggested that patients with chronic prostatitis refrain from the following activities: Drinking alcoholic or carbonated beverages, eating spices, cycling, and sitting on cold surfaces.[13]
Due to the possibility of chronic bacterial prostatitis being misdiagnosed as CNBP, some authors have suggested that an empirical trial period of anti-microbial treatment may be attempted at first especially in the inflammatory subtypes of the condition.[13,14] Some have even suggested the use of antibiotics (especially newer generation fluorquinolones) can be used in noninflammatory cases.[15] For the noninflammatory subtype of CNBP many different treatment approaches with varying degrees of success have been attempted; these approaches include the following: One of the approaches suggested for treatment of CNBP is the injection of botulinum toxin with some studies showing promising results.[16] Alpha blockers have also been suggested as a possible treatment choice for the condition[17] with some suggesting a combination of alpha blockers and fluoroquinolones.[18] In other studies, finasteride was used in the treatment of the condition.[19,20] Among other approaches used for treatment of this condition, we can point to transurethral microwave thermotherapy,[21,22] osteopathic remedies,[23] acupuncture,[24] and holistic approaches.[25]
Extracorporeal shockwave therapy has shown promise in other chronic conditions such as diabetic wounds[26] and due to its effects on inhibition of chronic inflammatory processes, it has been applied to CPPS/CNBP`1 as well with studies showing a positive effect especially in pain relief.[27,28,29,30] In our previous paper, we studied the effects of this treatment modality on CPPS/CBNP and found that it was a safe and effective method in treatment of the condition in short-term,[31] in this paper, we have followed-up the patients at 16, 20, and 24 weeks after intervention in order to evaluate the effects of extracorporeal shockwave therapy in a long-term period.
MATERIALS AND METHODS
In the original study, 40 patients were recruited and randomly assigned to two groups: The treatment group and the sham group.[31] These patients were chosen from a pool of patients with chronic prostatitis type IIIB (as classified by the NIH) and after obtaining informed consent, they were included in the study. The inclusion criteria consisted of: Chronic pelvic pain for more than 3 months and definitive diagnosis of chronic prostatitis/CPPS. Any patient who had a history of drug/narcotics abuse or had abnormalities in imaging workup was excluded from the study. In the study group, the patients received extracorporeal shock wave therapy (ESWT) treatment on an once weekly basis for 4 weeks; in each session 3000 impulses, with an energy of 0.25 mJ/mm2 and frequency of 3 Hz were delivered, with weekly increments of 0.05 mJ/mm2. After 500 pulses were delivered, the probe position was adjusted by means of transperineal ultrasound. In the sham group, the same protocol was adhered to with the exception that the probe was turned off. We used the standard electromagnetic DUOLITH SD1, Storz Medical, Tȧgerwilen, Switzerland. The kind of shock wave was focus. In the original study the patients were followed-up from first week to week 12,[31] but in this follow-up study we followed the same patients until 24 weeks posttreatment to understand the long-term effects of the treatment protocol. The study protocol was approved by the Ethics Committee of Isfahan University of Medical Sciences (390528).
The evaluation of patients was performed using visual analog scale (VAS, 0-10),[32] NIH-CPSI.[33] NIH-CPSI address the three most important domains of chronic prostatitis, which are pain, urinary function and quality-of-life. Data collected data were entered into an IBM SPSS (SPSS Inc. Released 2009. PASW Statistics for Windows, Version 18.0. Chicago, USA) database and analyzed using the same software. Chi-square, independent t-test, and repeated analysis of variences were used for statistical analyses.
RESULT
During the study follow-up, three patients did not complete the study protocol and hence 37 eligible patients were randomly allocated into two groups. There were 19 patients in treatment and 18 patients in sham group. The mean age in treatment and sham groups were 34.4 ± 8.4 and 36 ± 10.1 years old, respectively (P value: Not significant). In our previous study all four domains were statistically different at week 3 and week 12 [Figure 1]. It should be notice that in all four domains as well as pain score in both groups, worse outcomes were achieved at each follow-up compared with previous. At week 24, the mean of pain score, urinary score, QOL and NIH-CPSI score between two groups were not statistically different [Table 1]. At week 24, all four domains were not statistically different from the baseline.
Figure 1.
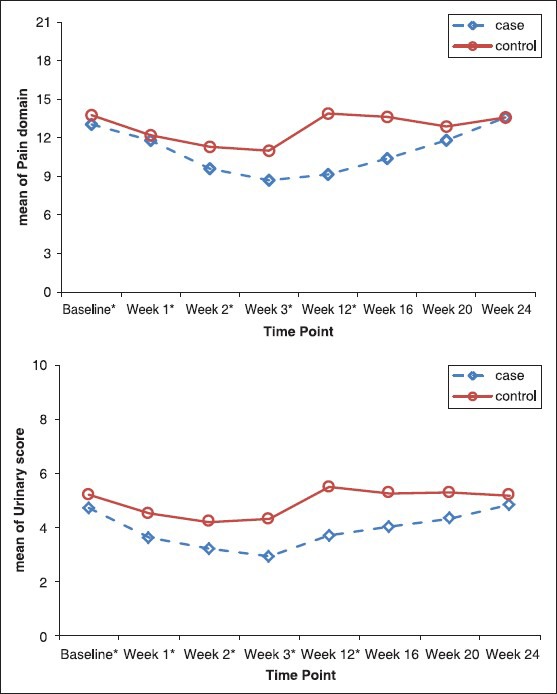
Line chart of the mean of pain domain, urinary score, quality-of-life and National Institutes of Health-Chronic Prostatitis Symptom Index scores between study groups at time points[31]
Table 1.
Comparison of the mean of pain domain, urinary score, QOL, and NIH-CPSI scores between study groups at time points
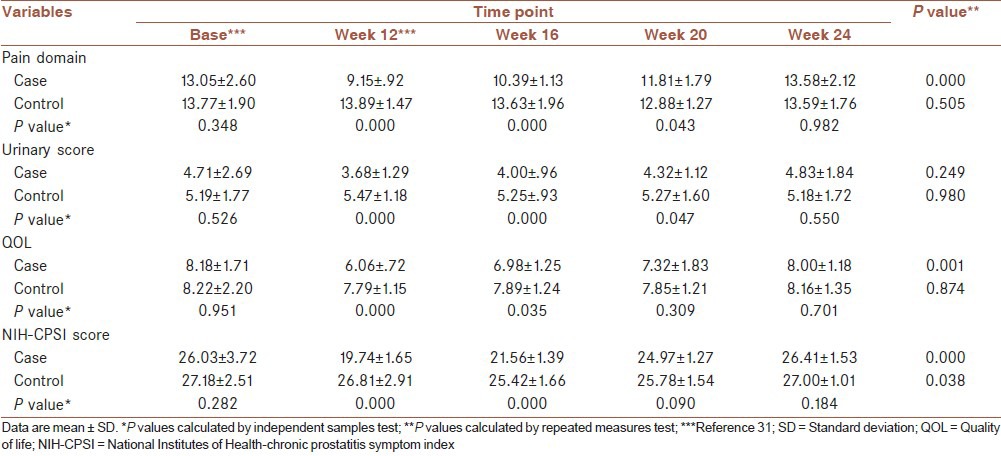
Figure 1 exhibited that deterioration in the values of pain domain, urinary score, QOL and total NIH-CPSI score during study period in treatment and sham group.
DISCUSSION
Our study revealed that in long-term follow-up, total NIH-CPSI, pain and urinary symptom scores as well as QOL deteriorated in both groups; although, it was more significantly in ESWT compared with sham group. In week 20 and 24 follow-up, there were not statistically significant differences between ESWT and sham groups in all four aspects.
According to our literature review, no study was found about the efficacy of ESWT on CPPS with long-term follow-up to 24 weeks. Our previous study showed that total NIH-CPSI, pain and urinary symptom scores as well as QOL improved significantly in ESWT compared with sham group; although, we encountered deterioration in all fields at week 12 of follow-up compared with week 3.[31] In recent study, all aspects including pain domain, urinary score, QOL and NIH-CPSI score deteriorated by the time in follow-up week 16, week 20 and week 24. These findings were in concordance with our previous, which showed worse outcomes in week 12 in comparison with week 3. It was noticeable that the outcomes in 6 months follow-up was very close to baseline, which made a question on long-term effect of ESWT on CPPS [Table 1].
In two recent studies by Zimmermann et al., in first study,[29] they showed statistically significant improvements in pain and QOL after ESWT although voiding conditions, improved but with no statistical significance. In their later one, they found[30] reduced pain and improved QOL in a significantly greater proportion of patients who underwent ESWT treatment. In another study by Yan et al.,[26] randomized study with 80 CPPS patients, NIH-CPSI, QOL and the pain domain scores significantly improved compared to the baseline at all posttreatment time points in ESWT group. In their follow-up, the exacerbation of NIH-CPSI, pain and symptom score on follow-up 12 week in both groups was in agreement with our findings. In similar study by Zeng et al.[28] also ESWT showed significant improvement in pain domain and QOL up 12 week follow-up. One important issue that should be noticed is the maximum follow-up in these studies that are 12 weeks, which reflect the short-term follow-up. Our study is the first long-term follow-up, which challenge the persistence of therapeutic effect of ESWT therapy. Therefore, more comprehensive research with long-term follow-up is needed to approve our findings.
The first limitation of our study was small sample size. The second was missing International Prostate Symptom score and erectile function. Absence of standard protocol for ESWT therapy was the third one.
CONCLUSION
Our studies confirmed ESWT therapy as a safe and effective therapy in CPPS in short-term follow-up, although its long-term efficacy was not supported by ours and more comprehensive surveys so as to describe a standard protocol ESWT with long follow-up are essential.
ACKNOWLEDGMENTS
It is part of thesis done by Dr. Amir Moayednia with register no. 390528 Isfahan University of Medical Science. Great thanks of this university and also Kashani Hospital.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Balvocius A. Chronic prostatitis with chronic pelvic pain syndrome. Medicina (Kaunas) 2002;38(Suppl 1):36–41. [PubMed] [Google Scholar]
- 2.Badalyan RR, Fanarjyan SV, Aghajanyan IG. Chlamydial and ureaplasmal infections in patients with nonbacterial chronic prostatitis. Andrologia. 2003;35:263–5. [PubMed] [Google Scholar]
- 3.Krieger JN, Jacobs RR, Ross SO. Does the chronic prostatitis/pelvic pain syndrome differ from nonbacterial prostatitis and prostatodynia? J Urol. 2000;164:1554–8. [PubMed] [Google Scholar]
- 4.Hochreiter W, Bader P. Etiopathogenesis of prostatitis. Urologe A. 2001;40:4–8. doi: 10.1007/s001200050424. [DOI] [PubMed] [Google Scholar]
- 5.Delavierre D, Rigaud J, Sibert L, Labat JJ. Symptomatic approach to chronic prostatitis/chronic pelvic pain syndrome. Prog Urol. 2010;20:940–53. doi: 10.1016/j.purol.2010.09.018. [DOI] [PubMed] [Google Scholar]
- 6.Donovan DA, Nicholas PK. Prostatitis: Diagnosis and treatment in primary care. Nurse Pract. 1997;22:144–6. 149. [PubMed] [Google Scholar]
- 7.Gonzalez RR, Te AE. Is there a role for urodynamics in chronic nonbacterial prostatitis? Curr Urol Rep. 2006;7:335–8. doi: 10.1007/s11934-996-0014-0. [DOI] [PubMed] [Google Scholar]
- 8.Lenk S. Diagnosis of chronic prostatitis. Urologe A. 2001;40:9–11. doi: 10.1007/s001200050425. [DOI] [PubMed] [Google Scholar]
- 9.Forrest JB, Nickel JC, Moldwin RM. Chronic prostatitis/chronic pelvic pain syndrome and male interstitial cystitis: Enigmas and opportunities. Urology. 2007;69:60–3. doi: 10.1016/j.urology.2006.08.1106. [DOI] [PubMed] [Google Scholar]
- 10.Schaeffer AJ. Etiology and management of chronic pelvic pain syndrome in men. Urology. 2004;63(3 Suppl 1):75–84. doi: 10.1016/j.urology.2003.11.002. [DOI] [PubMed] [Google Scholar]
- 11.Lv C, Zhong Z, Wu Z, Xiao N, Yang M, Zhao X. Nonbacterial prostatitis in Kunming mouse induced by long-term stimuli of passive sexual abstinence. J Androl. 2010;31:244–9. doi: 10.2164/jandrol.109.007559. [DOI] [PubMed] [Google Scholar]
- 12.Schaeffer AJ, Datta NS, Fowler JE, Jr, Krieger JN, Litwin MS, Nadler RB, et al. Overview summary statement. Diagnosis and management of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) Urology. 2002;60:1–4. doi: 10.1016/s0090-4295(02)01979-9. [DOI] [PubMed] [Google Scholar]
- 13.Krhen I, Skerk V, Schönwald S, Mareković Z. Classification, diagnosis and treatment of prostatitis syndrome. Lijec Vjesn. 2002;124:89–98. [PubMed] [Google Scholar]
- 14.Lipsky BA. Prostatitis and urinary tract infection in men: What's new; what's true? Am J Med. 1999;106:327–34. doi: 10.1016/s0002-9343(99)00017-0. [DOI] [PubMed] [Google Scholar]
- 15.Kunishima Y, Takeyama K, Takahashi S, Matsukawa M, Koroku M, Tanda H, et al. Gatifloxacin treatment for chronic prostatitis: A prospective multicenter clinical trial. J Infect Chemother. 2008;14:137–40. doi: 10.1007/s10156-008-0593-4. [DOI] [PubMed] [Google Scholar]
- 16.Chuang YC, Chancellor MB. The application of botulinum toxin in the prostate. J Urol. 2006;176 (6 Pt 1):2375–82. doi: 10.1016/j.juro.2006.07.127. [DOI] [PubMed] [Google Scholar]
- 17.Datta NS. Role of alpha-blockers in the treatment of chronic prostatitis. Urology. 2002;60(6 Suppl):27–8. doi: 10.1016/s0090-4295(02)02302-6. [DOI] [PubMed] [Google Scholar]
- 18.Kulovac B, Aganović D, Prcić A, Hadziosmanović O. Management of chronic nonbacterial prostatitis/chronic pelvic pain syndrome. Bosn J Basic Med Sci. 2007;7:245–9. doi: 10.17305/bjbms.2007.3053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Holm M, Meyhoff HH. Chronic prostatic pain. A new treatment option with finasteride? Scand J Urol Nephrol. 1997;31:213–5. doi: 10.3109/00365599709070335. [DOI] [PubMed] [Google Scholar]
- 20.Nickel JC, Downey J, Pontari MA, Shoskes DA, Zeitlin SI. A randomized placebo-controlled multicentre study to evaluate the safety and efficacy of finasteride for male chronic pelvic pain syndrome (category IIIA chronic nonbacterial prostatitis) BJU Int. 2004;93:991–5. doi: 10.1111/j.1464-410X.2003.04766.x. [DOI] [PubMed] [Google Scholar]
- 21.Liatsikos EN, Dinlenc CZ, Kapoor R, Smith AD. Transurethral microwave thermotherapy for the treatment of prostatitis. J Endourol. 2000;14:689–92. doi: 10.1089/end.2000.14.689. [DOI] [PubMed] [Google Scholar]
- 22.Mené MP, Ginsberg PC, Finkelstein LH, Manfrey SJ, Belkoff L, Ogbolu F, et al. Transurethral microwave hyperthermia in the treatment of chronic nonbacterial prostatitis. J Am Osteopath Assoc. 1997;97:25–30. doi: 10.7556/jaoa.1997.97.1.25. [DOI] [PubMed] [Google Scholar]
- 23.Marx S, Cimniak U, Beckert R, Schwerla F, Resch KL. Chronic prostatitis/chronic pelvic pain syndrome. Influence of osteopathic treatment-a randomized controlled study. Urologe A. 2009;48:1339–45. doi: 10.1007/s00120-009-2088-z. [DOI] [PubMed] [Google Scholar]
- 24.Posadzki P, Zhang J, Lee MS, Ernst E. Acupuncture for chronic nonbacterial prostatitis/chronic pelvic pain syndrome: A systematic review. J Androl. 2012;33:15–21. doi: 10.2164/jandrol.111.013235. [DOI] [PubMed] [Google Scholar]
- 25.Potts JM. Nonpharmacological approaches for the treatment of urological chronic pelvic pain syndromes in men. Curr Urol Rep. 2009;10:289–94. doi: 10.1007/s11934-009-0047-2. [DOI] [PubMed] [Google Scholar]
- 26.Yan X, Yang G, Cheng L, Chen M, Cheng X, Chai Y, et al. Effect of extracorporeal shock wave therapy on diabetic chronic wound healing and its histological features. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2012;26:961–7. [PubMed] [Google Scholar]
- 27.Qin X, Lu YP. Application of extracorporeal shockwave therapy in andrology. Zhonghua Nan Ke Xue. 2012;18:1125–9. [PubMed] [Google Scholar]
- 28.Zeng XY, Liang C, Ye ZQ. Extracorporeal shock wave treatment for non-inflammatory chronic pelvic pain syndrome: A prospective, randomized and sham-controlled study. Chin Med J (Engl) 2012;125:114–8. [PubMed] [Google Scholar]
- 29.Zimmermann R, Cumpanas A, Hoeltl L, Janetschek G, Stenzl A, Miclea F. Extracorporeal shock-wave therapy for treating chronic pelvic pain syndrome: A feasibility study and the first clinical results. BJU Int. 2008;102:976–80. doi: 10.1111/j.1464-410X.2008.07742.x. [DOI] [PubMed] [Google Scholar]
- 30.Zimmermann R, Cumpanas A, Miclea F, Janetschek G. Extracorporeal shock wave therapy for the treatment of chronic pelvic pain syndrome in males: A randomised, double-blind, placebo-controlled study. Eur Urol. 2009;56:418–24. doi: 10.1016/j.eururo.2009.03.043. [DOI] [PubMed] [Google Scholar]
- 31.Vahdatpour B, Alizadeh F, Moayednia A, Emadi M, Khorami MH, Haghdani S. Efficacy of extracorporeal shock wave therapy for the treatment of chronic pelvic pain syndrome: A randomized, controlled trial. ISRN Urol. 2013;2013:972601. doi: 10.1155/2013/972601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Huskisson EC. Measurement of pain. Lancet. 1974;2:1127–31. doi: 10.1016/s0140-6736(74)90884-8. [DOI] [PubMed] [Google Scholar]
- 33.Litwin MS, McNaughton-Collins M, Fowler FJ, Jr, Nickel JC, Calhoun EA, Pontari MA, et al. The National Institutes of Health Chronic Prostatitis Symptom Index: Development and validation of a new outcome measure. Chronic Prostatitis Collaborative Research Network. J Urol. 1999;162:369–75. doi: 10.1016/s0022-5347(05)68562-x. [DOI] [PubMed] [Google Scholar]