

Abstract
Bicornuate uterus has two symmetric uterine cavities that are fused caudally and have some degree of communication between two cavities, usually at the uterine isthmus. A complete bicornuate uterus has a seperatory cleft of tissue that is extended to the internal OS. Lesser degree of septation of the two uterine horns has constitution, a partial bicornuate uterus. Bicornuate uterus is a class of four anomaly of American fertility society classification of mullerian anomalies. Here we report a case of a 19-year-old female patient with complaint of abdominal pain and spotting since 4 months ago. In sonography it revealed bicornuate uterus and hematocolpos. The patient underwent general anesthesia and examination that reveal the transverse vaginal septum. Septum removed by resectoscope was successful.
Keywords: Bicornuate uterus, vaginal septum, hematocolpos
INTRODUCTION
Bicornuate uterus is a type of lateral fusion disorder of the mullerian ducts.[1]
Congenital uterine anomaly is more common and generally is recognized by many practicing clinicians. Distribution of mullerian anomaly is septet (34%), bicornuate (39%), didelphic (11%), arcuate (7%), unicorn (5%), hypoplastic and aplastic and other forms (4%).[2]
Uterine didelphys (class III) anomaly is distinguished from bicornuate and septate uteri by the presence of complete non-fusion of the cervix and hemiuterine cavity. Heinonen[3] reported that all 26 women with a uterine didelphys had a longitudinal vaginal septum as well. Occasionally one hemivagina is obstructed by an oblique or transverse vaginal septum.[4,5,6]
Heinonen reported 70% of successful pregnancy outcomes. There was preterm delivery in 20%, fetal growth restriction in 10%, and breech presentation in 43%.
In a study of Tzialidou, predominance of imperforated hemivagina: 69.2% right-sided versus 30.8% left sided septum; 84.6% previous surgical interventions in the study group, such as partial removal of the septum and re-obliteration, unilateral salpingo-ovariectomy and vaginal drainage of pyometra. They used a single transvaginal surgical procedure, including the removal of the obstructed vaginal septum and marsupialization of the blind hemivagina.[7]
CASE REPORT
Here, we report a case of a 19-year-old female patient with complaint of dysmenorrheal, spotting, and severe abdominal pain since past 6 months. She had abnormal menstruation cycle from past 5 years. The patient also complained that after finishing her last menstruation cycle in November 2012, she had spotting for 50 days. As she was virgin, no physicians examined her hymen or urogenital area. In some sonographic reports hematocolpos was reported, and the other sonographic reports indicate a dens mass or tumor. Of course, bicornuate uterus and collection of clot in the left horn and cervix was seen too. Because of this reason the patient had menstruation cycle from one horn of uterus, but another horn was blocked by an oblique septum so it makes for her hematocolpos and hematometra. Kidney sonographic report was normal. Finally, magnetic resonance imaging (MRI) was requested for the patient. In MRI [Figure 1] report, bicornuate uterus and hydrometrocolpos was seen.
Figure 1.
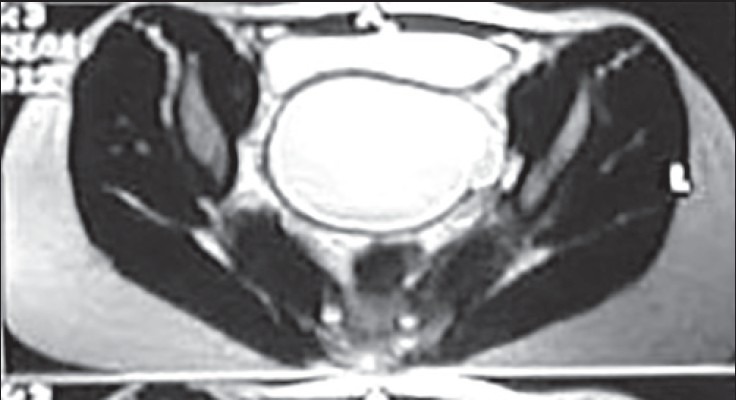
MRI for hematometra because of transverse vaginal septum
As the patient was virgin and virginity in Iran has ethical and legal importance, she was examined by giving her a legal certificate from the official physicians, under general anesthesia in Alzahra hospital operating room in December 2012. Hymen was annular and intact. An oblique vaginal septum near the cervix had touched then septum removed by resectoscope. Thick chocolate liquid extracts. After the surgery, hymenorrhaphy was done on the patient. After 2 days, the patient recovery and was discharged from the hospital.
DISCUSSION
Bicornuate uterus and vaginal septum are congenital defect of the female genital tract.[2]
According to the American Fertility Society classification of mullerian duct anomalies, bicornuate uterus is a class IV anomaly. Incidence of this anomaly varies. This may affect a woman's obstetric as well as her gynecologic outcome.[1]
A bicornuate uterus is caused by incomplete lateral fusion of the mullerian ducts. It is characterized by two separate but communicating endometrial cavities.[2] Mullerian anomaly is divided in to seven classes (unicorn, bicorn, septate, arcuate, didelphys, hypoplastic and apalastic, associated with DES).
External fundal depressions of variable depths are associating with a septate uterus, indicating the coexistence of the two anomalies.[8]
Sergio is present in the patient with severe dysmenorrheal with septate uterus and cervical duplication and longitudinal vaginal septum.[9] Bicornuate uterus is associated with infertility. Unfortunately, bicornuate uterus is mostly a birth defect. Pregnancy cannot be carried out successfully even if the fertilized egg is implanted. Bicornuate uterus can be diagnosis by method of sonography, MRI, HSG, hysteroscopy and laparoscopy. Bicornuate uterus could be one of the causes of female infertility, the woman can conceive. She will face numerous complicate to carry on with the pregnancy and deliver successfully. Singh et al,[10] presented the pregnant woman with bicornuate uterus that presented with acute abdomen rule of ectopic pregnancy.[10] Also Nepal department of obstetrics and gynecology presented the woman with term pregnancy with complete bicornuate uterus and with complete longitudinal vaginal septum.[1]
In a case report study of Kumar et al,[11] the MRI showed bicornuate uterus and cervical agenesis. Hysterectomy and repair of the uterovesical fistula was done. The vagina was reconstructed using an amniotic mould.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Suwal A, Kumar A. Complete bicornuate uterus with complete longitudinal vaginal septum. JNMA J Nepal Med Assoc. 2010;49:243–6. [PubMed] [Google Scholar]
- 2.Cunningham FG, Leveno KJ, Bloom SL, Hauth JC, Rose DJ, Spong CY. Reproductive tract Abnormalities. In: Cunningham FG, Leveno KJ, Bloom SL, Hauth JC, Rose DJ, Spong CY, editors. Williams Obstetrics. 23rd ed. New York: McGraw Hill; 2010. pp. 895–6. [Google Scholar]
- 3.Heinonen PK. Uterus didelphys: A report of 26 cases. Eur J Obstet Gynecol Reprod Biol. 1984;17:345–50. doi: 10.1016/0028-2243(84)90113-8. [DOI] [PubMed] [Google Scholar]
- 4.Asha B, Manila K. An unusual presentation of uterus didelphys with obstructed hemivagina with ipsilateral renal agenesis. (e-10).Fertil Steril. 2008;90:849. doi: 10.1016/j.fertnstert.2007.08.003. [DOI] [PubMed] [Google Scholar]
- 5.Coskun A, Okur N, Ozdemir O, Kiran G, Arykan DC. Uterus didelphys with an obstructed unilateral vagina by a transvaginal septum associated with ipsilateral renal agenesis, duplication of inferior venacava, high-riding aortic bifurcation and intestinal malrotation: A case report. Fertil Steril 2006. 2006;90:e9–11. doi: 10.1016/j.fertnstert.2008.05.030. [DOI] [PubMed] [Google Scholar]
- 6.Hinckley MD, Miki AA. Management of uterus didelphys, obstructed hemivagina and ipsilateral renal agenesis. A case report. J Reprod Med. 2003;48:649–51. [PubMed] [Google Scholar]
- 7.Tzialidou-Palermo I, von Kaisenberg CS, Garcia-Rocha GJ, Schloesser HW, Baehr I, Schippert C. Diagnostic challenges of hemihematocolpos and dysmenorrhea in adolescents: Obstructed hemivagina, didelphys or bicornuate uterus and renal aplasia is a rare female genital malformation. Arch Gynecol Obstet. 2012;286:785–91. doi: 10.1007/s00404-012-2392-5. [DOI] [PubMed] [Google Scholar]
- 8.El Saman AM, Shahin AY, Nasr A, Tawfik RM, Saadeldeen HS, Othman ER, et al. Hybrid septate uterus, coexistence of bicornuate and septate varieties: A genuine report. J Obstet Gynaecol Res. 2012;38:1308–14. doi: 10.1111/j.1447-0756.2012.01866.x. [DOI] [PubMed] [Google Scholar]
- 9.Ribeiro SC, Yamakami LY, Tormena RA, Pinheiro Wda S, Almeida JA, Baracat EC. Septate uterus with cervical duplication and longitudinal vaginal septum. Rev Assoc Med Bras. 2010;56:254–6. doi: 10.1590/s0104-42302010000200029. [DOI] [PubMed] [Google Scholar]
- 10.Singh N, Singh U, Verma ML. Ruptured bicornuate uterus mimicking ectopic pregnancy. A case report. J Obstet Gynaecol Res. 2013;39:364–6. doi: 10.1111/j.1447-0756.2012.01914.x. [DOI] [PubMed] [Google Scholar]
- 11.Kumar S, Singh SK, Mavuduru R, Naveen A, Agarwal MM, Vanita J, et al. Bicornuate uterine horns with complete cervical-vaginal agenesis and congenital vesicouterine fistula. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:739–41. doi: 10.1007/s00192-007-0507-5. [DOI] [PubMed] [Google Scholar]