

The American College of Radiology (ACR) Breast Imaging Reporting and DataSystem (BI-RADS®) is an international consensus document developed by ACR. It covers three imaging modalities including mammography (MG), ultrasound (US), and magnetics resonance imaging (MRI), with an attempt to promote the standardized application of breast imaging in clinical diagnosis and treatment. In 1998, based on the practices and experiences of BI-RADS MG, ACR established a Lesion Diagnosis Working Group, trying to reach consensus on morphology, dynamic enhancement, and parametric mapping and to conduct feasibility evaluation. The “dictionary” in the breast MRI report includes the minimum reporting standards on MRI scanningtechniques, lesion architecture, and region-of-interest kinetic curve acquisition, in which the lexicon used for description and diagnosis is listed. After reviewing the efficacy of the morphology and kinetic curves in differentiating the malignancy of breast lesions, the group proposed the management principles for the corresponding lesions. From 1998 to 2002, the group reviewed these lexicon again and established ACR BI-RADS®–MRI Lexicon. The continuous efforts of ACR exert guiding role in the optimization of ACR BI-RADS®–MRI Lexicon.
The content of ACR BI-RADS®–MRI Lexicon include the definitions and atlas of various morphological features, the technical requirements of breast MRI, the description of kinetic curves, and the final classification and assessment (Figure 1). It is developed to provide uniform wording for the standard breast MRI report, help clinicians to understand MRI reports and select appropriate management modes, and facilitate the communication among different research and facilities.
Figure 1.
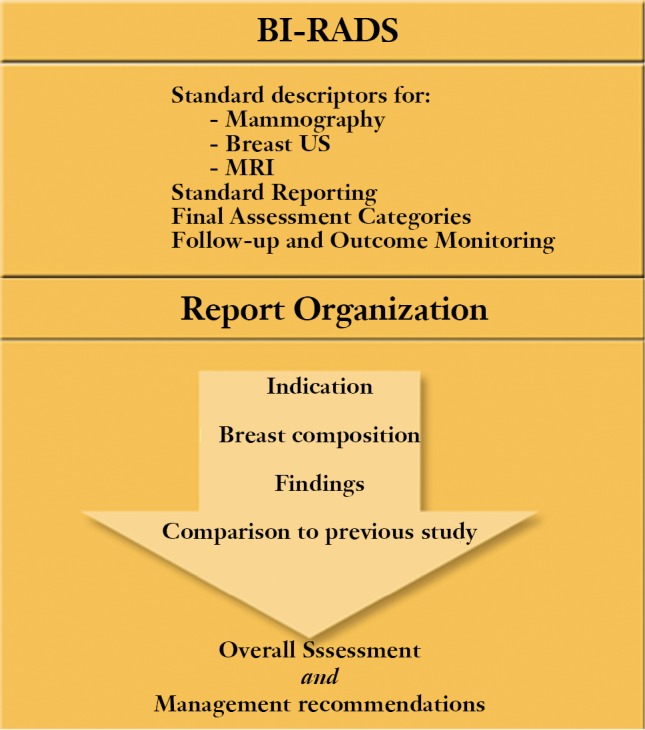
The content of ACR BI-RADS®–MRI Lexicon.
The lexicon is a basic index for breast MRI report and diagnostic description. When conducting breast MRI report discription, the basic lexicon that most meets the lesion features in the “discription” should be chosen in a logical sequence, and their meanings are basically consistent with those in the BI-RADS MG lexicon. Based on dynamic enhancement, ACR BI-RADS®–MRI Lexicon (Table 1) is especially feasible for lesions with abnormal enhancement. The lexicon recommends to carry out morphological assessment based on the images obtained at peak enhancement from high-spatial-resolution MRI (Figure 2).
Table 1. ACR BI-RADS®-MRI lexicon classification form.
| A Mass: Three-dimensional space-occupying lesion that is one process, usually round, oval,or irregular in shape. | |
|---|---|
| Shape (select one) | Description |
| ❏ Round | Spherical or ball-shaped |
| ❏ Oval | Elliptical or egg-shaped |
| ❏ Lobular | Undulating contour |
| ❏ Irregular | Uneven shape (not round, oval, or lobulated) |
| Margin (select one) | Description |
| ❏ Smooth | Well-circumscribed and well-defined margin |
| ❏ Spiculated | Characterized by radiating lines |
| ❏ Irregular | Uneven margin can be round or jagged(not smooth or spiculated) |
| Enhancement Pattern | Description |
| ❏ Homogeneous | Confluent uniform enhancement |
| ❏ Heterogeneous | Nonspecific mixed enhancement |
| ❏ Rim enhancement | Enhancement more pronounced at the periphery of mass |
| ❏ Dark internal septation | Dark nonenhancing lines within a mass |
| ❏ Enhancing internal septation | Enhancing lines within a mass |
| ❏ Central enhancement | Enhancement more pronounced at center of mass |
| B. Focus/Foci (tiny spot of enhancement, < 5 mm) if only finding, GO TO SECTION E | |
| C. Non-Mass-Like Enhancement (in an area that is not a mass) | |
| Distribution Modifiers (select one) | Description |
| ❏ Focal area | Enhancement in a confined area, less than 25% of quadrant |
| ❏ Linear | Enhancement in a line that may not conform to a duct |
| ❏ Ductal | Enhancement in a line that may have branching, conforming to a duct |
| ❏ Segmental | Triangular region of enhancement, apex pointing to nipple |
| ❏ Regional | Enhancement in a large volume of tissue not conforming to a ductal distribution, geographic |
| ❏ Multiple regions | Regional enhancement in at least two large volumes of tissue |
| ❏ Diffuse | Enhancement distributed uniformly throughout the breast |
| Distribution Modifiers (select one) | Description |
| ❏ Homogeneous | Confluent uniform enhancement |
| ❏ Heterogeneous | Nonuniform enhancement in a random pattern |
| ❏ Stippled, punctate | Enhancing foci, sand-like or dot-like |
| ❏ Clumped | Cobblestone-like enhancement, with occasional confluent areas |
| ❏ Reticular, dendritic | Enhancement with finger like projectionsextending toward nipple, especially seen on axial or sagittal images, in women with partly fatty–involuted breasts |
| D. Symmetric or Asymmetric Distribution | |
| Symmetric or Asymmetric (select one) | Description |
| ❏ Symmetric | Similar-appearing mirror-image enhancement in two breasts |
| ❏ Asymmetric | More in one breast than in the other |
| E. Other Findings (select all that apply) | |
| ❏ None apply | ❏ Edema |
| ❏ Nipple retraction | ❏ Lymphadenopathy |
| ❏ Nipple invasion | ❏ Pectoralis muscle invasion |
| E. Other Findings (select all that apply) | |
| ❏ Pre-contrast high ductal signal | ❏ Chest wall invasion |
| ❏ Skin thickening (focal) | ❏ Hematoma/blood |
| ❏ Skin invasion | ❏ Cysts |
| F. Kinetic Curve Assessment | |
| Kinetic Curve Assessment (select one) | Description |
| ❏ Initial rise | ❏ Slow |
| ❏ Medium | |
| ❏ Rapid | |
| ❏ Delayed phase | ❏ Persistent |
| ❏ Plateau | |
| ❏ Washout | |
Figure 2.

ACR BI-RADS®-MRI lexicon in breast lesion.
Notably, ACR BI-RADS MRI Lexicon can somehow be misleading or ambiguous, especially when it is translated into Chinese. The distinction between “punctuate enhancement” and “stippled enhancement” is confusing, and can be non-specific among different literature. Some literature list it as a third category after “Mass” and “Non-Mass-Like Enhancement (NMLE)”, and others regard it as a special type of NMLE. The descriptions of their imagining features are also not clear. Sometimes a same word is used for describing the different features of lesions. Particularly, the word “Irregular” is used for both the morphology and the rim of a mass, causing confusion between “irregular rim” and “irregular mass”. Therefore, it is recommended that the word “Irregular” should only be used for describing either morphology or rim, rather than both. For lesions that may be described using multiple terms, select the term that best describes the dominant lesion feature. The existence of multiple lesion features should be carefully managed because they usually can be malignant.
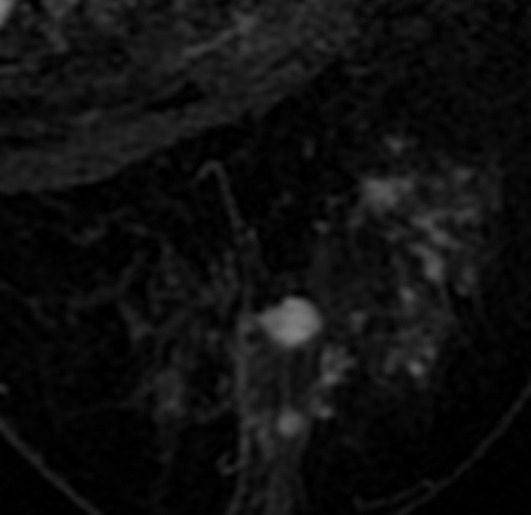
Technically, the description of a lesion needs the reconstruction/imaging from different views. For example, the linear NMLE refers to the “enhancement in a line that may not conform to aduct”; a linear enhancement at sagittal view may be shown as regional enhancement at axial or coronal view. Ductal enhancement refers to “enhancement in a line that may have branching, conforming to a duct”. The enhance can be smooth or irregular, and can be differentiated under high-resolution MRI. A segmental NMLE refers to the triangular region of enhancement, apex pointingto nipple, suggesting a duct or its branches. It is more common under thick-slice MRI. Under High-spatial-resolution thin-slice MRI, it may be shown as ductal enhancement; it may also be clumpedenhancement at the coronal plance verticle to the ducts. Unenhanced images may be applied to describe the lesions more accurately. For example, sometimes it is hard to distinguish “huge, irregular mass with heterogeneous enhancement” from “large, uneven regional enhancement”; in fact, both are used for describing large MRI enhancements. To facilitate distinction, a “mass” should have well-defined border with the surrounding breast tissues, whereas the border between a “regional enhancement” and its surrounding tissues is unclear, which can represents either lesions or normal structure, mainly depending on the internal features of the enhancement. “Stippled enhancement with a regional distribution” refers to the punctuate, mutually separated appearing enhancing foci, sand-like or dot-like, which is suggestive of the fibrocystic changes inside the breast tissue. Isolated fatty foci and non-enhanced breast tissue can be found among them. Observing the distribution features of the fat with non-enhanced T1WI may be helpful for the differentiation (Figure 3).
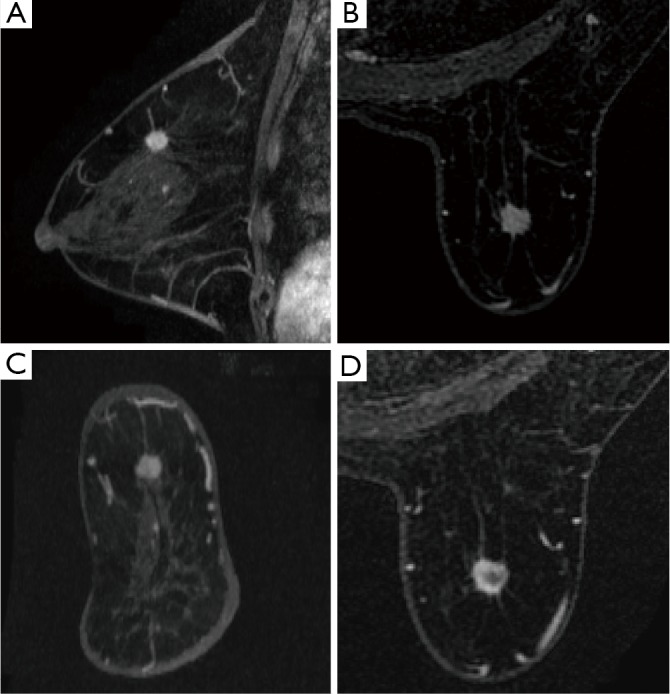
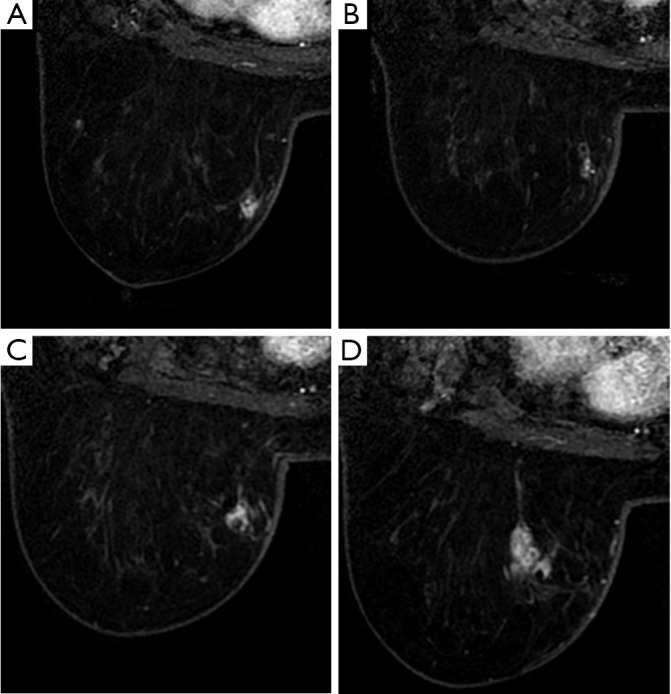
Figure 3.
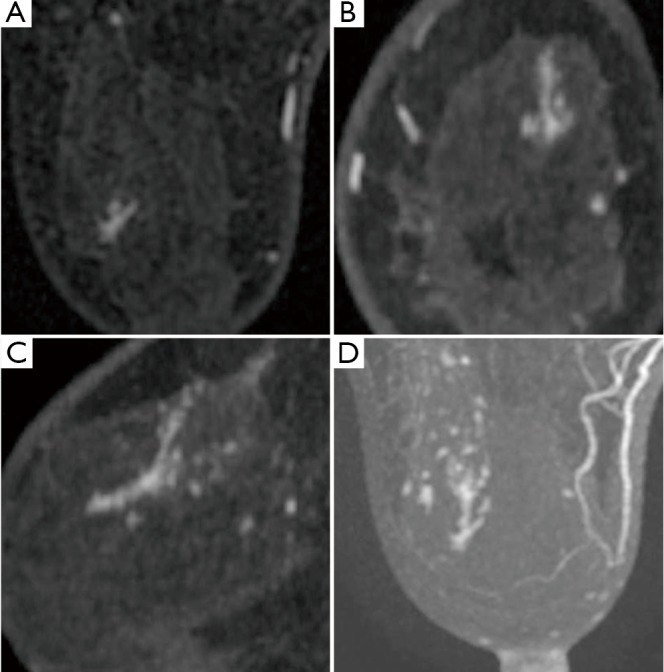
Three-dimensional morphology of a lesion. The lesion shows focal enhancement on axial view, linear enhancement on coronal view, and ductal enhancement on sagittal view. Meanwhile, it shows clumpeddistribution along the ducts. Thick-slice MIP shows ductal enhancement with clumpeddistribution. The final interpretation is “clumpedenhancement with ductal distribution”, which is suggestive of maligancy. Pathology: Ductal Carcinoma In Situ (DCIS).
A mass is a three-dimensional lesion that occupies a space within the breast. It suppresses the fibroglandular tissue in the surrounding normal breast, and an individual mass lesion usually does not contain fat or normal gland tissues.
The description of a mass should include at least three morphological characteristics: (I) shape (II) margin (III) internal enhancement pattern (Figure 4).
Figure 4.
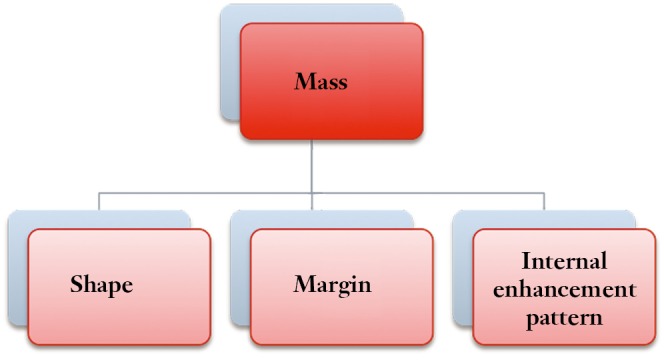
Morphological characteristics of a mass.
The interpretation of the margin and morphology of the mass should be based on the findings during the first contrast-enhanced acquisition (Arterial Phase) to avoid the interference brought by washout and progressive enhancement of the surrounding breast tissue (Figure 5).
Figure 5.
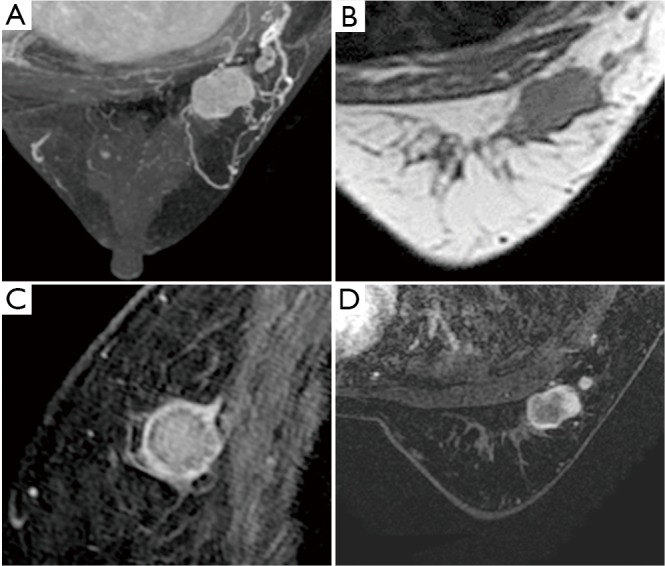
Mass features: The mass is a three-dimensional lesion that occupies a spacewithin the breast. It pushes the surrounding fat and glands, with well-defined margins. The mass exhibits a constant appearance on the MRI, without any fat or gland inside the lesion. The mass-like enhancement is described in terms of shape, margin, and internal enhancement. In this case, the mass is lobular-shaped and has smooth margin and rim enhancement. Pathology: Invasive ductal carcinoma.
Shape of the mass
The 3D geometric features of a lesion can be divided into four types: Round, oval, lobular, and irregular (Figure 6).
Figure 6.
Shape of the mass.
Round and oval: The mass can be spherical (or ball-shaped) or elliptical (or egg-shaped), which may be the morphological appearance of a mass on different cross-section. When the diameters of a mass in various directions are generally equal, it shows as round, otherwise as oval; they have no substantial difference in differentiating malignant or benign tumors. Therefore the authors name them collectively as “Oval” (Figures 7,8,9,10,11,12).
Figure 7.
Oval mass: The lesion is oval-shaped and has smooth margin and heterogeneous enhancement. Pathology: Invasive ductal carcinoma.
Figure 8.
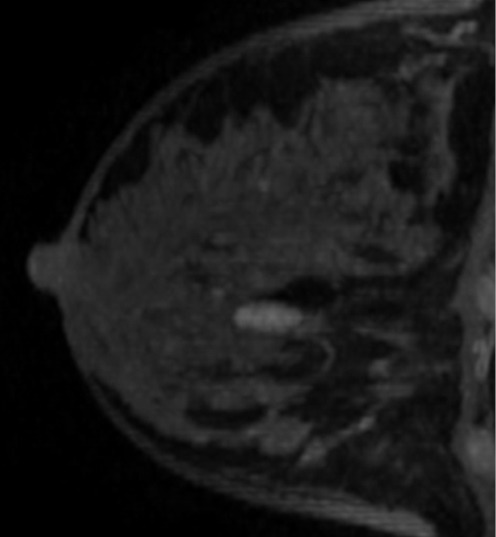
Oval mass: The mass is oval-shaped (on axial and coronal views) and has smooth margin and homogeneous internal enhancement. Pathology: Adenoma.
Figure 9.
Round mass: The lesion has nearly same diameters in all directions, with smooth margin, heterogeneous enhancement in the arterial phase, and basically homogeneous enhancement at central filling in the delay phase. Pathology: Adenoma.
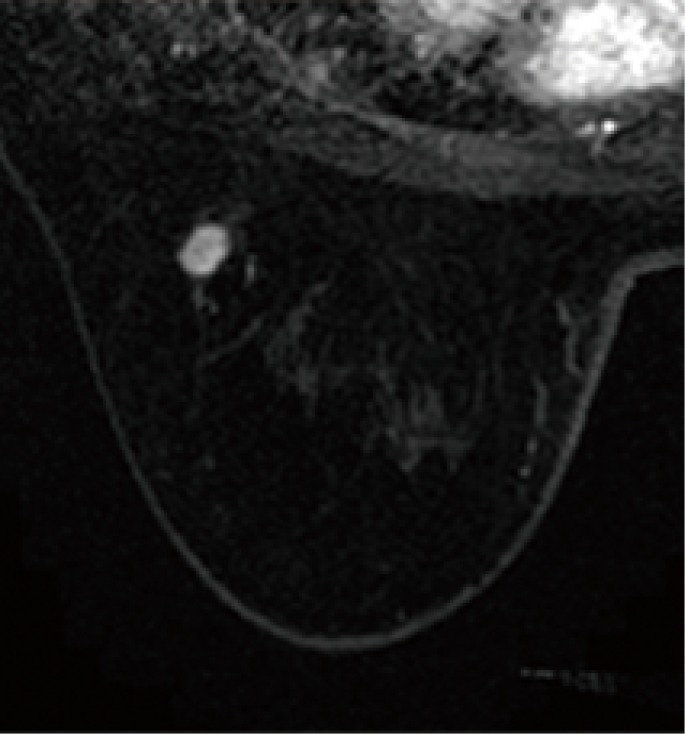
Figure 10.

Round mass: The lesion is round-shaped, without lobulation (although the margin is irregular), and without spiculation. The lesion shows mild heterogeneous enhancement during the arterial phase and increased enhancement (heterogeneous) enhancement during the delayed phase. Pathology: Fibroadenoma.
Figure 11.
Round mass: The lesion has nearly same diameters in all directions. It has smooth margin and heterogeneous internal enhancement, which shows rim enhancement. Pathology: Invasive breast carcinoma.
Figure 12.
Oval mass: The lesion shows unequal diameters in various directions. It has smooth margin and enhancing internal septation. Pathology: Invasive breast carcinoma.
The lesion is interpreted based on both morphology and margin. If the margin is irregular or with spiculation, the shape can be listed as irregular.
Lobular: A mass that has a contour with deep or shallow undulations, whose convex is not completely outward; rather, it shows scallop-like or wavy appearance (Figures 13,14,15,16).
Figure 13.
Marginal spiculae: The spherical mass has long marginal spiculae and internal homogeneous enhancement. It presents central washout during the delayed phase. Pathology: Invasive ductal carcinoma.
Figure 14.
Lobular mass: The lesion develops a mild lobulation with mild undulations. It has smooth margin and heterogeneous enhancement, with its center being unenhanced fiber components; T2WI shows low signal. Pathology: Fibroadenoma.
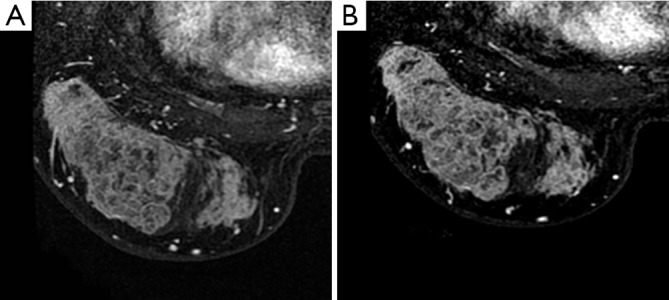
Figure 15.
Lobular mass: A huge mass in the right breast has deep lobular-shaped undulations. It has smooth margin and internal heterogeneous enhancement. Pathology: Borderline (low-grade malignant) phyllodes tumor.
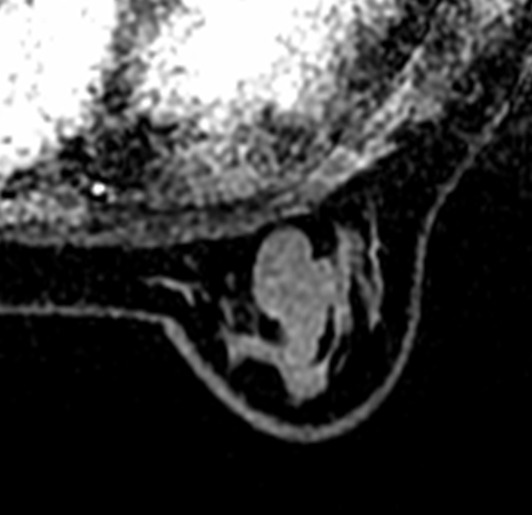
Figure 16.
Marginal spiculae: The lesion is lobular-shaped and has deep undulations. Its margin has radial protrusions, showing typical spur sign. The lesion has internal heterogeneous enhancement. The mammography shows irregular mass and burr sign. Pathology: Invasive ductal carcinoma.
Irregular: The morphology of the lesion can not be described as oval or lobular, and can not be properly described using the exact morphological terminologies. An irregular mass should be distinguished from non-mass lesions. When a non-mass lesion is relatively large, a similar visual mass effect may appear; or, a oval mass-like structure (e.g., clumped enhancement) may occur inside it. According to the authors' experiences, an “irregular” lesion is featured by the absence of fat signal inside the lesion (Figures 17,18,19,20,21).
Figure 17.
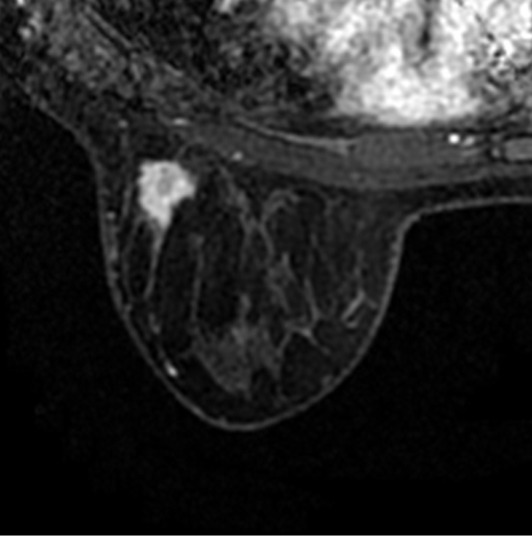
Irregular mass: The lesion has irregular shape and margin, with heterogeneous internal enhancement but without obvious spur sign. Pathology: Invasive ductal carcinoma.
Figure 18.
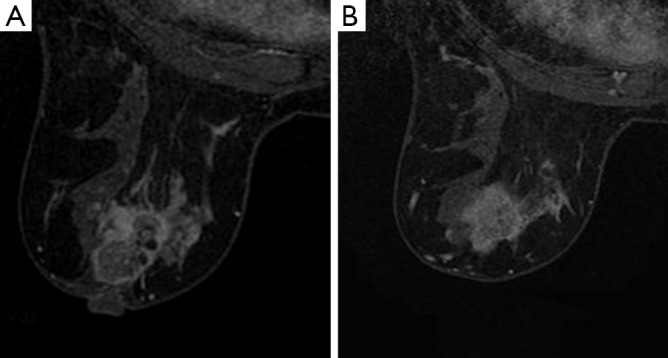
Irregular mass: The lesion has irregular morphology: Neither round nor oval; not lobular-shaped; irregular rim; heterogeneous internal enhancement, which shows rim enhancement. Pathology: Invasive ductal carcinoma.
Figure 19.
Irregular-shaped mass: The mass has a shape that is neither round nor oval; furthermore, it is not lobular. Therefore it is classified as irregular. Although another dimension of the lesion is close to round, the lesion is predominantly classified as “irregular”. It has spiculated margin and homogeneous internal enhancement. Pathology: Invasive breast carcinoma.
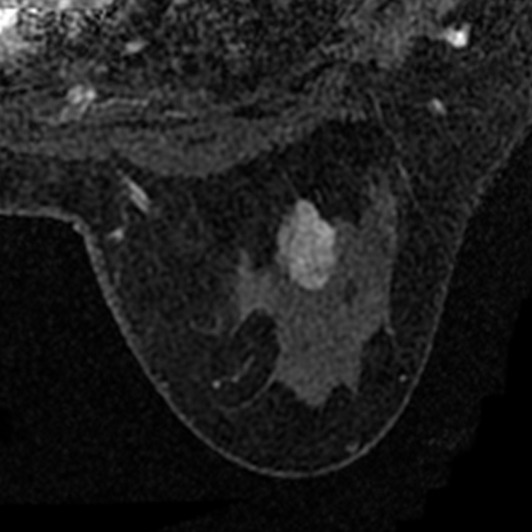
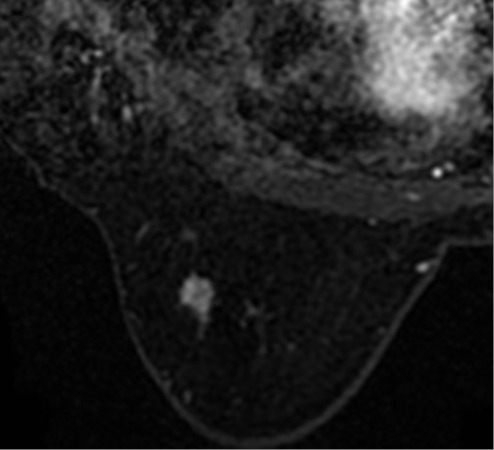
Figure 20.
Irregular mass: The lesion has irregular shape and margin and heterogeneous enhancement. Pathology: Adenosis.
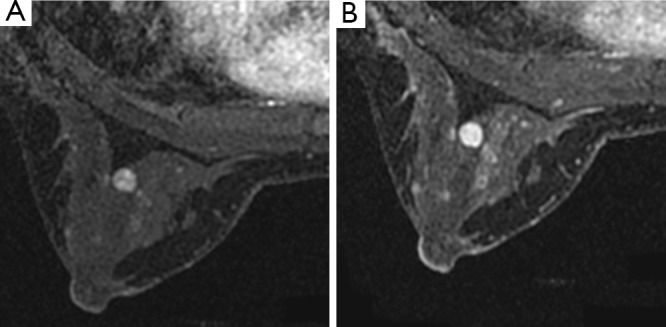
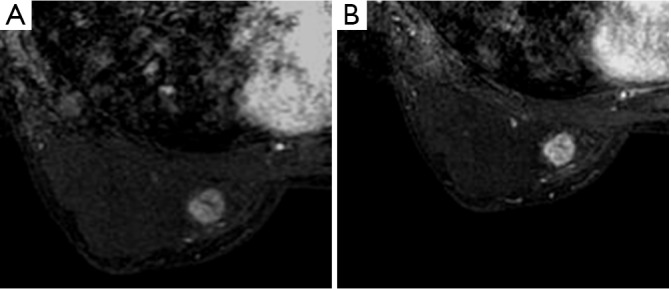
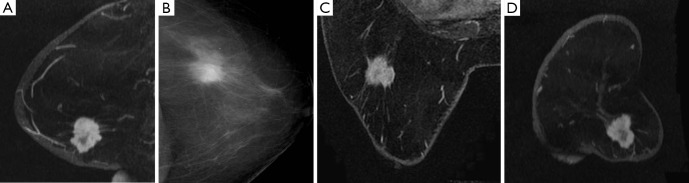
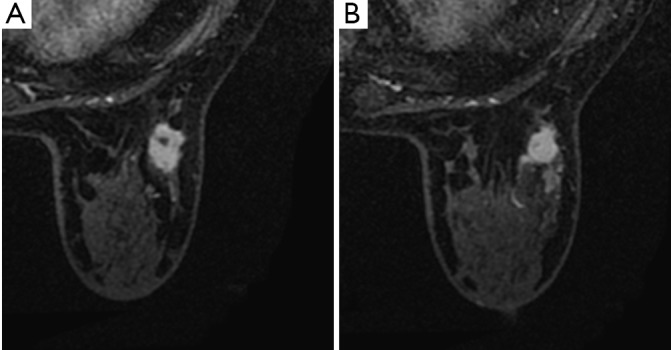
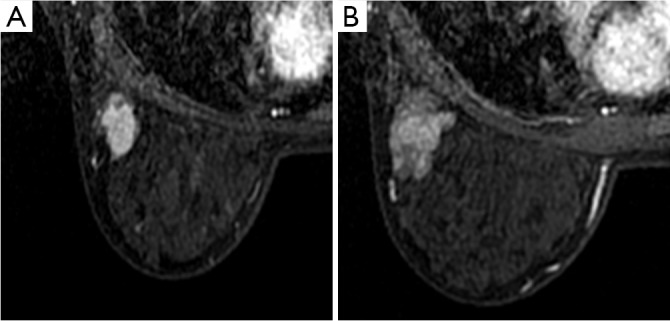
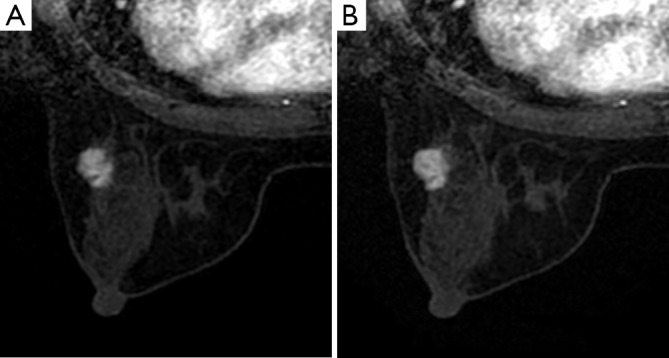
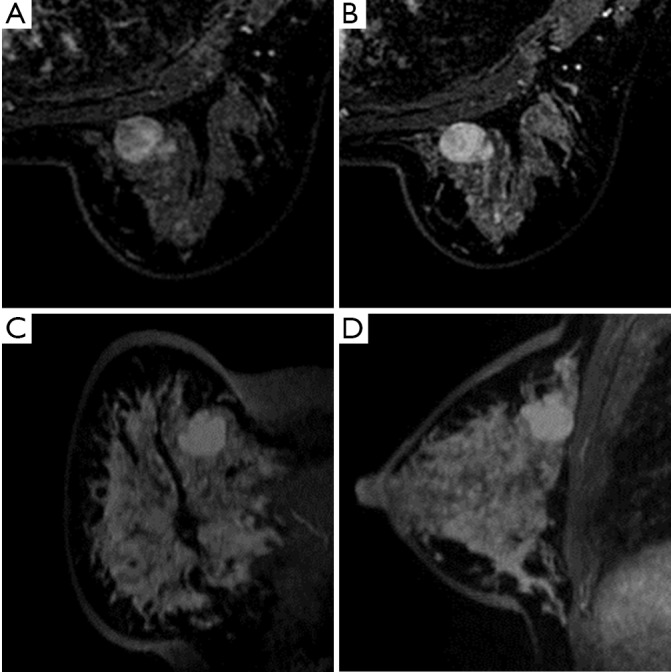
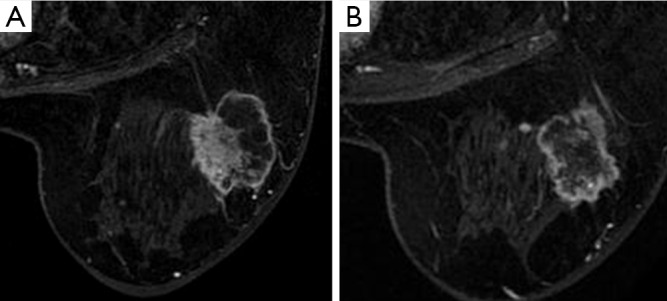
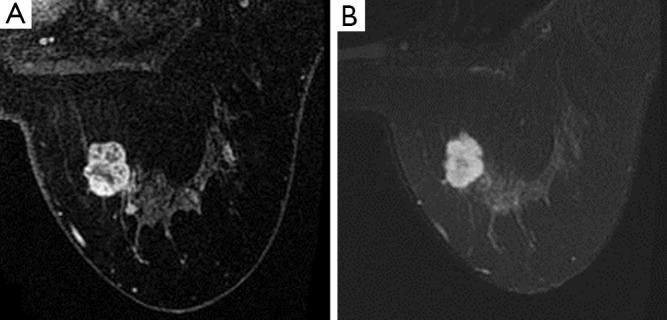
Figure 21.

Irregular mass: Multiple foci of cancer within the same breast Figure A: Irregular mass with spiculated margin and rim enhancement; Figure B: Irregular mass with irregular margin and heterogeneous enhancement. Pathology: Invasive breast carcinoma.
Margin of a mass
The margin of a lesion and its relationship with the surrounding tissues (rather than the morphology of the lesion) is emphasized. Similar to mammography, the characteristics of the margin of a mass in MRI is important for the differentiation of malignant and benign tumors. It includes three types: Smooth, spiculated and irregular (Figures 22,23,24, 25,26,27,28,29,30,31,32,33).
Figure 22.
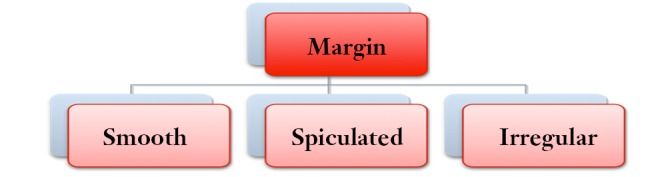
The characteristics of the margin of a mass.
Figure 23.
Smooth margin: The lesion is lobular-shaped and has smooth margin and heterogeneous internal enhancement. No spiculation is observed. Pathology: Adenoma.
Figure 24.
Smooth margin: Lobular adenoma with smooth margin and heterogeneous internal enhancement. Pathology: Sclerosing adenosis accompanied with adenoma formation. The tumor is sized 3 cm × 2 cm × 2 cm, with some of its glands becoming cancerous, which is interpreted as low-grade intraductal cancer and lobular carcinoma.
Figure 25.
Marginal spiculae: The lesion is an oval mass with spur sign (radiating line-like spinous processes) and homogeneous internal enhancement. Pathology: Invasive ductal carcinoma.
Figure 26.
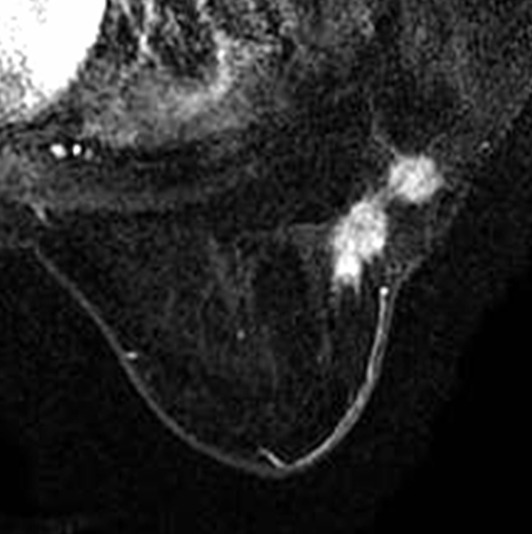
Marginal spiculae: Two oval masses with their margin covered with sharp spine-like spur. Pathology: Invasive ductal carcinoma, part of which is intraductal carcinoma.
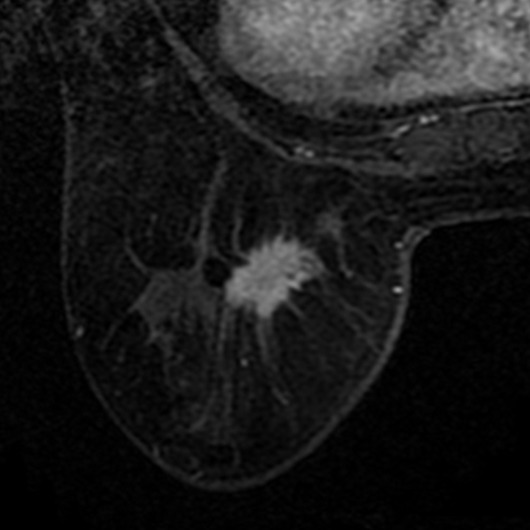
Figure 27.

Marginal spiculae: The lesion has irregular shape, with its margin covered with long, sharp spine-like processes. It has heterogeneous internal enhancement. Pathology: Invasive ductal carcinoma.
Figure 28.

Irregular margin: The mass is oval-shaped. The margin is neither smooth nor spiculated, showing irregular margin. Pathology: Invasive ductal carcinoma.
Figure 29.
Irregular margin: The lesion is round-shaped, with equal diameters in all directions. Its margin is not smooth, but also does not form spur sign, which is therefore interpreted as “irregular”. It has heterogeneous internal enhancement. Pathology: Fiber adenosis accompanied with epithelial ductal hyperplasia with a cribriform pattern.
Figure 30.
Irregular margin: The lesion has a shape of neither oval nor lobular and a margin of neither smooth nor spiculated. Therefore, it is interpreted as “irregular” in terms of both shape and margin. Pathology: Invasive ductal carcinoma.
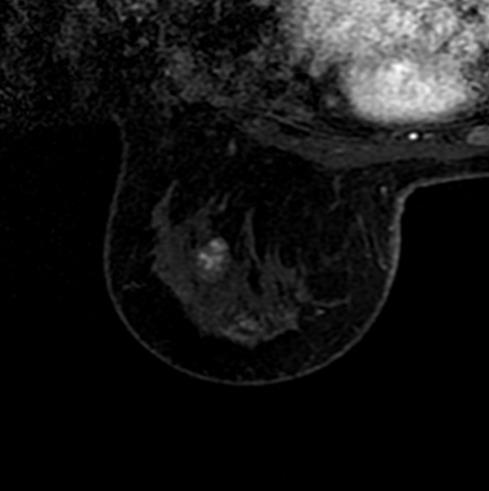
Figure 31.
Smooth margin: The lesion has smooth margin and rim enhancement.
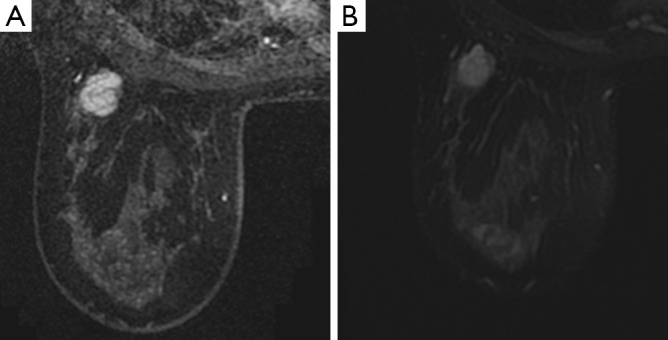
Figure 32.
Smooth margin: This is a lobular mass without enhancement during arterial phase. Pathology: Fibroadenoma.
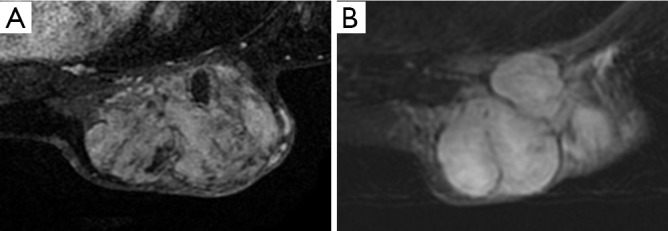
Figure 33.

Irregular mass: Both the shape and margin is irregular. Pathology: Intraductal carcinoma.
Smooth: A benign lesion usually has clear and smooth margin, which is well defined with the surrounding breast tissues. Nevertheless, not all lesions with smooth margin are begin; in fact, some malignant tumors can also have smooth margin.
Spiculated: Characterized by radiating lines.
Irregular: Uneven margin can be round or jagged (not smooth or spiculated). Genarally, masses with spiculated and irregular margin usually are malignant, whereas those with smooth margin are mostly benign. There are exceptions, though. Similar to mammography, some early breast cancer with small foci can presents benign appearance even under high-resolution MRI. The spacial resolution is extremely important in displaying the features of a mass margin, since the spiculae in some masses will not be displayed under low-resolution MRI.
Internal enhancement pattern of a mass
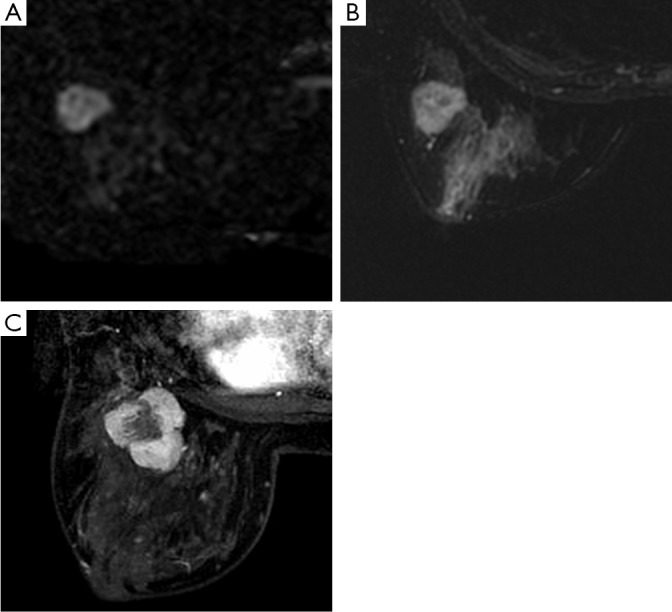
It is used to describe the consistence of the internal enhancement within a lesion in terms of scope and spacial distribution. It can be divided into six main patterns: Homogeneous enhancement, heterogeneous enhancement, rim enhancement, central enhancement, enhancing internal septations, and dark internal septations (Figures 34,35,36,37, 38,39,40,41,42,43,44,45,46,47,48,49).
Figure 34.
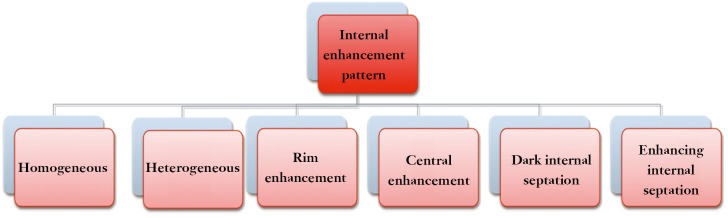
Internal enhancement pattern of a mass.
Figure 35.
Homogeneous enhancement: A irregular mass with smooth margin and homogeneous internal enhancement. Pathology: Adenoma.
Figure 36.
Homogeneous enhancement: A lobular-shaped mass with smooth margin and homogeneous, uniform, and confluent enhancement. Pathology: Invasive ductal carcinoma.
Figure 37.
Heterogeneous enhancement: The mass has heterogeneous enhancement during the arterial phase with homogeneous filling during the late phase. Interpretation is based on the appearance during the arterial phase. Lobular mass: One side of the lesion shows deep undulations and is lobular-shaped, along with smooth margin, heterogeneous enhancement during the arterial phase and homogeneous enhancement during in the late phase. Pathology: Fibroadenoma.
Figure 38.

Relativity of homogeneous enhancement: Under high-spatial-resolution MRI, some homogeneously enhancing foci may be further interpreted as heterogeneous enhancement.
Figure 39.
Heterogeneous enhancement: Irregular mass with heterogeneous internal enhancement. Pathology: Invasive ductal carcinoma.
Figure 40.
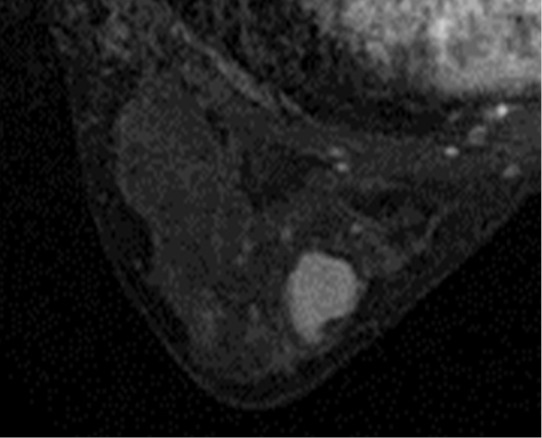
Ring enhancement: Lobular adenoma with smooth margin and rim internal enhancement. Pathology: Invasive ductal carcinoma.
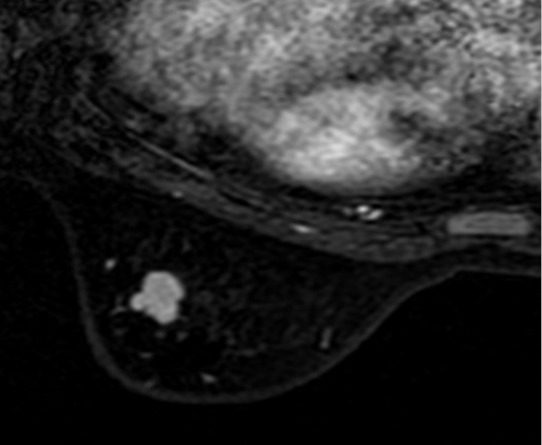
Figure 41.

Ring enhancement: Round mass with irregular margin (neither smooth nor spiculated). Pathology: Invasive ductal carcinoma.
Figure 42.
Central enhancement: Lobular mass with smooth margin. It shows enhanced processing at central than peripheral locations. Pathology: Fibroadenoma.
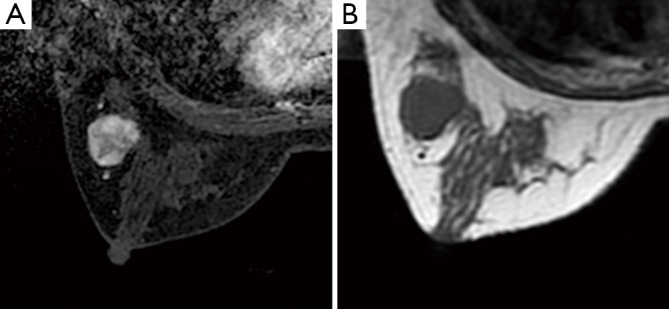
Figure 43.
Dark internal septation: An oval mass with smooth margin. Fine line-like dark internal septations can be seen, which corresponds the low signal on T2WI. Pathologically it is interpreted as fibrous septation. Pathology: Fibroadenoma.
Figure 44.

Dark internal septation: In the original 120-s arterial phase images, the lesion is shown as irregular-shaped mass with irregular margin; low-signal dark internal septation can be seen within the lesion. MIP images obtained during the delayed phase show that the lesion is fobular-shaped, with smooth margin and dark internal septations. Pathology: Fibroadenoma.
Figure 45.
Dark internal septation. T2WI shows high signal, which needs to be differentiated from adenoma. However, the high DWI signal is helpful. Pathology: Cystosarcoma phyllodes.
Figure 46.
Enhancing internal septations: Mucinous carcinoma with enhancing internal septations.
Figure 47.

Septation-like enhancement: A mass in the upper outer quadrant of the right breast shows mildly lobular enhancement during the early arterial phase and solid enhancement in the delayed phase. Pathology: Mucinous adenocarcinoma.
Figure 48.
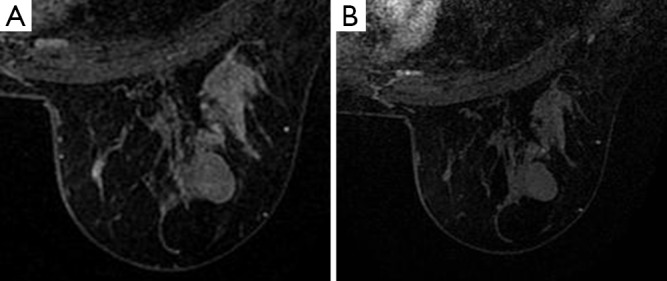
Non-enhancing mass: An oval mass with smooth margin. Compared with th breast glands, it shows no enhancement during the first phase and delayed phase. Pathology: Fibroadenoma.
Figure 49.
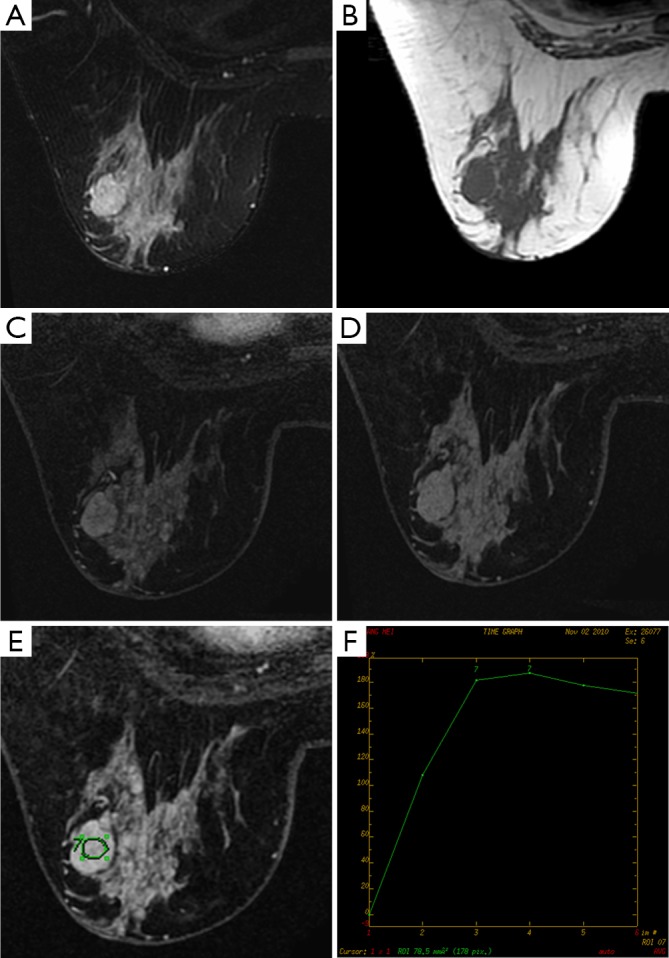
Dark internal septation. The lesion shows enhancement during the delayed phase. It has washout curve, with smooth margin. Unenhanced signals. Pathology: Fibroadenomas.
Homogeneous enhancement Homogeneous enhancement is uniform and confluent enhancement throughout the mass. The homogeneous enhancement often is suggestive of benign lesion. However, spatial resolution may limit observations on small foci. Even in a monitor with high contrast, the homogeneous enhancement is also relative.
Heterogeneous enhancement is nonuniform and unevenly-distributed enhancement, which varies at different spatial locations.
Rim enhancement is mostly suggestive of malignancy. However, benign fat necrosis can also presents rim enhancement (but with a low-signal center), which can be differentiated by mammography and medical history. This type of enhancement is also a feature of inflammatory cysts, which can be identified by its high T2 signal.
Acknowledgements
Disclosure: The authors declare no conflict of interest.