

Abstract
Background:
Test anxiety aggravates psychological distress and reduces the motivation among graduate students. This study aimed to identify psychological intervention for test anxiety, which reduces the level of psychological distress, amotivation and increases the intrinsic and extrinsic motivation among medical students.
Materials and Methods:
Westside test anxiety scale, Kessler Perceived Stress Scale and Academic Motivation Scale were used to measure test anxiety, psychological distress and motivation on 436 1st year medical students. Out of 436 students, 74 students who exhibited moderate to high test anxiety were randomly divided into either experimental or waiting list group. In this true randomized experimental study, 32 participants from the intervention group received five sessions of psychological intervention consist of psychoeducation, relaxation therapy and systematic desensitization. Thirty-three students from waiting list received one session of advice and suggestions.
Results:
After received psychological intervention participants from the intervention group experienced less anxiety, psychological distress, and amotivation (P < 0.01) and high intrinsic and extrinsic motivation (P < 0.01) in the postassessment compared with their preassessment scores.
Conclusion:
Overall psychological intervention is effective to reduce anxiety scores and its related variables.
Keywords: Anxiety, motivation, psychological distress
INTRODUCTION
Test anxiety is considered as one of the major problems among graduate students which may leads to decline in academic performance, reduces motivation and aggravates psychological distress.[1] Test anxiety is considered as normal exam worries for some students, whereas for other students it is a pathological problem as they tend to avoid exam. Test anxiety is a psychological condition in which people experience extreme distress and anxiety in testing situations.[2] Students who experience test anxiety express maladaptive thoughts such as worrying greatly about exams and exhibit negative emotion before and during an examination.[3] Various terms are similarly used for test anxiety which includes performance anxiety, examination anxiety, mathematics anxiety, sports anxiety, or fear of failure.[4] This study prefers to use the term test anxiety as this term is widely used to indicate exam anxiety. Test anxiety is a type of state anxiety where an individuals with test anxiety experience significant psychological distress only under specific situation (e.g., when taking a test, giving a class presentation, answering questions in front of others.[2]
Transition from school to medical program may create test anxiety as medical program is highly stressful and medical students are required to do lot of presentation in front of their classmates.[5,6] Test anxiety becomes a maladaptive problem when it is unmanageable and interferes with test preparation and performance.[7] Medical students generally present intense level of test anxiety specifically 1st year medical students are more susceptible for test anxiety as they are required to do lot of presentation in front of their peers in problem based learning (PBL), mock objective subjective clinical examination, demonstrate how to manage difficult clients and explain physiology and anatomy of the body in the lab.[7,8,9,10] Previous studies identified that the prevalence of test anxiety among medical students in India 6%,[11] German 29.9%,[9] Malaysia 52%,[12] and Pakistan 64%.[13] Medical students who experience test anxiety exhibited, psychological symptoms include tension, lack of concentration, worries, and stress and physical symptoms were trembling and sweeting.[12] Untreated test anxiety may leads to poor academic performance and irrational thoughts about themselves.[5] Therefore, psychological intervention is necessary for test anxiety.
Test anxiety involves many negative effect including low motivation, inadequate concentration, poor academic performance, and high distress.[14,15,16] Motivation is the inner power or internal process that energizes and directs behavior to perform certain action in order to achieve the goals.[15] Intrinsic motivation is the innate propensity to engage one's interest and to exercise one's capacity. It emerges from our psychological needs and personal curiosities. Extrinsic motivation can be obtained from the environmental incentives that will motivate a person from initiating particular action.[15] These two motivations are imperative for the attainment of high academic performance and destination. Test anxiety is significantly correlated with extrinsic and intrinsic motivation.[17,18] Test anxiety is positively correlated with demotivation.[19] Students who experience test anxiety underestimate their performance and that causes low motivation and aspiration towards studies.[20] Further, student with high test anxiety has negative belief about their performance and thus cause significant distress[21,22] identified that test anxiety and psychological distress is positively correlated. Students with high test anxiety experience more psychological stress when compared with low test anxiety.[23] Test taking anxiety can produce elevated stress and thus affect the test performance. Previous studies identified strong relationship between test anxiety, motivation and psychological distress, but have not explored provide an intervention for test anxiety reduces the psychological distress and enhances the motivation among medical students.
Previous studies[12,14] identified that test anxiety is one of the problems among medical students, which attribute for underachievement, low performance, demotivation and psychological distress, but it can be managed by appropriate psychological intervention. Lack of insight about test anxiety attributes not to take treatment for their test anxiety. Previous studies used cognitive behavior therapy,[24] systematic desensitization,[25] behavioral activation,[26] progressive muscle relaxation,[26,27] and psychoeducation[26] to reduce test anxiety. Students are more likely unwilling to come for long-term therapy and also psychological treatment, which requires more attention. Students are more likely willing to attend brief intervention and intervention which is easy to implement to handle their test anxiety. This study aims to use psychoeducation, progressive muscular relaxation therapy (PMRT) and systematic desensitization as these techniques were individually and widely been used by previous researchers to treat anxiety, but not on these combination (psychoeducation, PMRT and systematic desensitization) to reduce test anxiety. This study prefers to use the combination of three psychological interventions for test anxiety to evaluate whether test anxiety management reduces the amotivation and psychological distress. Moreover, previous studies have not identified whether anxiety management which includes psychoeducation, relaxation therapy and systematic desensitization for test anxiety reduces psychological distress and increase the motivation among medical students in Malaysia and overseas. Based upon these previous findings this study aims to:
Identify the prevalence of test anxiety among undergraduate medical students
Whether psychological intervention for anxiety reduces the level of test anxiety, psychological distress, amotivation and increases the intrinsic and extrinsic motivation among medical students.
MATERIALS AND METHODS
Study design and participants
This is a randomized experimental study, which has been approved by one of the private university in Malaysia in 2013. The target participants were 436 first semester undergraduate medical students from one of the private universities in Malaysia. Out of these 436 participants 74 students who exhibited moderate to high anxiety score in Westside test anxiety scale (WTAS)[28] in the preliminary assessment were randomly divided into either intervention or waiting group. Thirty-two students fully participated in intervention group and 33 participated in waiting list group. The mean age of the participants was 19 (1.04). There were 12 male and 20 female in the intervention group and 13 male and 21 female were participated in the waiting list. The participants who fulfilled their first 5 weeks in their medical program and exhibited moderate to high anxiety score ranges from 30 to 39 in the WTAS were included in this study. The participants who exhibited above the score 40 in WTAS were excluded as they experienced extremely higher level of test anxiety and they were referred to student counselor. Participants who were willing to participate in this study were given written consent before they fill the questionnaires and participate in the intervention.
Measures
Socio demographic information
This scale is prepared for this study purpose to collect data on gender, age, marital status, employment status and ethnicity.
Westside test anxiety scale[28]
This scale was used to measure anxiety toward exam. It contains 10 items, which are in a five-point scale ranging from 1 - not at all true to 5 - extremely true. Total score ranges from 10 to 50. According to Driscoll,[28] the score ranges from 10 to 29 considered to be normal test anxiety, 30-34 moderate test anxiety, 35-39 high test anxiety and 40-50 extremely high test anxiety. The scale has been found to be a sensitive measure of impairment, with an attained r = 0.44 correlation between changes in anxiety as measured by the scale and changes in test scores over time.[28]
The Kessler perceived distress scale (K-10)[29]
It consists of ten items and measured in five points Likert scale. K-10 has a cut-off score of below 20 indicates no psychological distress while score of 21-50 is considered as psychological distress. The validity alpha 0.95.[30]
Academic motivation scale (AMS)
This scale was used for measuring intrinsic, extrinsic and amotivation. It consisted of 28 items and each item is scored in seven point Likert scale. Higher score indicates higher strength of motivation. It is an overall estimate scale by summing items comprising of three constructs included intrinsic motivation, intrinsic, and amotivation. AMS concludes motivation level by covering intrinsic motivation with 12 items, another 12 items on extrinsic motivation and four items on amotivation. This scale alpha value ranges from 0.71 to 0.83.[31]
Procedures
After obtaining ethical and research approval from the university where this study was conducted, the researchers of this study approached the medical students towards conclusion of one of their lectures from week 5-7 to participate in this study. After described the aim of this study, written consent were received from the participants who were willing to participate in this study. Therapist invited one of the staff member (statistician) from their faculty to random the number of participants who exhibited moderate to high anxiety score in WTAS. Four students from intervention group and three from waiting list were unwilling to participate in this study intervention part. Overall, 33 participants were willing to participate in intervention group and 34 in waiting list. One student declined in mid of intervention from the intervention group. Similarly, one student from waiting list was unwilling to participate in the postassessment. Thirty-two students from intervention group received five sessions of psychological intervention to reduce their test anxiety for a period of 3 weeks. Simultaneously, 33 students from the waiting group received one session of advice and suggestion to manage test anxiety.
In this experimental design participants received their preassessment consists of WTAS, K-10 and AMS. The first author of this study is a clinical psychologist who offered the psychological intervention for the intervention group participants. Co-author of this study offered advice and suggestion to the waiting list participants. All these intervention were offered before their first semester exam and these participants were received their postassessment consists of WTAS, K-10 and AMS before a week of their second semester exam. Waiting list participants were received full intervention as like as intervention group participants after their postassessment.
This study intervention covers psychoeducation, PMRT and systematic desensitization. First session focused on explaining the scores of test anxiety, psychological distress and subscales of motivation. Subsequently, therapist explained about psychological intervention and rules and regulation of intervention sessions. Session two focused on psychoeducation and PMRT. Counseling was focused towards psychological and physical symptoms of test anxiety and the consequences of test anxiety such as low marks, pessimistic thoughts about themselves and scholastic performance. Subsequently, therapist taught the short version of PMRT. Participants were provided CD of PMRT and advised to practice the PMRT twice daily until come for next session. Therapist counseled participants to write the hierarchy of least to most anxiety provoking situation related to test anxiety. Participants were counseled to rate the level of anxiety from 0 to 100 for each items in the list and also counseled to describe the feelings and emotions related with each item in the anxiety provoking list.
Session three focused on systematic desensitization. Therapist went through the item related with the anxiety producing situation from the test anxiety hierarchy and also discussed with participants to rate the least to higher level of anxiety. Participants were advised to practice the relaxation therapy and slowly imagine the least level of anxiety producing situation in the test anxiety hierarchy. If participants felt tension and anxiety, they were advised to stop and return to relaxation technique until they were comfortable. Once again, when they reached the relax mood, they were counseled to continue to imagine the anxiety producing situation. Homework was given to continue their PMRT.
Session four also focused on systematic desensitization like session three. Session five was provided for the participants who needed additional sessions to cover their anxiety situation from test anxiety hierarchy.
Waiting list participants were advised to plan their time management and use effective study skill techniques. They were also advised to use breathing techniques to relax their anxiety before exam.
Statistical analysis
Descriptive statistics was used to find out the prevalence of test anxiety. Paired t-test was used to find out the significant difference within pre and postassessment scores. Independent t-test was used to find out significant differences between experimental and waiting list group scores.
RESULTS
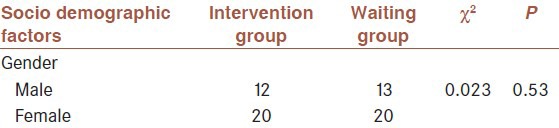
Table 1 shows the demographic characteristics of the participants participated in experimental and waiting group are similar (P > 0.05). All the participants participated in this study were unmarried and unemployed.
Table 1.
Socio demographic characteristics of participants
Prevalence of test anxiety
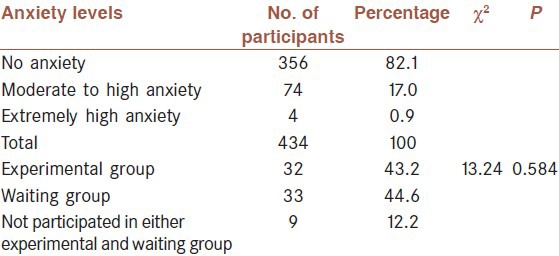
The prevalence and percentage of test anxiety among the sample is shown in Table 2. Out of 436 participants 358 (82.1%) did not experience test anxiety during this study assessment while, 74 (17.0%) experienced moderate to high test anxiety. Both the experimental and waiting group participants’ anxiety levels are similar (P > 0.05).
Table 2.
Prevalence of anxiety between experimental and waiting group
Difference in the scores of test anxiety between and within group of participants
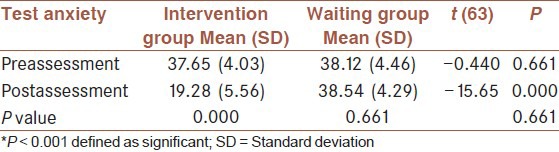
Table 3 shows significant difference between intervention and waiting list participants scores of test anxiety in postassessment (t(63) = −15.65, P = 0.000, d = −3.87). The Cohen's effect size value (d = 0.3.87) suggested a high practical significance between intervention and waiting list participants postassessment scores of test anxiety. Further, there is a significant difference exist within intervention group participants pre and postassessment scores of test anxiety (P = 0.000).
Table 3.
Differences in test anxiety between and within group
Difference between and within groups of participants scores in subscales of motivation
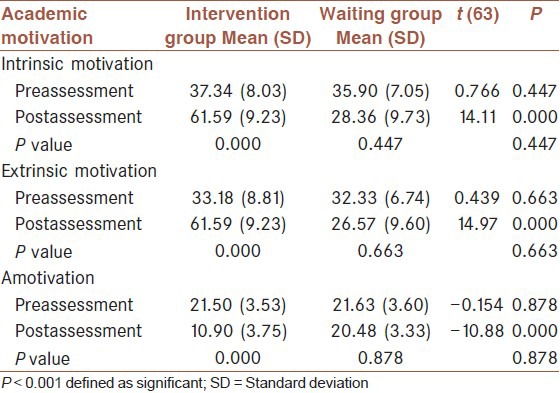
Table 4 shows that there is a significant difference between intervention and waiting list participants scores of intrinsic motivation (t(63) = 14.11, P = 0.000, d = 3.50), extrinsic motivation (t(63) = 14.97, P = 0.000, d = 3.71) demotivation (t(63) = −10.88, P = 0.000, d = −2.70). The Cohen's effect size value showed high practical significance between intervention and waiting list participants postassessment scores in the subscales of academic motivation. Further, there is a significant difference exist within intervention group participants pre- and post-assessment scores of motivation (intrinsic, extrinsic and amotivation) (P = 0.000).
Table 4.
Differences in academic motivation scores between and within group
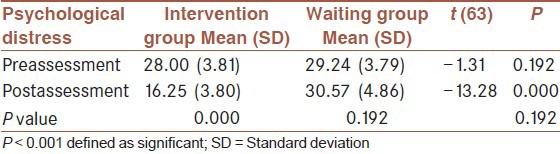
Difference in the scores of psychological distress between and within group of participants’
The result from Table 5 depicts there is a significant difference between intervention and waiting list participants scores of psychological distress (t(63) = −13.28, P = 0.000, d = −3.28). The Cohen's effect size value showed high practical significance between intervention and waiting list participants postassessment scores of psychological distress. Further, there is a significant difference exist within intervention group participants pre- and post-assessment scores of psychological distress (P = 0.000).
Table 5.
Differences in psychological distress between and within group
DISCUSSION
International researchers have identified medical students experience test anxiety and untreated test anxiety leads to poor academic performance, low motivation and psychological distress. Current research investigated the effectiveness of psychological intervention for test anxiety to reduce psychological distress and increase the motivation among medical students in one of the private universities in Malaysia.
The prevalence of test anxiety among the sample of medical students in the present study was 18%. This study prevalence is lower than was found in a study of medical students attending in German 29.9%,[9] Iran 40.3%,[8] Malaysia 52%,[12] and Pakistan 64%[13] and higher than Taiwan 7.0,[6] India 6%.[11] The prevalence of test anxiety is lesser compared to previous study in Malaysia as participants of this study entered into medical program with high entry requirements and prospective medical students are interviewed professionally to measure their psychological well-being and competency to handle crisis situation. Further, students join in this university medical program are aware that university expects high performance in their medical program as this university has 36 partner schools from all over the world. Thus, create awareness among students to enhance their self-confidence to face the challenges in the medical program. Whereas, this study prevalence of test anxiety is higher compare with medical students from Taiwan and India. It is because[13] medical students were expected to do various presentations in front of their fellow mates in their 1st year which contribute for higher anxiety among 1st year students.
Many researchers suggest that a little worry about exam is good for students because it keeps them task oriented; however unmanageable excessive exam worry on the other hand can be very debilitating and interferes with the exam performance and results.[5,12] The first hypothesis of this study was achieved as the result of this study showed that students who participated in this study intervention group exhibited significant reduction in their scores of test anxiety in the postassessment compared with postassessment scores of waiting list students. Previous studies had also found similar results that students who received anxiety intervention includes relaxation therapy,[24,27] psychoeducation[26] and systematic desensitization[26] manifest low scores in their postassessment compared with students who did not receive intervention. Further, untreated test anxiety leads to surge of test anxiety as participants in waiting list exhibited high anxiety scores in the postassessment compare with their preassessment scores of test anxiety. In addition,[5,32] identified that relentless test anxiety more likely leads to poor academic performance, lack of motivation, excessive distress and negative perception about the skill and program there are pursuing. Therefore, providing intervention at the first semester would be beneficial for the students to overcome their test anxiety at the early stage.
Previous studies[14,32] identified that students who experience test anxiety are less motivated, manifest poor academic performance and reluctant to clarify their doubts with lecturers in class room setting. The second hypothesis of this study were achieved as the results of this study showed that students who received test anxiety intervention manifest increased scores of intrinsic and extrinsic motivation compared with students who did not receive interventions. Students’ negative perceptions about their academic performance were associated with intrinsic and extrinsic motivations.[23] Students experience test anxiety perceives negatively about their academic performance and thus reduces their motivation and increases their psychological distress. Hence, provide intervention for test anxiety is beneficial for the students to increase the intrinsic and extrinsic motivation and reduced a motivation. Previous studies[33] used psychological intervention to enhance student motivation, but when students experience test anxiety their demotivation becomes excessive. Therefore, test anxiety has to be treated as it is an aggravating factor for demotivation and low intrinsic and extrinsic motivation.
The third hypothesis of this study were achieved as the results of this study showed that students who received test anxiety intervention manifest reduced scores of psychological distress compared with students who did not receive intervention. Previous studies identified that psychoducation[34] and relaxation therapy[22] was useful to reduce psychological distress but test anxiety is an aggravating factor for psychological distress[16] and intervention has to be given for test anxiety as test anxiety person perceives their performance negatively and highly distressed before the exam.[11] Providing psychoeducation is useful for students understand the relationship between negative thoughts about exam and its related psychosomatic symptoms and also the consequences of test anxiety. Further, systematic desensitization intervention is useful to desensitize their worries and tension related to test anxiety beneficial for students to overcome and manage their test anxiety. If the anxiety is not treated at the first semester, these students may continue to show low academic performance which causes them to discontinue the medical program. Overall anxiety intervention for test anxiety reduced the psychological distress and enhanced the motivation.
One of the major practical implication of this study is students are more likely to use this study anxiety management techniques as it is a brief psychological intervention and easy to understand and implement to handle their test anxiety. This study used individual counseling as students are more likely willing to receive individual counseling rather than group counseling because in group counseling students need to share their grievances in front of their fellow mates which may embarrass them and they may feel anxious that their group members will come to know about their problems. One of the research studies identified that medical student were least bothered about the mental status and one in every five students strongly conceal their emotional problems.[35] Universities have to provide insight about the sequel of test anxiety and availability of psychological services in the university during orientation day. Students who experience test anxiety are more likely experience performance anxiety in other activities such as PBL, mock objective subjective clinical examination (OSCE) and medical lab.[5]
Limitation of this study is this study focused only on 1st year students as they are more vulnerable for test anxiety. However, the senior students also most likely experience test anxiety and this study did not explore the senior students test anxiety, their motivation and psychological distress. This study focused only on medical students and did not explore other health sciences students test anxiety.
Overall psychoeducation and systematic desensitization are effective to reduce test anxiety, psychological distress and enhance academic motivation. Provide intervention for test anxiety more likely influence students to manage their performance anxiety related to PBL, mock OSCE and medical lab. Student counselors and other mental health professionals can also use this study psychological intervention technique to provide intervention for test anxiety for their students.
AUTHORS CONTRIBUTION
First author provided psychological intervention and second author collected and analysed data. Both authors substantially contributed for designing this study research, interpreting the data, drafting and reviewing the manuscript, and provide approval for the revised version of the manuscript.
ACKNOWLEDGMENT
The authors are grateful to the medical students who participated in this study. The authors thankful to the university, which offered the permission to conduct this study (B01/10-Res (20) 2013).
Footnotes
Source of Support: This research was funded by International Medical University, Malaysia
Conflict of Interest: None declared.
REFERENCES
- 1.Rafiq R, Ghazal S, Farooqi YN. Test anxiety in students: Semester's vs. annual system. J Behav Sci. 2007;17:79–95. [Google Scholar]
- 2.Cherry K. What is test anxiety? About com. [Last accessed on 2013 October 12]. Available from: http://www.psychology.about.com/od/mentalhealth/a/test-anxiety.html .
- 3.Akca F. The relationship between test anxiety and learned helplessness. Soc Behav Pers. 2011;39:101–12. [Google Scholar]
- 4.Stober J, Pekrun R. Advances in test anxiety research. Anxiety Stress Coping. 2004;3:205–11. [Google Scholar]
- 5.Chandavarkar U, Azzam A, Mathews CA. Anxiety symptoms and perceived performance in medical students. Depress Anxiety. 2007;24:103–11. doi: 10.1002/da.20185. [DOI] [PubMed] [Google Scholar]
- 6.Chen CS, Lai CS, Lu PY, Tsai JC, Chiang HC, Huang IT, et al. Performance anxiety at English PBL groups among Taiwanese medical students: A preliminary study. Kaohsiung J Med Sci. 2008;24:S54–8. doi: 10.1016/S1607-551X(08)70095-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Latas M, Pantić M, Obradović D. Analysis of test anxiety in medical students. Med Pregl. 2010;63:863–6. doi: 10.2298/mpns1012863l. [DOI] [PubMed] [Google Scholar]
- 8.Miri HR, Piroozan A, Hesam AA, Naderi N, Rezaei P. Determining the level of test anxiety and some of its contributing factors among the freshmen students. Life Sci. 2013;10:149–55. [Google Scholar]
- 9.Tektaş OY, Paulsen F, Sel S. Test anxiety among German medical students and its impact on lifestyle and substance abuse. Med Teach. 2013;35:969. doi: 10.3109/0142159X.2013.786813. [DOI] [PubMed] [Google Scholar]
- 10.Yousefi F, Habibi S, Mohammadkhani M. Test anxiety level in medical students and its relationship with sexuality. Q Educ Strateg Med Sci. 2013;6:141–5. [Google Scholar]
- 11.Pahwa B, Goyal S, Srivastava K, Saldanha D, Bhattacharya D. A study of exam related anxiety amongst medical students. Indian J Psychiatry. 2008;18:46–58. [Google Scholar]
- 12.Ping LT, Subramaniam K, Krishnaswamy S. Test anxiety: State, trait and relationship with exam satisfaction. Malays J Med Sci. 2008;15:18–23. [PMC free article] [PubMed] [Google Scholar]
- 13.Hashmat S, Hashmat M, Amanullah F, Aziz S. Factors causing exam anxiety in medical students. J Pak Med Assoc. 2008;58:167–70. [PubMed] [Google Scholar]
- 14.Rana RA, Mahmood N. The relationship between test anxiety and academic achievement. Bull Educ Res. 2010;32:63–74. [Google Scholar]
- 15.Ryan RM, Deci EL. Intrinsic and extrinsic motivations: Classic definitions and new directions. Contemp Educ Psychol. 2000;25:54–67. doi: 10.1006/ceps.1999.1020. [DOI] [PubMed] [Google Scholar]
- 16.Sena JD, Lowe PA, Lee SW. Significant predictors of test anxiety among students with and without learning disabilities. J Learn Disabil. 2007;40:360–76. doi: 10.1177/00222194070400040601. [DOI] [PubMed] [Google Scholar]
- 17.Harpell JV, Andrews JW. Relationship between schools based stress and test anxiety. Int J Psychol Stud. 2013;5:74–84. [Google Scholar]
- 18.Masson AM, Hoyois P, Cadot M, Nahama V, Petit F, Ansseau M. Girls are more successful than boys at the university. Gender group differences in models integrating motivational and aggressive components correlated with Test-Anxiety. Encephale. 2004;30:1–15. doi: 10.1016/s0013-7006(04)95410-3. [DOI] [PubMed] [Google Scholar]
- 19.Rastegar M, Akbarzadeh M, Heidari N. The darker side of motivation: Demotivation and its relation with two variables of anxiety among Iranian learners. ISRN Educ. 2012:1–8. [Google Scholar]
- 20.Urhahne D, Chao SH, Florineth ML, Luttenberger S, Paechter M. Academic self-concept, learning motivation, and test anxiety of the underestimated student. Br J Educ Psychol. 2011;81:161–77. doi: 10.1348/000709910X504500. [DOI] [PubMed] [Google Scholar]
- 21.Cassady JC, Johnson RE. Cognitive test anxiety and academic performance. Contemp Educ Psychol. 2002;27:270–95. [Google Scholar]
- 22.Akinsola EF, Nwajei AD. Test anxiety, depression and academic performance: Assessment and management using relaxation and cognitive restructuring techniques. Psychology. 2013;4:18–24. [Google Scholar]
- 23.Ahn D, Park G, Baek KJ, Chung SI. Academic motivation, academic stress, and perceptions of academic performance in medical students. Korean J Med Educ. 2007;19:59–71. [Google Scholar]
- 24.Arefi M, Momeni K, Mohsenzadeh F. The effect of cognitive and relaxation therapy on student's test anxiety. J Kerman Univ Med Sci. 2012;16:125–31. [Google Scholar]
- 25.Ali FA, Seyed HS, Fatemeh E. Test-anxiety in Iranian students: Cognitive therapy vs. systematic desensitisation. Arch Med Sci. 2006;2:199–204. [Google Scholar]
- 26.Powell DH. Behavioral treatment of debilitating test anxiety among medical students. J Clin Psychol. 2004;60:853–65. doi: 10.1002/jclp.20043. [DOI] [PubMed] [Google Scholar]
- 27.Vitasari P, Wahab MN, Othman A, Awang MG. The use of study anxiety intervention in reducing anxiety to improve academic performance among university students. Int J Psychol Stud. 2010;2:89–95. [Google Scholar]
- 28.Driscoll R. Westside test anxiety scale validation. Education Resources Information Center. 2007:6. [Google Scholar]
- 29.Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normand SL, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32:959–76. doi: 10.1017/s0033291702006074. [DOI] [PubMed] [Google Scholar]
- 30.Arnaud B, Malet L, Teissedre F, Izaute M, Moustafa F, Geneste J, et al. Validity study of Kessler's psychological distress scales conducted among patients admitted to French emergency department for alcohol consumption-related disorders. Alcohol Clin Exp Res. 2010;34:1235–45. doi: 10.1111/j.1530-0277.2010.01201.x. [DOI] [PubMed] [Google Scholar]
- 31.Vallerand RJ, Pelletier LG, Blais MR, Brière NM, Senécal C, Vallières EF. On the assessment of intrinsic, extrinsic and amotivation in education: Evidence on the concurrent and construct validity of the academic motivation scale. Educ Psychol Meas. 1993;53:159–72. [Google Scholar]
- 32.Hancock DR. Effects of test anxiety and evaluative threat on students’ achievement and motivation. J Educ Res. 2001;94:284–90. [Google Scholar]
- 33.Wigfield A, Wentzel KR. Introduction to motivation at school: Interventions that work. Educ Psychol. 2007;42:191–6. [Google Scholar]
- 34.Donker T, Griffiths KM, Cuijpers P, Christensen H. Psychoeducation for depression, anxiety and psychological distress: A v. BMC Med. 2009;7:79. doi: 10.1186/1741-7015-7-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Walter G, Soh NL, Norgren Jaconelli S, Lampe L, Malhi GS, Hunt G. Medical students’ subjective ratings of stress levels and awareness of student support services about mental health. Postgrad Med J. 2013;89:311–5. doi: 10.1136/postgradmedj-2012-131343. [DOI] [PubMed] [Google Scholar]