

Abstract
Background:
Due to the wholesome benefits of nuts increased consumption of them has been recommended. However, because of nut's high energy density, the role of them in the treatment of overweight and obesity is vague. This current clinical trial study aims to investigate the effects of a balanced hypocaloric almond-enriched diet (AED) (almond group) in comparison to a balanced hypocaloric nut-free diet (NFD) (nut-free group) on body weight and cardiovascular disease risk factors in women with body mass index (BMI) >25 for 3-month.
Materials and Methods:
A total of 108 overweight and obese women were assigned in our 3-month randomized controlled trial. The subjects were randomly divided into two groups regarding a balanced hypocaloric diet with or without almond. The planned reduced calorie diets for both groups were identical except for the almond group who consumed 50 g of almonds daily. Anthropometric and laboratory measurements of the participants who completed the study were made prior to and at the end of the study.
Results:
A total of 100 subjects completed the study. Weight, BMI, waist circumference, waist to hip circumference ratio, total cholesterol, and triglyceride, total: High density lipoprotein-cholesterol (HDL-C), fasting blood sugar and diastolic blood pressure decreased significantly in the almond group compared to the nut-free group (P > 0.001). Greater reduction in low density lipoprotein-cholesterol (P > 0.002) and systolic blood pressure (P > 0.001) and greater increase in HDL-C (P = 0.001) were found in the nut-free group.
Conclusion:
The balanced hypocaloric AED in comparison to the balanced hypocaloric NFD led to a greater weight-loss and overall better improvements in studied cardiovascular disease risk factors.
Keywords: Almond, blood glucose, caloric restriction, lipids, nuts, obesity, overweight, weight-loss, weight reduction program
INTRODUCTION
In recent decades, overweight and obesity have become the major public health concerns. Population health statistics shows that obesity in most of the industrial countries such as the United Kingdom, Australia, and the United States have been increasing.[1]
Energy balance equations indicate that weight gain can occur when there is a prolonged persistence of energy imbalance between energy intake and energy expenditure. In recent years, increase in the prevalence of overweight and obesity is significant in both developed and developing countries; it shows that the origin of this public health problem is complicated and multifactorial.[2,3] Sedentary lifestyle, macronutrient composition of the diet and increased energy density of foods are some factors that may contribute to the growth of obesity in the world.[4] The cause of many diseases such as diabetes mellitus, cancer, coronary heart disease, and sleep-breathing disorders are obesity.[5]
Currently, there is no single dietary or lifestyle intervention that is effective in reducing weight for a prolonged period. Traditional prescriptions for weight-loss decrease total fat and so often restrict nut consumption.[6] Nuts are rich in many vitamins, minerals, monounsaturated and polyunsaturated fatty acids.[7] Because of nut's usefulness's regular consumption of them has been recommended as a part of a wholesome diet.[8]
Nut consumption (such as almond) cause improvements in triglycerides, total cholesterol (TC),[9] and low density lipoprotein-cholesterol (LDL-C) and so it has positive effects on various cardiovascular disease risk factors.[9,10,11] Moreover, observational studies show that nut consumption is associated with a lower risk of developing coronary artery disease, hypertension, and type 2 diabetes.[12,13,14] It has been known that fiber and protein[15] are known factors of increase of the satiety of meals and prolong feelings of fullness;[16] moreover, nuts are also a dietary source of them[15] and almonds also contain a high level of arginine, fiber, vitamin E, polyphenolic compounds, magnesium and monounsaturated fatty acids, and particularly oleic acid.[13] Although, nut consumption has the above-mentioned benefits, many individuals who are trying to lose weight due to nut's high energy density may consciously avoid their consumption.
Epidemiological studies have shown that the consumption of nuts (such as almond) is inversely related to body weight.[17,18,19,20] The effect of nut consumption in the context of a weight-loss program have been evaluated only by a few randomized studies and their results were somewhat contradictory.[21] Among nuts, almonds approximately have the highest amount of protein and fiber.[22] This current study aims to find out the effects of a balanced hypocaloric almond-enriched diet (AED) in comparison to a balanced hypocaloric nut-free diet (NFD) on body weight and cardiovascular disease risk factors in women with body mass index (BMI) ≥25 for 3-month.
MATERIALS AND METHODS
Participants
A total of 152 subjects volunteered to participate in this study. Participants were recruited through public advertisements and 108 cases that had inclusion criteria were selected. Inclusion criteria were BMI ≥25, an age of 20-55 years and had no exercise (they had light physical activity: Doing household tasks, riding in a car, light activity while sitting.). The subjects were all premenopause females.
The individuals who had following criteria were not included to the study: Having a chronic illness (e.g., cancer, renal failure, cardiovascular disease, liver, and lung failure), uncontrolled hypertension (defined as a blood pressure ≥180/100 mmHg), taking lipid-lowering medications or vitamin supplements, an inflammatory condition (e.g., lupus), diabetes or use of anti-hyperglycemic drugs, working night shifts, pregnancy or lactation, smoking, alcohol consumption or any known allergy or sensitivity to nuts. Additional criteria that cause subject not included in the study were being on weight control diets or any specific diets at the time, use of medications known to affect body weight or a weight-loss of ≥5 kg in the preceding 6-month.
Also, participants who did not comply with their diet, did not do their recommended walking or did not intend to continue the study were excluded from the study. Subjects were asked to visit in valiasr charity clinic, Shiraz, Iran. This study was conducted from March to September 2013.
This study protocol was approved by the Ethics Committee of Human Experimentation of Shiraz University of Medical Sciences and written informed consent was obtained from each participant. Furthermore, this trial was registered in Iranian Registry of Clinical Trials with ID number of IRCT2013062313751N1.
Study design and diets
This study was a randomized controlled trial. A sample of 80 based on BMI was calculated to detect the predicted difference of eight between the means of two groups with a power level of 80% and the significance level set to 0.05 if the standard deviation (SD) was 12.7 and 12.8.[23] The calculated required sample size was 40 in each group. To allow for attrition, a sample size of 108 subjects was selected (54 from each group).
Participants were randomly assigned into almond and nut-free groups through the balanced block randomization method (block size of four). Three 24-h dietary recalls (2 weekdays and 1 for weekend day), for the assessments of food intake at baseline, end of the study and the end of each month were carried out from all participants.
At the beginning, balanced low calorie diets for both groups were designed (a balanced, restricted-energy diet should be nutritionally adequate except for energy: Approximately, 50-55% of total kilocalories for carbohydrates, 15-25% of total kilocalories for proteins and fat content should not exceed 30% of total calories[24]). Energy requirements were calculated according to the Harris Benedict equation. For everyone, 1000 kcal were reduced from the total calculated energy requirement. In both groups, the percentage of energy from macronutrients was the same (approximately 54% for carbohydrates, 16% for proteins, and 30% for fat). The almond group was requested to consume 50 g raw almond in the form of two snacks (approximately, 25 g raw almond in each snack) per day while the nut-free group were asked not to consume any nut. Instead of almond consumption, compensatory serving from the meat and fat exchange lists (like sunflower oil and corn oil) were used by the nut-free group participants. Supplies of prepackaged almonds (each package contain 50 g of almond) were given to participants who are going to the clinic monthly.
All participants were instructed to maintain their usual activity habits. Moreover, both groups were recommended to walk with medium speed 30-min every day. They were trained about their diet, healthy nutrition, and self-monitoring and stimulus control separately. All participants requested to comply with their diets for 3-month. They were called by phone every 15 days to ask about their situations and diet compliance. Also, suggestions to enhance compliance were provided. Moreover, intervention protocol and assessment of their compliance (including food intake and recommended walking) was checked by using 24-h dietary recalls.
Weight, waist and hip circumferences were determined by standard anthropometric methods in the beginning and after 3-month at the end of the study. Weight was measured to the nearest 0.1 kg on a seca electronic scale when the subjects were fasting, with no shoes and with light-weight clothing. BMI was calculated as weight (kg) divided by height (m2). Waist and hip circumference measurements were made to the nearest 0.1 cm by a tape measure. Waist circumferences (WC) were measured midway between the last rib and the ileac crest. Height was determined to the nearest 0.1 cm by using a stadiometer only at baseline.
Blood pressure was assessed by using a calibrated automatic digital monitor. After the participants sat quietly for 5-min, two blood pressure readings were made separated by a 1-min rest period. The average of the two readings was used to determine blood pressure.[21]
Biological sample collection and analysis
Participants were recruited for a blood sample collection on separate days. A volume of 10 ml blood samples were drown from arm after subjects had fasted overnight (12-h). In order to obtain plasma and to avoid clotting, 2 cc of blood samples were put in a tube containing ethylenediaminetetraacetic acid 5% (0.3 ml). Plasma separated by centrifugation at 1500 g for 10-min. Venous blood samples were taken using venous retention needles prior to and at the end of the study and analyzed for fasting blood sugar (FBS), TC, triglyceride, high density lipoprotein-cholesterol (HDL-C), and LDL-C concentrations. Lipid profiles (plasma total TC, HDL-C, LDL-C, and triglycerides) and FBS were measured based on a photometric method (Autoanalyzer BT 1500, blotecnica Instruments, Italy). To eliminate day-to-day laboratory variances, all blood samples were analyzed in a single batch following completion of the study.
Statistical analysis
Data were analyzed using the IBM SPSS statistical software (version 19, IBM Company, Armonk, NY, USA). The results are expressed as mean ± SD. Paired t-test was used for comparison of the measurements before and after the study in each group. The independent sample t-test was used for between group comparisons at baseline and at 3-month postintervention. Nonparametric tests such as sign test or Mann–Whitney U-test were used to analyze the variables that their distribution was not normal. Analysis of covariance (ANCOVA) was used to adjust the probable confounding effect of FBS, BMI and systolic blood pressure. P < 0.05 were considered statistically significant in all statistical tests.
RESULTS
In this study, 54 subjects participated in each group. During the study, four subjects in the almond group did not continue the study, one due to pregnancy and others for personal problems. Four subjects in the nut-free group were excluded because two of them did not follow the planned diet and the others due to their personal problems. Ultimately, 50 persons in each group continued the study.
Characteristics of the sample at baseline are described in Table 1.
Table 1.
Baseline characteristics of the subjects
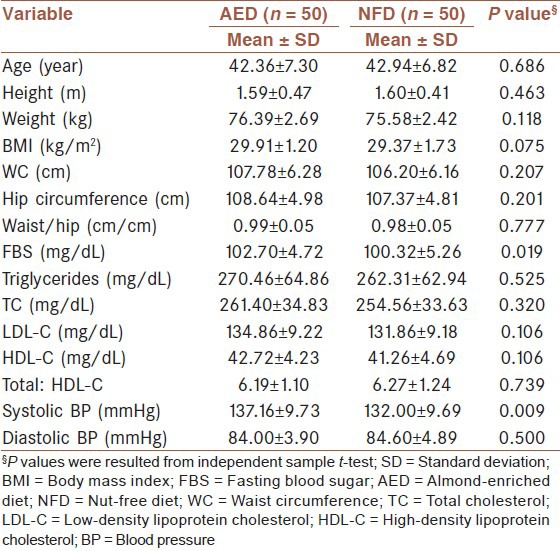
There were no statistically significant differences between the two groups except for FBS and systolic blood pressure.
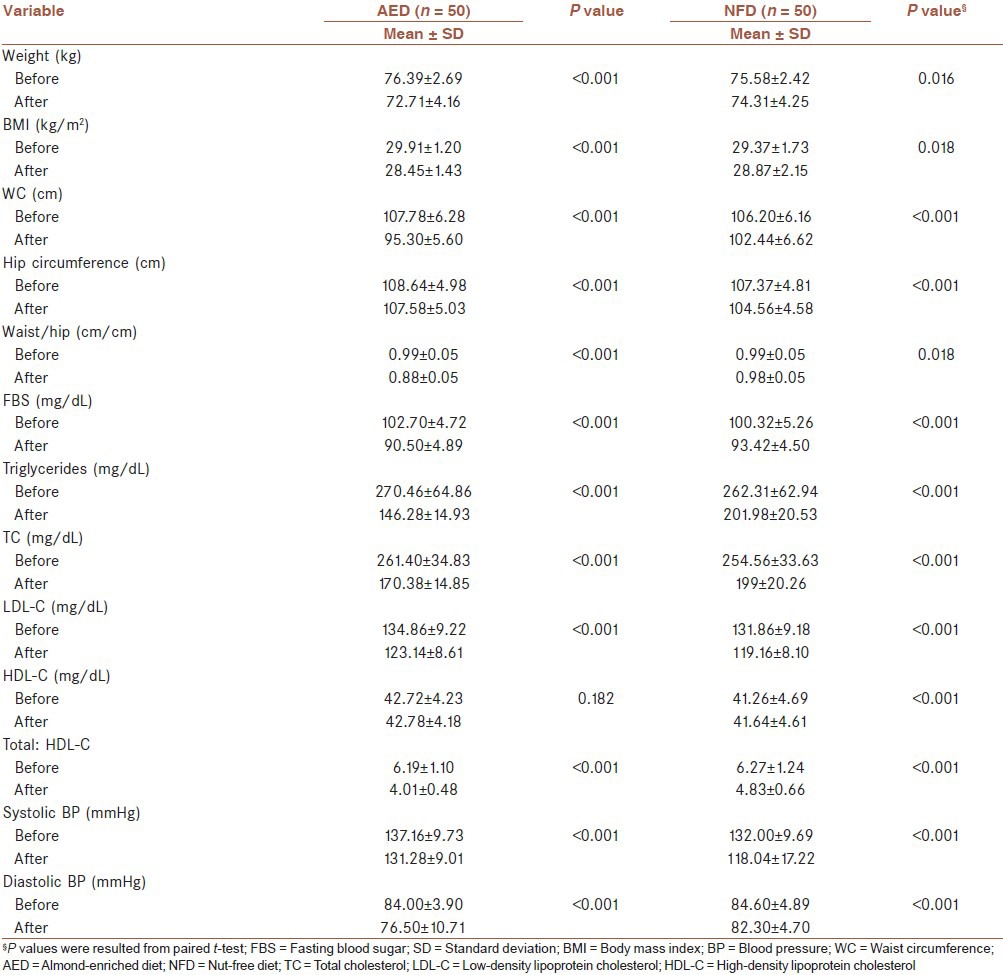
The effects of hypocaloric diet on the parameters with and without almonds are presented in Table 2.
Table 2.
Comparison of parameters values before and after the study in both groups
Anthropometric factors
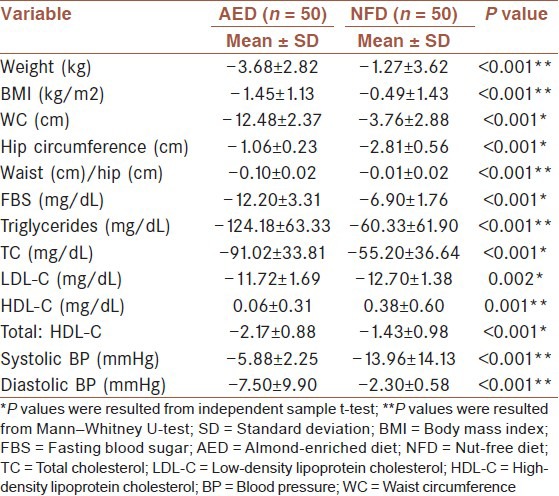
The almond group lost significantly more weight than the nut-free group after 3-month (−3.68 compared with −1.27 kg, P < 0.001). Also, reduction of WC (P < 0.001) and waist to hip circumference ratio (W/H) (P < 0.001) in the almond group were significantly higher, than the nut-free group [Table 3].
Table 3.
Mean differences in the two groups by treatment condition from baseline to 3-month
Plasma lipids and fasting blood sugar
In the almond group, greater significant reduction in triglycerides, TC, Total: HDL-C and FBS were found than the nut-free group after 3-month [Table 3]. LDL-C decreased in both groups over time, but greater reductions in LDL-C were observed significantly in the nut-free group. Increase of HDL in the almond group was not significant at the end of the study while in the nut-free group, this was significant [Table 2]; however, significant differences were found between the two groups after 3-month. Increase of HDL-C in the nut-free group was greater than the almond group [Table 3].
Blood pressure
Systolic and diastolic blood pressure decreased with weight-loss in both groups [Table 2]. The greater reduction in diastolic blood pressure observed in the almond group was statistically significant at the end of the study, but inversely systolic blood pressure in the almond group had less reduction in comparison with the nut-free group [Table 3].
Table 3 compared the effects of the two hypocaloric diet on the parameters.
Because there were significant differences in FBS and systolic blood pressure between the two groups at baseline, we repeated the analysis for these variables and also for BMI to adjust the probable confounding effect of them by using ANCOVA. The significant variables remained significant after controlling the effect of probable confounding such as BMI. P value did not change except for BMI (P = 0.001) [Table 3].
DISCUSSION
Increased prevalence of overweight and obesity in the community, and the risk of chronic diseases associated with obesity encourage us to find ways to reduce weight. We know nuts (such as almond) have many advantages and the evidences from epidemiologic studies have indicated a negative relation between nut consumption and body weight.[17,18,19,20] Perhaps one of the advisable factors for weight management program is nut's consumption.
The present trial was designed to evaluate the comparison effect of a balanced hypocaloric diet with and without almonds on weight reduction and lipid profiles in females with BMI ≥25 over a 3-month period.
In this study, both groups (almond and nut-free) experienced significant weight reduction after 3-month, but the greater weight-loss in the almond group was significant. Furthermore, the almond group had more reduction in BMI, WC and W/H than the nut-free group, all of which were significant. These findings are similar to the results obtained by Wien et al.,[23] where 65 overweight and obese subjects were randomized to consume complex carbohydrate enriched or an almond-enriched low calorie diets for 24 weeks under the free-living condition. The AED group consumed approximately 84 g/d of almonds. Both diet groups lost weight, but the almond group had greater reduction in weight, BMI, and WC.[23]
In another weight reduction study by McManus et al.,[25] 101 overweight participants were fed either a low-fat (20% energy from fat) or a moderate fat diet (35% energy from fat) including several nuts. The moderate fat group experienced superior adherence and greater weight-loss and decrease in WC over 18-month while the low fat group regained weight progressively.[25]
In contrast, a study examined by Foster et al.[21] examined the effects of a hypocaloric, AED compared with a hypocaloric NFD on body weight and cardiovascular disease risk factors in the context of an 18-month weight reduction program. One hundred twenty-three overweight and obese subjects were randomly divided to consume an AED or NFD. Both groups were trained in traditional behavioral methods of weight control. NFD group had slightly, but significantly more weight-loss than the AED group at 6-month, but there were no statistically significant differences in body weight between the groups at 18-month.[21] These findings may be secondary to the NFD group choosing foods for snacks with lower calories than nuts; therefore, resulting in slightly greater energy deficits.
In other studies outside the context of weight reduction conducted by Spiller et al.,[26] Sabaté et al.[27] and Jenkins et al.[28] revealed no changes in weights of subjects when they received almonds. Also Tamizifar et al.,[29] Wien et al.[30] and Hollis and Mattes[31] found similar results.
There are several mechanisms that can potentially explain why nut consumption could help control weight. Firstly, nuts provide greater satiety. Nuts are energy dense foods with high fiber, protein, unsaturated fats, various phytochemicals, and low glycemic index; all of them are dietary factors that have been associated with satiety responses. Secondly, chronic consumption of nuts may lead to increased resting energy expenditure due to high unsaturated fatty acids, which may influence diet-induced thermogenesis. Thirdly, bioavailability of fatty acids in nuts may not be full, and it is likely because of the nut parenchyma cell wall's resistance to enzymatic degradation in the gastrointestinal tract which leads to the encapsulation of fat. However, the indicated mechanisms are not clear.[7,19,22,23,31,32,33]
Consumption of almonds has been shown to have health promoting benefits on lipid profiles. In a pooled analysis of 25 intervention trials study performed by Sabaté et al.[9] on 583 men and women with normolipidemia and hypercholesterolemia (who did not use lipid-lowering medications) indicated that a mean daily consumption of 67 g of nuts resulted in mean reduction in TC, LDL, LDL: HDL and TC: HDL. Triglycerides levels were reduced in individuals whose blood triglyceride levels were at least 150 mg/dL, and there was a correlation between the effects of nut consumption and dose related.[9] The results obtained in another study by Sabaté et al.[27] are similar to these results. In a randomized crossover design, 25 healthy subjects were recruited to comply with three isocaloric diets for 4 weeks. A Step I diet, a low-almond diet, and a high-almond diet were experimental diets that the participants followed in which almonds contributed 0%, 10%, and 20% (68 g) of total energy, respectively. Inverse relations between the percentage of energy in the diet from almonds and the subject's TC, LDL-C concentrations and the ratios of LDL to HDL-C were found.[27]
In agreement with these findings, Jenkins et al.[28] in a randomized cross-over study used three isocaloric (mean 423 kcal/d) supplements. Participants were 27 hyperlipidemic males and females that consumed supplements (included full-dose almonds (73 ± 3 g/d), half-dose almonds plus half-dose muffins, and full-dose muffins) each for 4 weeks. The greatest reduction in levels of blood lipids were experienced in full-dose almonds.[28]
In a randomized, cross-over clinical trial performed by Tamizifar et al.,[29] 35 hyperlipidemic subjects were selected to consume almond (25 g) or a reference diet. Duration of each phase was 4 weeks. TC and LDL were reduced significantly in almond group, but the changes of HDL and triglycerides were not significant.[28] Results of Tamizifar's et al. study consist with other studies. Furthermore, this study suggested that consumption of almond had a favorable lipid-altering effect, even in lower dose than previous studies (25 g vs. 100 g).[29]
Foster et al.[21] showed that in spite of a slightly smaller weight reduction at 6-month in the AED group, triglycerides, TC, and TC: HDL-C improved more in the AED group than in the NFD group. Regards HDL, LDL, and very-low-density lipoprotein (VLDL) levels, no differences were found between the groups at 6- or 18-month.[21]
In this study, TC and triglycerides improved more in the almond group than the nut-free group like other studies, but an increase in HDL and a decrease in LDL in the nut-free group were significantly greater than the almond group. In our sample, the effect of almonds on LDL may have been attenuated due to higher levels of LDL in the almond group at baseline and perhaps the effect of almond on LDL are greater in subjects with lower LDL concentration. In addition, pooled analyses suggested that nut consumption were more effective in subjects with a lower MBI.[9] Therefore, the potential cholesterol-lowering effects of nut consumption may have restricted by the elevated BMI in our sample.
Foster et al.[21] indicated no differences in HDL between the groups and pooled analyses[9] proposed that no significant effect on the mean HDL were observed by nut consumption. In our study, HDL increased slightly in the almond group without significance, but significant differences were found between the two groups after 3-month. Furthermore, perhaps the nut-free group had more exercise than the almond group or the almond group did not do their recommended amount of walking, which resulted in greater improvement of HDL in nut-free group.
Although improvement of LDL and HDL in the nut-free group was more, greater improvement of TC: HDL-C, which has been recently suggested as a good or better indicator of predicting cardiovascular disease risk than LDL-C,[28,34] were observed in the almond group. These results are in agreement with those obtained by Foster et al.[21] and Sabaté et al.[9] and are consistent with a cardioprotective effect.
Pearson et al.[35] suggested that if the reduction in triglycerides and cholesterol preserved over a long time, reduction in cardiovascular disease risk might be expected. The effect of almond mechanisms that help in causing improvements in triglycerides and TC remain unclear; however, they seem to be related to effects on VLDL metabolism. Unsaturated fatty acids are rich in almonds and can influence VLDL metabolism by either reduced hepatic VLDL production or increased VLDL lipolysis.[21,26]
Fasting blood sugar decreased over the period of study in both groups, but greater significant reductions were observed in the almond group. In Wien's et al. study[23] fasting glucose decreased significantly in both dietary interventions by a similar extent, but an improvement in insulin sensitivity among participants consuming almonds were found. These findings were similar to results acquired in another study by Wien et al.[30] Rocca et al.[36] have suggested that almond consumption was related to improvement of insulin sensitivity. High content of oleic acid in almonds may improve B-cell efficiency through enhanced intestinal secretion of glucagon-like-peptide-1.
Systolic and diastolic blood pressure decreased with weight-loss in both groups after 3-month consistent with Foster et al.[21] but in Foster's study no differences were found between the groups. In our study, a significantly greater reduction in diastolic blood pressure was observed in the almond group at the end of study, but inversely, systolic blood pressure in the almond group had significantly less reduction compared to the nut-free group. That may be because subjects in the almond group had higher systolic blood pressure at baseline, so the effect of almond on systolic blood pressure was attenuated. In Wien's et al. study[23] diastolic blood pressure decreased similarly in both groups, but systolic blood pressure decreased only in the almond group. In other studies conducted by Spiller et al.,[26] Jenkins et al.[28] and Wien et al.[30] blood pressure did not change.
This study is not without limitations. Participants in our study were females; therefore, our results may not be generalized to males. In addition, it is possible that errors may have occurred in the participant's self-reported dietary intake. However, further studies are needed to demonstrate theories on the effects of almonds on weight-loss.
CONCLUSION
The balanced hypocaloric AED in comparison to the balanced hypocaloric NFD led to a greater weight-loss and better improvements in the studied cardiovascular disease risk factors.
AUTHORS’ CONTRIBUTIONS
ZA carried out the design and all the experiments and prepared the manuscript. MS carried out the design and all the experiments and prepared the manuscript. SK analyzed the data and provided assistance for manuscript preparation. All authors have read and approved the content of the manuscript.
ACKNOWLEDGMENT
The present article was extracted from the thesis written by Zohreh Abazarfard and was financially supported by Shiraz University of Medical Sciences, Grant number: 92-6498. The authors grateful to Ms. Asma Kazemi, Ms. Ghazal Moradzadeh and also Mr. Amin Mosleh at Center for Development of Clinical Research of University of Medical Sciences for editorial assistance.
Footnotes
Source of Support: Shiraz University of Medical Sciences (Grants No. 92-6498)
Conflict of Interest: None declared.
REFERENCES
- 1.National Health and Medical Research Council. Canberra: 2013. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia. Available from: https://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/n57_obesity_guidelines_131204_0.pdf . [Google Scholar]
- 2.Holmbäck I, Ericson U, Gullberg B, Wirfält E. A high eating frequency is associated with an overall healthy lifestyle in middle-aged men and women and reduced likelihood of general and central obesity in men. Br J Nutr. 2010;104:1065–73. doi: 10.1017/S0007114510001753. [DOI] [PubMed] [Google Scholar]
- 3.Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA. 2006;295:1549–55. doi: 10.1001/jama.295.13.1549. [DOI] [PubMed] [Google Scholar]
- 4.Kuulasmaa K, Tunstall-Pedoe H, Dobson A, Fortmann S, Sans S, Tolonen H, et al. Estimation of contribution of changes in classic risk factors to trends in coronary-event rates across the WHO MONICA Project populations. Lancet. 2000;355:675–87. doi: 10.1016/s0140-6736(99)11180-2. [DOI] [PubMed] [Google Scholar]
- 5.Kopelman PG. Obesity as a medical problem. Nature. 2000;404:635–43. doi: 10.1038/35007508. [DOI] [PubMed] [Google Scholar]
- 6.Natoli S, McCoy P. A review of the evidence: Nuts and body weight. Asia Pac J Clin Nutr. 2007;16:588–97. [PubMed] [Google Scholar]
- 7.Jaceldo-Siegl K, Sabaté J, Rajaram S, Fraser GE. Long-term almond supplementation without advice on food replacement induces favourable nutrient modifications to the habitual diets of free-living individuals. Br J Nutr. 2004;92:533–40. doi: 10.1079/bjn20041223. [DOI] [PubMed] [Google Scholar]
- 8.US Department of Agriculture, US Department of Health and Human Services. Dietary Guidelines for Americans 2010. 2011. Jan, Available from: http://www.cnpp.usda.gov/Publications/DietaryGuidelines/2010/PolicyDoc/PolicyDoc.pdf .
- 9.Sabaté J, Oda K, Ros E. Nut consumption and blood lipid levels: A pooled analysis of 25 intervention trials. Arch Intern Med. 2010;170:821–7. doi: 10.1001/archinternmed.2010.79. [DOI] [PubMed] [Google Scholar]
- 10.Griel AE, Kris-Etherton PM. Tree nuts and the lipid profile: A review of clinical studies. Br J Nutr. 2006;96(Suppl 2):S68–78. doi: 10.1017/bjn20061866. [DOI] [PubMed] [Google Scholar]
- 11.Li Z, Song R, Nguyen C, Zerlin A, Karp H, Naowamondhol K, et al. Pistachio nuts reduce triglycerides and body weight by comparison to refined carbohydrate snack in obese subjects on a 12-week weight loss program. J Am Coll Nutr. 2010;29:198–203. doi: 10.1080/07315724.2010.10719834. [DOI] [PubMed] [Google Scholar]
- 12.Kris-Etherton PM, Zhao G, Binkoski AE, Coval SM, Etherton TD. The effects of nuts on coronary heart disease risk. Nutr Rev. 2001;59:103–11. doi: 10.1111/j.1753-4887.2001.tb06996.x. [DOI] [PubMed] [Google Scholar]
- 13.Jiang R, Manson JE, Stampfer MJ, Liu S, Willett WC, Hu FB. Nut and peanut butter consumption and risk of type 2 diabetes in women. JAMA. 2002;288:2554–60. doi: 10.1001/jama.288.20.2554. [DOI] [PubMed] [Google Scholar]
- 14.Djoussé L, Rudich T, Gaziano JM. Nut consumption and risk of hypertension in US male physicians. Clin Nutr. 2009;28:10–4. doi: 10.1016/j.clnu.2008.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lairon D, Arnault N, Bertrais S, Planells R, Clero E, Hercberg S, et al. Dietary fiber intake and risk factors for cardiovascular disease in French adults. Am J Clin Nutr. 2005;82:1185–94. doi: 10.1093/ajcn/82.6.1185. [DOI] [PubMed] [Google Scholar]
- 16.Holt SH, Miller JC, Petocz P, Farmakalidis E. A satiety index of common foods. Eur J Clin Nutr. 1995;49:675–90. [PubMed] [Google Scholar]
- 17.Martínez-González MA, Bes-Rastrollo M. Nut consumption, weight gain and obesity: Epidemiological evidence. Nutr Metab Cardiovasc Dis. 2011;21(Suppl 1):S40–5. doi: 10.1016/j.numecd.2010.11.005. [DOI] [PubMed] [Google Scholar]
- 18.Mattes RD, Kris-Etherton PM, Foster GD. Impact of peanuts and tree nuts on body weight and healthy weight loss in adults. J Nutr. 2008;138:1741S–5. doi: 10.1093/jn/138.9.1741S. [DOI] [PubMed] [Google Scholar]
- 19.Sabaté J. Nut consumption and body weight. Am J Clin Nutr. 2003;78:647S–50. doi: 10.1093/ajcn/78.3.647S. [DOI] [PubMed] [Google Scholar]
- 20.Mozaffarian D, Hao T, Rimm EB, Willett WC, Hu FB. Changes in diet and lifestyle and long-term weight gain in women and men. N Engl J Med. 2011;364:2392–404. doi: 10.1056/NEJMoa1014296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Foster GD, Shantz KL, Vander Veur SS, Oliver TL, Lent MR, Virus A, et al. A randomized trial of the effects of an almond-enriched, hypocaloric diet in the treatment of obesity. Am J Clin Nutr. 2012;96:249–54. doi: 10.3945/ajcn.112.037895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rajaram S, Sabaté J. Nuts, body weight and insulin resistance. Br J Nutr. 2006;96(Suppl 2):S79–86. doi: 10.1017/bjn20061867. [DOI] [PubMed] [Google Scholar]
- 23.Wien MA, Sabaté JM, Iklé DN, Cole SE, Kandeel FR. Almonds vs complex carbohydrates in a weight reduction program. Int J Obes Relat Metab Disord. 2003;27:1365–72. doi: 10.1038/sj.ijo.0802411. [DOI] [PubMed] [Google Scholar]
- 24.Lysen LK, Israel DA. Nutrition in weight management. In: Mahan LK, Escott-Stump S, Raymond J, editors. Krause's Food and the Nutrition Care Process. 13th ed. United States of America: Elsevier; 2012. p. 474. [Google Scholar]
- 25.McManus K, Antinoro L, Sacks F. A randomized controlled trial of a moderate-fat, low-energy diet compared with a low fat, low-energy diet for weight loss in overweight adults. Int J Obes Relat Metab Disord. 2001;25:1503–11. doi: 10.1038/sj.ijo.0801796. [DOI] [PubMed] [Google Scholar]
- 26.Spiller GA, Miller A, Olivera K, Reynolds J, Miller B, Morse SJ, et al. Effects of plant-based diets high in raw or roasted almonds, or roasted almond butter on serum lipoproteins in humans. J Am Coll Nutr. 2003;22:195–200. doi: 10.1080/07315724.2003.10719293. [DOI] [PubMed] [Google Scholar]
- 27.Sabaté J, Haddad E, Tanzman JS, Jambazian P, Rajaram S. Serum lipid response to the graduated enrichment of a Step I diet with almonds: A randomized feeding trial. Am J Clin Nutr. 2003;77:1379–84. doi: 10.1093/ajcn/77.6.1379. [DOI] [PubMed] [Google Scholar]
- 28.Jenkins DJ, Kendall CW, Marchie A, Parker TL, Connelly PW, Qian W, et al. Dose response of almonds on coronary heart disease risk factors: Blood lipids, oxidized low-density lipoproteins, lipoprotein (a), homocysteine, and pulmonary nitric oxide: A randomized, controlled, crossover trial. Circulation. 2002;106:1327–32. doi: 10.1161/01.cir.0000028421.91733.20. [DOI] [PubMed] [Google Scholar]
- 29.Tamizifar B, Rismankarzadeh M, Vosoughi AA, Rafieeyan M, Tamizifar B, Aminizade A. A low-dose almond-based diet decreases LDL-C while preserving HDL-C. Arch Iran Med. 2005;8:45–51. [Google Scholar]
- 30.Wien M, Bleich D, Raghuwanshi M, Gould-Forgerite S, Gomes J, Monahan-Couch L, et al. Almond consumption and cardiovascular risk factors in adults with prediabetes. J Am Coll Nutr. 2010;29:189–97. doi: 10.1080/07315724.2010.10719833. [DOI] [PubMed] [Google Scholar]
- 31.Hollis J, Mattes R. Effect of chronic consumption of almonds on body weight in healthy humans. Br J Nutr. 2007;98:651–6. doi: 10.1017/S0007114507734608. [DOI] [PubMed] [Google Scholar]
- 32.Alper CM, Mattes RD. Effects of chronic peanut consumption on energy balance and hedonics. Int J Obes Relat Metab Disord. 2002;26:1129–37. doi: 10.1038/sj.ijo.0802050. [DOI] [PubMed] [Google Scholar]
- 33.Ellis PR, Kendall CW, Ren Y, Parker C, Pacy JF, Waldron KW, et al. Role of cell walls in the bioaccessibility of lipids in almond seeds. Am J Clin Nutr. 2004;80:604–13. doi: 10.1093/ajcn/80.3.604. [DOI] [PubMed] [Google Scholar]
- 34.Ridker PM, Rifai N, Cook NR, Bradwin G, Buring JE. Non-HDL cholesterol, apolipoproteins A-I and B100, standard lipid measures, lipid ratios, and CRP as risk factors for cardiovascular disease in women. JAMA. 2005;294:326–33. doi: 10.1001/jama.294.3.326. [DOI] [PubMed] [Google Scholar]
- 35.Pearson TA, Blair SN, Daniels SR, Eckel RH, Fair JM, Fortmann SP, et al. AHA guidelines for primary prevention of cardiovascular disease and stroke: 2002 update: Consensus panel guide to comprehensive risk reduction for adult patients without coronary or other atherosclerotic vascular diseases. American Heart Association Science Advisory and Coordinating Committee. Circulation. 2002;106:388–91. doi: 10.1161/01.cir.0000020190.45892.75. [DOI] [PubMed] [Google Scholar]
- 36.Rocca AS, LaGreca J, Kalitsky J, Brubaker PL. Monounsaturated fatty acid diets improve glycemic tolerance through increased secretion of glucagon-like peptide-1. Endocrinology. 2001;142:1148–55. doi: 10.1210/endo.142.3.8034. [DOI] [PubMed] [Google Scholar]