

Abstract
Most of the ingested foreign bodies pass uneventfully through the gastrointestinal tract. However, long and rigid foreign bodies are associated with an increased risk of gastrointestinal impaction, perforation, and bleeding. Spontaneous passage of a toothbrush has not been reported till date and the technique of its removal is a curiosity for surgeons. Endoscopy is a recommended technique for the removal of such complex foreign bodies. However, if it fails, the foreign body can be removed successfully with a laparoscopic gastrotomy. We devised an innovative technique by using pneumatic gastric insufflation and extracted the toothbrush by a tiny gastrotomy under local anesthesia.
Keywords: Gastrotomy, local anesthesia, toothbrush, upper gastrointestinal endoscopy
INTRODUCTION
The pylorus, duodenal C-loop, and ileocecal valve are the three physiological narrowings in the gastrointestinal tract, and most of the swallowed indigestible foreign bodies pass through it without complications.[1] However, foreign bodies such as a toothbrush cannot pass out of the stomach, and the gastrointestinal tract should get rid of these objects as soon as possible to avoid pressure necrosis and gastrointestinal perforation.[2] Although these objects are extracted either by endoscopy or laparoscopic gastrostomy,[3] we devised an innovative technique by using pneumatic gastric insufflation and extracted the toothbrush by a tiny gastrotomy under local anesthesia.
CASE REPORT
A 35-year-old male presented in our hospital at M.M. Institute of Medical Sciences and Research (MMIMSR), Mullana, Ambala, Haryana, India in May 2013; he had accidentally swallowed a toothbrush two months back and there was a history of epigastric discomfort especially after meals. However, the vital signs were within normal limits and the abdomen was soft and nontender. X-ray of the abdomen suggested the presence of a foreign body and a computed tomography (CT) scan was done which confirmed a toothbrush lying in the stomach [Figures 1, 2]. An upper gastrointestinal endoscopy was done which revealed the toothbrush in the stomach with its head toward the gastroduodenal junction. Biopsy forceps were used to deliver the toothbrush by holding its bristles [Figure 3]. However, it could not be removed even after repeated attempts. The endoscope was kept inside to insufflate and distend the stomach and a minilaparotomy with gastrotomy of 1.5-2 cm was performed through the midline under local anesthesia and the toothbrush was successfully removed. The postprocedure period was uneventful.
Figure 1.

X-ray of the abdomen suggesting the presence of the toothbrush in the abdomen
Figure 2.
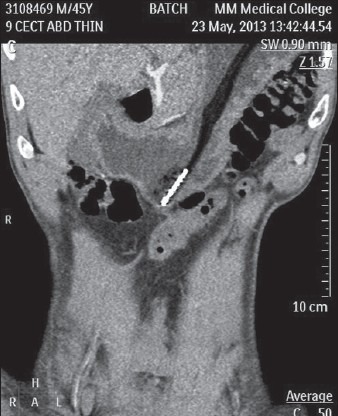
Computed tomography (CT) scan of the abdomen showing the presence of the toothbrush in the tomach
Figure 3.
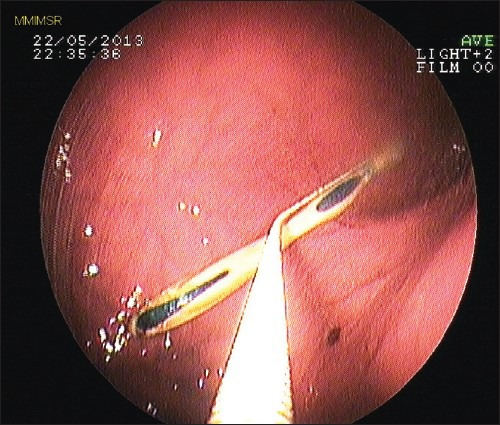
Endoscopic picture of toothbrush with biopsy forceps in situ to retrieve it from the stomach
DISCUSSION
In the stomach, 80-90% of foreign bodies pass uneventfully through the gastrointestinal tract without complications.[1] However, objects longer than 10 cm like a toothbrush cannot negotiate the duodenal C-loop due to its fixed position in the retroperitoneum, and these must be removed as soon as possible to avoid pressure necrosis and gastric perforation.[2,4,5,6] More than 40 cases of toothbrush ingestion have been reported in the literature till date.[3,7] Endoscopic removal of these objects is strongly recommended.[8,9] However, extreme caution and experience of the endoscopist is required for such procedures. In failed cases of endoscopic removal, laparoscopic gastrotomy is an alternative. However, we devised a simple technique of minilaparotomy and gastrotomy under local anesthesia for removing such foreign bodies. In this technique, the stomach is distended with the help of air insufflation through the endoscope and a small incision is made in the midepigasrium under local anesthesia and the foreign object can be removed directly under the vision of the endoscope.
CONCLUSION
A swallowed toothbrush is a rare occurrence and it never passes through the gastrointestinal tract spontaneously. Early removal of the toothbrush is critical for reducing morbidity and mortality. In cases where endoscopic removal fails, endoscopy still remains an aid in performing surgical gastrotomy for delivering such complex foreign bodies under local anesthesia.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Smith MT, Wong RK. Foreign bodies. Gastrointest Endosc Clin N Am. 2007;17:361–82. doi: 10.1016/j.giec.2007.03.002. [DOI] [PubMed] [Google Scholar]
- 2.Li ZS, Sun ZX, Zou DW, Xu GM, Wu RP, Liao Z. Endoscopic management of foreign bodies in the upper-GI tract: Experience with 1,088 cases in China. Gastrointest Endosc. 2006;64:485–92. doi: 10.1016/j.gie.2006.01.059. [DOI] [PubMed] [Google Scholar]
- 3.Niknam R, Mahmoudi L, Nasseri-Moghaddam S. An incidentally swallowed toothbrush. Arch Iran Med. 2012;15:177–8. [PubMed] [Google Scholar]
- 4.Bastos I, Gomes D, Cotrim I, Gouveia H, Donato A, de Freitas D. An unusual endoscopic procedure to remove a toothbrush from the stomach. Endoscopy. 1996;28:5250. doi: 10.1055/s-2007-1005540. [DOI] [PubMed] [Google Scholar]
- 5.Faust J, Schreiner O. A swallowed toothbrush. Lancet. 2001;357:10. doi: 10.1016/S0140-6736(00)04238-0. [DOI] [PubMed] [Google Scholar]
- 6.Kim IH, Kim HC, Koh KH, Kim SH, Kim SW, Lee SO, et al. Journey of a swallowed toothbrush to the colon. Korean J Intern Med. 2007;22:106–8. doi: 10.3904/kjim.2007.22.2.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Harvey M, Cave G, Prince G. Endoscopic removal of an inadvertently swallowed toothbrush in the emergency department. Case Rep Emerg Med 2012. 2012:568163. doi: 10.1155/2012/568163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nagashima R, Saitoh H, Fukase Y, Takahashi T. Endoscopic removal of a toothbrush using biopsy forceps and thread. Endoscopy. 1998;30:S90–1. doi: 10.1055/s-2007-1001407. [DOI] [PubMed] [Google Scholar]
- 9.Mughal M. Accidental ingestion of a toothbrush. Arch Emerg Med. 1986;3:119–23. doi: 10.1136/emj.3.2.119. [DOI] [PMC free article] [PubMed] [Google Scholar]