

Abstract
Background
Since the political transition in 1991, Russia has been targeted intensively by the transnational tobacco industry. Already high smoking rates among men have increased further; traditionally low rates among women have more than doubled. The tobacco companies have so far faced little opposition as they shape the discourse on smoking in Russia. This paper asks what ordinary Russians really think about possible actions to reduce smoking.
Methods
A representative sample of the Russian population (1600 respondents) was interviewed face-to-face in November 2007.
Results
Only 14% of respondents considered tobacco control in Russia adequate, while 37% felt that nothing was being done at all. There was support for prices keeping pace with or even exceeding inflation. Over 70% of all respondents favoured a ban on sales from street kiosks, while 56% believed that existing health warnings (currently 4% of front and back of packs) were inadequate. The current policy of designating a few tables in bars and restaurants as non-smoking was supported by less than 10% of respondents, while almost a third supported a total ban, with 44% supporting provision of equal space for smokers and non-smokers. Older age, non-smoking status and living a smaller town all emerged as significantly associated with the propensity to support of antismoking measures. The tobacco companies were generally viewed as behaving like most other companies in Russia, with three-quarters believing that they definitely or maybe bribe politicians. Knowledge of impact of smoking on health was limited with significant underestimation of dangers and addictive qualities of tobacco. A third believed that light cigarettes are safer than normal.
Conclusion
The majority of the Russian population would support considerable strengthening of tobacco control policies but there is also a need for effective public education campaigns.
Keywords: Russia, tobacco control, attitudes
Introduction
Russia has been a prime target for the transnational tobacco companies (TTCs). Following the political transition in 1991, TTCs devoted major efforts first to increase imports, taking advantage of western development assistance and barter trade, supplemented with targeted support for smuggling1 and, second, to establish a manufacturing practice.2 By 2000 the industry had invested at least US$1.7 billion.3
The reason for this effort was obvious. There was an established market among men, over two thirds of whom smoked, and enormous potential for growth among women, whose smoking rates had been traditionally very low.4 An emphasis on inward investment, from whatever source, and on basic state building meant that health considerations took a low priority.3 The Russian public health community was weak and unable to advocate for tobacco control whilst the TTCs enjoyed considerable influence, allegedly negotiating the overturn of a Soviet decree banning tobacco advertising as a precondition for a deal to import 34 billion cigarettes.5 Subsequent tobacco control laws have been largely ineffective, being based on industry voluntary codes and failing to specify effective enforcement mechanisms.3,6
Prices of cigarettes remain incredibly low and have fallen in real terms by 40% (foreign brands) and 50% (local brands) between 2000 and 2007. 7 Although Moscow is now among the most expensive cities in the world to live in, the taxation regime, levying between 10 and 30 US cents on each pack, means that a pack of filter cigarettes costs between US$0.33 and US$1.1.whilst non filtered cigarettes cost only US$.15 or less. Advertisements are banned on television but are widespread in magazines and product placement is common. A combination of ignorance and corruption has made tobacco control difficult. Most physicians smoke and many non- governmental organizations in the health arena support the message that “smoking is a free choice”.
The consequences have been predictable. The most recent data show that between 1992 and 2003 smoking rates increased significantly by 6% among men and more than doubled among women.8 Between 1990 and 2000 cigarette consumption increased by an unprecedented 81% despite a declining population.9 Unsurprisingly the TTCs view Russia as one of the most important global markets – second in importance only to China and growing rampantly, it has been one of their biggest success stories.10
It has been argued that increases so large in such a short timescale are unprecedented. 9 Industry journals suggest the TTCs can barely believe the continued success they have been enjoying there. 11 This combined with the sheer size of the market and the difficulty most TTCs have experienced in accessing China mean Russia is now one if not the most important market to the TTCs.9
This is especially alarming given the high toll of tobacco related disease that is a legacy of historically high rates of smoking. Even in 1992, 57% of adult men smoked. 8 In 2004 (the most recent data available) the death rate from lung cancer among Russian men was 78.4 per 100,000, more than double that in Sweden (30.7 per 100,000).12 In 2000 it was estimated that smoking accounted for 33% of all deaths among Russian men aged 35-69,13 and a 1996 review concluded that smoking was likely to be the most important factor explaining the east-west mortality divide in Europe.14 The problems are exacerbated by the high levels of alcohol consumption that act synergistically with smoking in the aetiology of some causes of death, such as aerodigestive cancers.
There are, however, some cautious grounds for optimism. There is growing recognition of the adverse effects of poor adult health in Russia on economic growth and the consequences for national security, with depopulation of strategic areas.15 Recent progress has been made in alcohol control as a result. More specifically, on 31 August 2006 a coalition of nongovernmental organizations independent of the tobacco industry came together to lobby for Russian ratification of the Framework Convention on Tobacco Control (FCTC), the world's first public health treaty, at a time when Russia was among only a few countries in the world not to have done so. The Russian State Duma (Parliament) approved a law paving the way for accession on 11th April 2008. Establishment of the Coalition caused considerable alarm in industry circles, stimulating establishment of an industry-dominated “Committee on the problem of tobacco” under the auspices of the Ministry of Health and a high-profile roundtable discussion entitled “Problems with acceding to the FCTC” where tobacco control activists were denied the right to speak. The tobacco industry, while claiming to support the FCTC, pushed for measures that would be ineffective. With substantial financial support now obtained from the Bloomberg Global Tobacco Control Initiative, the NGO coalition provides a unique opportunity to take effective action on smoking in Russia.
With Russia now moving towards ratifying the FCTC the need to adapt and enforce effective legislation becomes crucial. It will be essential to ensure that the industry does not undermine regulations implementing the FCTC, something it will make a high priority. One factor in the debate will be public opinion. Politicians recall the riots that accompanied shortages of cigarettes in the late 1980s, leading to an emergency purchase that was the largest ever cigarette import in the history of the tobacco giants.16 There is a widespread view that the Russian population has little interest in tobacco control but so far there has been no information in the public domain to indicate whether this is so. This paper begins the process of clarifying this issue.
Methods
During a period of two weeks (November 1-15, 2007) a nationwide representative survey of the adult population 18 years or older was undertaken by the Levada Analytical Centre, one of the most experienced social survey companies in Russia and with well established quality control processes in place. 17 The Russian Federation is divided into 87 regions (variously termed oblasts, republics and krais depending on the level of autonomy). These are grouped into seven “super-regions”. The sampling frame was as follows: within each of the seven super-regional groupings, five strata of settlements were constructed according to population size: cities > 1 million population, cities 0.5-1 million population; towns 100-500 thousand population; towns 10-100 thousand population; towns and villages < 10 thousand population. All 13 Russian cities with a population > 1 million were included. In each of the other strata settlements were selected at random to yield 13 smaller cities, 29 large towns, 31 medium towns, and 42 small towns and villages. The total number of settlements was 128. Twelve regions had been excluded for practical reasons. These were Chechnya, Ingushetia, Dagestan and North Ossetia, where there are unresolved civil conflicts, and some very remote regions of the circumpolar north where the population is largely nomadic. In total, these regions include 5% of the Russian population. The final sample included settlements from 46 out of the 87 regions of Russia.
In the second stage, between 1 and 10 electoral areas were sampled at random within each settlement in proportion to population size (266 areas). In the third stage, households were sampled using the random route method, with every 17th household in apartment blocks and every 5th household in houses and cottages. Finally, within households, the respondent aged 18 and above whose birthday was nearest to the interview date was selected. Where no-one was at home or individuals refused to be interviewed, the interviewer moved to the next dwelling due to be sampled. 15% of interviews were validated by telephone or by repeat visits by supervisors, with a further 20% validated by post. The survey data was subject to logical checks during the survey process. The survey instrument, administered in face to face interviews, contained 18 questions on attitudes to smoking, supplemented by basic demographic details. The final sample size was 1,600, with an initial response rate of 74% before substitution. Analysis was performed using SPSS (version 16).
A score was constructed from eight of the variables to summarise attitudes to tobacco control. In each case those favouring action were scored 1 and otherwise 0. The variables were favouring tax increases above or in line with inflation, warnings that are pictorial or larger text, banning sales in kiosks, smoking in films, in restaurants and on public transport. The determinants of being in favour of action were examined using multiple linear regression.
Results
The final sample was representative of the Russian population, as described in the 2002 census, in terms of age and sex. Smoking prevalence among younger respondents was similar to that obtained in the most recent round of the Russian Longitudinal Monitoring Survey although at older ages smokers were considerably over-represented in the sample (Table 1).
Table 1.
Characteristics of sample
| Sample n (%) | Sample Smoking prevalence | Census – share of 20+ age group | RLMS per cent smoking prevalence (2003) | ||
|---|---|---|---|---|---|
| Male | 18-24 | 115 (16) | 65 | 11.4% | 64 |
| 25-34 | 152 (21) | 75 | 20.9% | 70 | |
| 35-44 | 136 (19) | 72 | 23.0% | 72 | |
| 45-54 | 154 (21) | 84 | 20.9% | 65 | |
| 55-64 | 83 (12) | 75 | 11.5% | 57 | |
| 65+ | 84 (12) | 84 | 12.3% | 35 | |
| Female | 18-24 | 118 (13) | 35 | 9.2% | 23 |
| 25-34 | 144 (16) | 25 | 16.8% | 28 | |
| 35-44 | 156 (18) | 28 | 19.7% | 21 | |
| 45-54 | 169 (19) | 16 | 19.5% | 14 | |
| 55-64 | 114 (13) | 25 | 13.1% | 6 | |
| 65+ | 174 (20) | 16 | 21.7% | 2 | |
Note: due to presentation of published data, the lowest age group in the census column refers to the share of the population aged 20+ that is 20-24
Only 14% of respondents (male and female combined) considered that tobacco control in Russia was adequate, while 37% felt that nothing was being done at all. The figures are broken down by age and sex in Table 2. Non-smokers, women, and younger people were especially likely to believe that more action was needed. Opinion was fairly evenly divided on the issue of tax rises, either to keep pace or exceed inflation, and while men tended to be less in favour of price rises. For both sexes, support was greater among non-smokers. Over 70% of all respondents favoured a ban on sales from street kiosks and 71% of those not in favour took this view because they thought a ban would be ineffective (data not shown). This proposal even attracted support from the majority of smokers, both male and female, with support strongest among older people.
Table 2.
Attitudes to tobacco control in Russia
| Male | Female | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 18-34 | 35-54 | 55+ | non-smokers | Smokers | All | 18-34 | 35-54 | 55+ | non-smokers | smokers | ||
| Tobacco control in Russia | Adequate | 18.2% | 14.4% | 20.8% | 19.6% | 11.6% | 22.6% | 10.2% | 12.4% | 12.0% | 6.2% | 8.2% | 20.7% |
| Insufficient | 38.3% | 35.5% | 39.0% | 41.7% | 41.1% | 36.5% | 42.1% | 40.8% | 47.6% | 37.1% | 41.7% | 44.0% | |
| Nothing is done | 33.7% | 40.2% | 32.0% | 26.5% | 40.4% | 29.3% | 38.7% | 40.0% | 33.2% | 43.8% | 40.4% | 30.3% | |
| Tobacco prices (effect of taxation) | Should increase faster than inflation | 18.1% | 19.7% | 16.5% | 18.4% | 27.8% | 11.7% | 24.0% | 23.3% | 21.3% | 27.8% | 26.8% | 10.3% |
| Should increase in accordance with inflation | 22.9% | 20.4% | 23.6% | 25.8% | 26.0% | 20.9% | 19.8% | 23.0% | 20.8% | 15.7% | 19.5% | 20.8% | |
| Should not increase | 51.9% | 52.3% | 54.8% | 46.3% | 37.4% | 61.6% | 40.5% | 42.7% | 44.2% | 34.3% | 36.3% | 61.7% | |
| Ban of sales in kiosks | Yes | 63.2% | 57.7% | 63.3% | 72.2% | 72.5% | 57.1% | 76.4% | 71.6% | 76.6% | 80.5% | 78.5% | 66.1% |
| No | 30.9% | 35.5% | 32.6% | 20.5% | 20.4% | 37.9% | 15.3% | 19.6% | 15.7% | 11.2% | 12.5% | 29.6% | |
| Health warnings (% agreeing, multiple responses possible) | Should include pictures | 27.0% | 21.2% | 31.0% | 29.4% | 30.6% | 24.6% | 32.5% | 29.7% | 33.6% | 33.9% | 33.4% | 28.2% |
| Should have larger text warnings | 24.6% | 24.0% | 23.0% | 28.1% | 28.0% | 22.3% | 27.0% | 26.3% | 25.1% | 29.7% | 27.5% | 24.1% | |
| Are adequate | 50.7% | 56.6% | 49.0% | 44.4% | 46.1% | 53.8% | 39.4% | 43.0% | 58.3% | 66.4% | 37.6% | 48.8% | |
| Should smoking be restricted in films and on television | Yes | 64.9% | 56.8% | 66.4% | 74.8% | 76.4% | 57.2% | 73.9% | 64.2% | 75.9% | 80.2% | 76.9% | 58.3% |
| No | 26.0% | 34.5% | 23.9% | 16.0% | 13.8% | 34.2% | 14.7% | 21.6% | 13.6% | 9.6% | 11.5% | 31.2% | |
Note: Those responding “difficult to say” not reported so columns may not sum to 100%
56% overall believed that existing health warnings (currently 4% on front and back of the pack, without specifying framing or colours) were inadequate, with a third favouring pictorial warnings and a quarter larger text. Support for improved warnings was greater among non-smokers. There was considerable support for restrictions on smoking in films and television, especially among older people and non-smokers.
At present, most Russian bars and restaurants, to the extent that they limit smoking at all, designate a few tables in the worst areas as non-smoking. This was supported by less than 10% of respondents (Table 3). Furthermore, even among smokers, less than one in five supported current policy or no restrictions at all. Almost a third supported a total ban, with 44% supporting provision of equal space for smokers and non-smokers. Support for a total ban was higher among women and non-smokers. Currently smoking in public transport is limited to designated areas but this is not enforced in taxis and trains. In buses and similar forms of transport drivers are allowed to smoke, even if the driver's cabin is not isolated from the public part of the carriage. The majority of respondents (almost 60%) favoured a total ban in all forms of public transport, a policy supported by 45% of smokers. Although many Russian doctors smoke, a clear majority of respondents felt it was inappropriate for them to smoke in the presence of a patient.
Table 3.
Attitudes to smoking bans
| Male | Female | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 18-34 | 35-54 | 55+ | non-smokers | smokers | All | 18-34 | 35-54 | 55+ | non-smokers | smokers | ||
| Support for ban in restaurants | Total ban | 26.1% | 21.1% | 24.9% | 36.0% | 36.9% | 18.8% | 38.1% | 27.6% | 39.6% | 45.9% | 41.0% | 23.6% |
| Provision of equal smoking/non-smoking areas | 46.3% | 49.9% | 46.9% | 39.7% | 39.8% | 50.7% | 42.2% | 54.7% | 43.1% | 29.8% | 39.1% | 57.9% | |
| Provision of small non-smoking area | 12.0% | 16.6% | 11.4% | 5.6% | 10.1% | 13.3% | 7.9% | 8.2% | 10.0% | 5.3% | 7.0% | 12.5% | |
| No ban | 4.9% | 4.5% | 6.5% | 3.0% | 2.4% | 6.7% | 1.4% | 2.5% | 0.6% | 1.2% | 1.1% | 2.6% | |
| Support for ban in public transport | Total ban | 51.9% | 44.5% | 54.4% | 59.2% | 64.7% | 43.3% | 65.7% | 55.5% | 64.5% | 76.4% | 68.7% | 51.1% |
| Smoking in designated places | 38.5% | 45.2% | 38.8% | 27.6% | 27.5% | 45.9% | 28.4% | 37.3% | 30.7% | 17.8% | 25.8% | 41.7% | |
| No change from current | 3.7% | 4.2% | 3.0% | 4.0% | 1.7% | 5.0% | 1.7% | 2.6% | 1.4% | 1.1% | 0.9% | 5.3% | |
| is it acceptable for doctor to smoke in presence of patient | No | 64.7% | 65.5% | 60.6% | 70.4% | 73.0% | 59.1% | 74.7% | 68.7% | 73.9% | 80.9% | 77.4% | 61.1% |
| Yes, but not on duty | 18.3% | 15.0% | 24.0% | 1.4% | 12.9% | 21.9% | 11.1% | 14.2% | 12.3% | 7.0% | 9.5% | 19.1% | |
| Yes, in smoking area | 13.0% | 14.9% | 12.6% | 10.6% | 9.2% | 15.5% | 10.4% | 13.6% | 9.8% | 8.0% | 9.0% | 17.1% | |
Note: Those responding “difficult to say” not reported so columns may not sum to 100%
The overwhelming majority of respondents were aware that nicotine is addictive, although smokers tended to see it as less addictive than non-smokers (Table 4). 13% of smokers reported believing that smoking would not shorten their life expectancy but overall the fact that it would was recognized by respondents, although many underestimated the magnitude of the effect. A clear majority of respondents recognized the harmful nature of second hand smoke, even among smokers although smokers underestimated impacts compared with non-smokers. A third of smokers thought that “light” cigarettes were safer than standard ones.
Table 4.
Health beliefs
| Male | Female | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 18-34 | 35-54 | 55+ | non-smokers | smokers | All | 18-34 | 35-54 | 55+ | non-smokers | smokers | ||
| Is nicotine addictive? | Yes, like illicit drugs | 37.0% | 36.0% | 38.1% | 36.8% | 42.3% | 33.5% | 46.7% | 44.1% | 43.3% | 52.9% | 48.2% | 39.3% |
| Yes, but less than illicit drugs | 49.0% | 46.6% | 50.9% | 49.9% | 43.7% | 52.6% | 42.2% | 44.7% | 45.2% | 36.7% | 41.1% | 48.2% | |
| Yes, but easily overcome | 8.1% | 9.8% | 6.6% | 7.9% | 8.7% | 7.6% | 5.7% | 7.3% | 7.4% | 2.3% | 4.9% | 10.0% | |
| No | 3.0% | 4.3% | 2.7% | 1.7% | 0.9% | 4.5% | 1.1% | 0.3% | 1.2% | 1.7% | 1.1% | 1.3% | |
| Does smoking shorten life? | No | 10.0% | 11.4% | 8.9% | 9.7% | 6.3% | 12.5% | 5.8% | 6.9% | 5.6% | 5.1% | 4.0% | 15.1% |
| Yes, only for people with cancer | 4.6% | 4.3% | 5.1% | 4.3% | 3.7% | 5.2% | 3.7% | 4.9% | 2.6% | 3.8% | 3.6% | 4.1% | |
| Yes, by 1-2 years | 12.7% | 12.5% | 15.1% | 8.8% | 8.5% | 15.5% | 9.1% | 14.7% | 9.1% | 3.9% | 6.9% | 20.0% | |
| Yes, by 3-5 years | 33.3% | 33.8% | 32.8% | 33.4% | 35.0% | 32.2% | 33.5% | 30.4% | 35.4% | 34.1% | 34.6% | 27.8% | |
| Yes, by more than 5 years | 24.3% | 21.0% | 24.9% | 28.5% | 35.7% | 16.7% | 34.6% | 28.8% | 34.5% | 39.9% | 37.8% | 18.4% | |
| Second hand smoke: | Severely harmful to adults and children | 60.7% | 57.8% | 62.9% | 61.6% | 71.8% | 53.3% | 75.3% | 68.9% | 75.2% | 81.4% | 77.3% | 65.4% |
| Harmful only for some people if exposure heavy | 20.0% | 20.8% | 19.6% | 19.6% | 17.2% | 21.9% | 14.8% | 18.7% | 16.5% | 9.3% | 13.5% | 21.3% | |
| Affects health but only slightly | 11.4% | 12.9% | 11.1% | 9.6% | 5.8% | 15.2% | 5.8% | 7.6% | 5.8% | 4.1% | 4.8% | 10.6% | |
| No harm | 3.1% | 4.1% | 2.6% | 2.4% | 0.7% | 4.7% | 0.8% | 1.1% | 0.6% | 0.7% | 0.6% | 1.4% | |
| Light cigarettes safer than regular ones | Percentage yes | 28.9% | 28.4% | 31.3% | 25.5% | 22.3% | 33.3% | 20.7% | 28.0% | 19.6% | 15.3% | 18.4% | 32.5% |
Note: Those responding “difficult to say” not reported so columns may not sum to 100%
The majority of respondents knew that smoking caused lung cancer (Table 5) but a surprising number, even among non-smokers, did not. Knowledge of its impact on other conditions, such as heart disease (where only 53% of smokers recognised a link) and, especially, impotence (around 9% of smokers), was poor.
Table 5.
Smoking is a cause of...
| Male | Female | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 18-34 | 35-54 | 55+ | non-smokers | smokers | All | 18-34 | 35-54 | 55+ | non-smokers | smokers | |
| Heart disease | 53.9% | 53.5% | 50.7% | 60.0% | 54.8% | 53.2% | 57.8% | 46.7% | 40.9% | 39.5% | 58.8% | 53.0% |
| Stroke | 33.8% | 32.7% | 34.6% | 34.1% | 36.5% | 32.0% | 39.4% | 33.5% | 42.8% | 40.9% | 40.4% | 34.1% |
| Lung cancer | 77.6% | 74.6% | 78.3% | 81.4% | 82.5% | 74.4% | 84.4% | 78.8% | 86.1% | 87.6% | 85.8% | 77.7% |
| Bronchitis | 47.3% | 45.1% | 47.4% | 50.6% | 52.6% | 43.7% | 55.6% | 56.1% | 54.6% | 56.2% | 56.8% | 49.6% |
| Dental caries | 18.9% | 21.5% | 18.2% | 15.8% | 24.1% | 15.3% | 21.9% | 25.3% | 21.5% | 19.5% | 21.9% | 22.3% |
| Impotence | 10.4% | 11.8% | 11.3% | 6.7% | 12.9% | 8.8% | 13.0% | 12.7% | 14.4% | 11.8% | 13.8% | 9.4% |
| Diabetes | 6.4% | 5.4% | 6.3% | 8.0% | 9.1% | 4.6% | 11.1% | 8.6% | 12.8% | 11.5% | 11.9% | 7.1% |
Note: Those responding “difficult to say” not reported so columns may not sum to 100%
The tobacco companies were generally viewed as behaving like most other companies in Russia. Very few respondents viewed them as behaving unethically and there was very little awareness of their involvement in illegal activities such as smuggling (Table 6). The vast majority of people thought that they definitely or maybe bribed politicians.
Table 6.
Attitudes to tobacco industry
| Male | Female | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 18-34 | 35-54 | 55+ | non-smokers | smokers | All | 18-34 | 35-54 | 55+ | non-smokers | smokers | ||
| Are Tobacco Companies socially responsible? | Yes, like other large corporations | 28.1% | 25.3% | 31.4% | 26.7% | 34.0% | 24.2% | 28.7% | 32.9% | 26.0% | 28.0% | 29.7% | 23.7% |
| Yes, in some ways | 23.8% | 28.4% | 19.2% | 24.4% | 15.5% | 29.4% | 19.5% | 23.1% | 20.4% | 15.4% | 18.6% | 24.4% | |
| In business, profits come first | 28.0% | 26.6% | 30.6% | 25.7% | 30.0% | 26.6% | 23.8% | 23.4% | 24.0% | 23.9% | 22.2% | 31.4% | |
| They are unethical | 3.5% | 3.1% | 4.3% | 2.6% | 4.3% | 3.0% | 6.3% | 5.0% | 7.9% | 5.6% | 7.1% | 2.1% | |
| They act illegally | 1.7% | 1.1% | 2.3% | 1.8% | 1.8% | 1.7% | 1.8% | 1.9% | 2.0% | 1.4% | 2.1% | 0.0% | |
| Industry bribes politicians and officials | Yes | 19.5% | 16.4% | 21.7% | 20.8% | 20.6% | 18.8% | 14.7% | 1.2% | 13.7% | 18.4% | 14.8% | 14.2% |
| Maybe | 53.0% | 53.7% | 51.6% | 54.3% | 53.0% | 53.0% | 52.9% | 54.0% | 55.6% | 49.0% | 53.5% | 50.3% | |
| No | 10.1% | 9.9% | 11.5% | 8.1% | 9.4% | 10.6% | 10.1% | 9.3% | 13.6% | 6.8% | 9.5% | 13.0% | |
Note: Those responding “difficult to say” not reported so columns may not sum to 100%
A composite score on attitudes to tobacco control was calculated as described above, with 0 indicating support for no action and 8 for all those considered. The distribution was normal, with a mean of 3 and standard deviation of 2. In a regression, with age group, self-reported social class, size of settlement, self-assessed economic status, sex, and smoking status, all entered into the equation, only age group (t=5.388, p<0.0001), smoking status (t=-10.466, p<0.0001) and settlement size (t=2.320, p=0.02) emerged as significantly associated with the score. The relationships with these variables are depicted in Figure 1.
Figure 1.
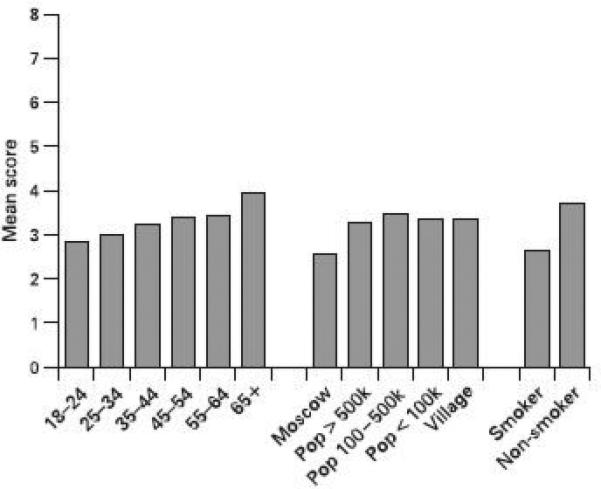
Support for action against smoking (mean scores, with 0= support for no action and 8=support for all actions)
Discussion
This study is, to our knowledge, the first to report publicly attitudes to tobacco control in a representative sample of the Russian population. While we would be surprised if the tobacco industry had not previously undertaken such surveys for its own internal use, we have so far been unable to locate any detailed reports, except for a single table from the Social Attitudes Tracking Study,18 conducted by the polling organization GfK sometime before 1997, on the on-line Legacy Tobacco Documents Library. This library contains over 8 million internal industry documents released in the process of litigation against the tobacco industry in the USA.19 The table indicates that a majority of Russian respondents were bothered by workplace smoking.
The survey has a number of limitations, largely consequent on financial constraints. These include a relatively small sample size, limiting the scope for detailed assessment of attitudes among sub-groups in the population, and the number of questions that could be asked. The sampling method, which is that used normally by polling agencies, allowed for substitution, and so could introduce some bias. This may explain the higher than expected frequency of smoking among older respondents. The effect of any such bias could be manifest in two ways. First, the respondents may be less supportive than the overall population of measures to curb smoking. This would imply that our findings of support for such measures may be conservative. Second, they may be less likely to be aware of the health risks of smoking, again rendering our findings of a considerable degree of ignorance about consequences such as heart disease an underestimate. Notwithstanding these caveats, it does provide a useful basis for the development of a contextually appropriate campaign to tackle smoking in a country where such activities have so far been extremely limited.
The need for action is highlighted by the remarkably high proportion of respondents who believe that there is no action to combat smoking in Russia. When these are added to those who believe that something is done but it is insufficient, it is apparent that support for effective action is compelling, even with the poor levels of understanding of the health impacts of smoking that the survey reveals. The respondents are, however, less clear about what should be done. This may reflect the relative paucity of popular debate in Russia so far about the evidence of effectiveness of different measures, although it may also capture a more general cynicism about the potential for the state to act effectively to promote health. In the Living Standards and Health survey,20 conducted in 2001, only 23% of respondents were definitely or quite satisfied with the performance of the Russian government (authors’ calculations).
The most effective areas of action in tobacco control are price increases, advertising bans and smokefree legislation. Space did not permit questions on advertising but even in the area of tobacco taxation, 40% of the population felt that cigarettes prices should increase.
There was also considerable support for an extension of existing restrictions on bans in smoking in public places although not yet majority support for a total ban on smoking in bars and restaurants. Interestingly, given the high rates of smoking, the level of support for a comprehensive ban was not far less than that seen prior to smokefree legislation in the United Kingdom and Ireland.21 Combined with evidence that support for such legislation increases after its implementation21 and with data from the survey indicating that a clear majority view second hand smoke as dangerous, this suggests that smokefree legislation in Russia may be feasible in the near future. As in other jurisdictions implementing such legislation, there will of course be a need to increase awareness of the health impacts of second hand smoke, drawing attention to evidence that has long been suppressed by the tobacco industry, 22 as well as countering misleading arguments by the industry suggesting that enhanced ventilation could offer a satisfactory alternative.23 It will be especially important to publicise the growing evidence of substantial falls in the incidence of myocardial infarction following the introduction of bans elsewhere.24
One area where there was overwhelming support was for a ban on sales of cigarettes from kiosks. These small stalls are ubiquitous on the streets of the former Soviet Union. A recent study conducted in Estonia found that they cater for many people living on the margins of society, selling mainly cigarettes, surrogate alcohols (aftershaves etc. for drinking), condoms, washing powder (possibly for cleaning needles), and pet food.25 While further research is necessary, they can be observed selling cigarettes individually and are believed to be a major source of sales to children. There was also much support for bans on smoking on television and films although it is unlikely that respondents were aware of the growing evidence of product placement by the tobacco industry26 and the clear link between exposure to images of smoking in films and initiation of smoking among adolescents.27
Levels of knowledge about the negative health consequences of smoking were poor particularly compared with levels recorded in the United States, United Kingdom, Canada and Australia where the proportion of those recognising a link with, for example, stroke and impotence were 2 to 3 times higher. 28 Interestingly, in contrast to the west, there was almost no difference in awareness by educational level. For example, the percentage believing that smoking caused heart disease was 56% among those with primary, 54.9% among those with secondary, and 59.3% among those with higher education (Χ2 = 0.389, NS) . This illustrates the need for improved anti-smoking education campaigns. These need not necessarily be expensive – large, graphic health warnings on cigarette packs produced at tobacco industry expense could for example play a key role as evidenced by Canada. 28,29 With under 50% of respondents in Russia considering current warnings adequate and approximately a third in support of pictorial warnings, such a change should be feasible in Russia. Poor levels of public understanding may also link to the high rates of smoking and lack of awareness among doctors in Russia. It is estimated that 66% of male doctors and 21% of female doctors are current or former smokers, than less than 10% doctors are familiar with the harm caused by tobacco use30 and that doctors who smoke are far less likely to advise their patients to quit (38% vs 58% of never smokers).31 This indicates that education of medical professionals is urgently needed.
Although nicotine is widely recognized as an addictive substance, it is likely that there is confusion about the role of nicotine in disease causation as this is seen even where knowledge of tobacco's health impacts is further advanced28. Future campaigns might usefully emphasise the scope for breaking the addiction using modern evidence-based therapy, with related work exploring how it can become more easily accessible in Russia. A substantial minority of respondents had been misled to think that “light” cigarettes were safer than standard ones. This is consistent with findings in other countries,32 reflecting the active promotion of this illusion by the tobacco industry. Given that the industry sees growth in “light” cigarettes as key to its success,33 and is increasingly promoting them in Russia, these results highlight the need to counter this view urgently in advocacy work.
Tobacco companies are generally viewed as similar to other companies. The perception among most respondents that they may bribe officials should be interpreted in the context of Russia's poor performance on corruption in assessments by Transparency International. In its 2007 Corruption Perception Index it ranked 143 out of 180 countries.34
The regression analysis demonstrated some differences within the Russian population that should be taken into account in future work to reduce smoking. The challenges are clearly greatest among young Russians and those living in Moscow, precisely the groups most intensively targeted by the tobacco industry.
Research from other countries has identified the importance of denormalising the industry,35,36 highlighting the unethical methods it uses to recruit children, its promotion of fraudulent research, and its involvement in illegal activities such as smuggling. These findings suggest that future anti-smoking advocacy might usefully seek to raise public awareness of the activities of the industry, drawing on experience of similar campaigns elsewhere.37
Effective advocacy and tobacco control policies must be based both on evidence of effectiveness and on an adequate understanding of the challenges that are being confronted. Although only a first step, the findings from this survey provide a valuable basis to move forward on tobacco control in Russia. They demonstrate that policy is lagging behind public expectations, although they also identify the need for greater public education to counter common misunderstandings.8 The high and increasing rates of smoking indicate that such improvements are urgently needed.
Acknowledgements
This research was supported by a grant from the Bloomberg Global Initiative on Tobacco Control. Additional support for AG and MM's work on tobacco policy in Russia is from the project “Globalisation, the tobacco industry and policy influence” funded by the US National Cancer Institute. AG is supported by a Health Foundation Clinician Scientist fellowship.
Footnotes
The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article (if accepted) to be published in Journal (insert name) editions and any other BMJPGL products to exploit all subsidiary rights, as set out in our licence (http://tc.bmj.com/ifora/licence.pdf).
Competing interests: none
References
- 1.Gilmore A, McKee M. Moving east: how the transnational tobacco companies gained entry to the emerging markets of the former Soviet Union. Part I: Establishing cigarette imports. Tobacco Control. 2004;13:143–150. doi: 10.1136/tc.2003.005108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gilmore A, McKee M. Moving east: how the transnational tobacco companies gained entry to the emerging markets of the former Soviet Union. Part II: an overview of priorities and tactics used to establish a manufacturing presence. Tobacco Control. 2004;13:151–160. doi: 10.1136/tc.2003.005207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gilmore A, McKee M. Tobacco and transition: an overview of industry investments, impact and influence in the former Soviet Union. Tobacco Control. 2004;13:136–142. doi: 10.1136/tc.2002.002667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McKee M, Bobak M, Rose R, Shkolnikov V, Chenet L, Leon D. Patterns of smoking in Russia. Tobacco Control. 1998;7:22–26. doi: 10.1136/tc.7.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gilmore A, Collin J, McKee M. British American Tobacco's erosion of health legislation in Uzbekistan. British Medical Journal. 2006;332:355–358. doi: 10.1136/bmj.332.7537.355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Danishevski K, McKee M. Campaigners fear that Russia's new tobacco law won't work. BMJ. 2002;324:382. doi: 10.1136/bmj.324.7334.382/a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ross H, Shariff S, Gilmore A. Economics of Tobacco Taxation in Russia. Bloomberg Initiative to Reduce Tobacco Use; Baltimore, MD: Forthcoming. [Google Scholar]
- 8.Perlman F, Bobak M, Gilmore A, McKee M. Trends in the prevalence of smoking in Russia during the transition to a market economy. Tobacco Control. 2007;16:299–305. doi: 10.1136/tc.2006.019455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gilmore AB. Believe it or not: growth continues on Russia market.. Tobacco industry strategies and smoking trends in the former Soviet Union. Summit of tobacco control leaders from Central and Eastern Europe and the Former Soviet Union countries; Warsaw. 22nd April 2008. [Google Scholar]
- 10.Gay G. Bullish about the bear. Tobacco Reporter. 2006 Sep;:24–28. [Google Scholar]
- 11.Gay G. Most Dynamic. Tobacco Reporter. 2007 Oct;:34–6. [Google Scholar]
- 12.World Health Organisation . Health for All database. WHO; Copenhagen: 2007. [Google Scholar]
- 13. [11th May 2008];Deaths from Smoking. URL: http://www.deathsfromsmoking.net/countries.html.
- 14.Bobak M, Marmot M. East-West mortality divide and its potential explanations: proposed research agenda. BMJ. 1996;312:421–5. doi: 10.1136/bmj.312.7028.421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Marquez P, Suhrcke M, McKee M, Rocco L. Adult Health in Russia – More than Just a Health Problem? Health Affairs. 2007;26:1040–1051. doi: 10.1377/hlthaff.26.4.1040. [DOI] [PubMed] [Google Scholar]
- 16.Gilmore A, McKee M. Moving east: how the transnational tobacco companies gained entry to the emerging markets of the former Soviet Union. Part I: Establishing cigarette imports. Tobacco Control. 2004;13:143–150. doi: 10.1136/tc.2003.005108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. [16th March 2008]; URL: http://www.levada.ru/express02.html.
- 18.GfK Great Britain. Social Attitudes Tracking Study - Russia (undated) Bates Number 2065261105. [Google Scholar]
- 19. [16th March 2008]; URL: http://legacy.library.ucsf.edu/
- 20.Gilmore A, Pomerleau J, McKee M, Rose R, Haerpfer CW, Rotman D, Tumanov S. Prevalence of Smoking in 8 Countries of the Former Soviet Union: Results from the Living Conditions, Lifestyles and Health Study. Am J Public Health. 2004;94:2177–2187. doi: 10.2105/ajph.94.12.2177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fong GT, Hyland A, Borland R, Hammond D, Hastings G, McNeill A, Anderson S, Cummings KM, Allwright S, Mulcahy M, Howell F, Clancy L, Thompson ME, Connolly G, Driezen P. Reductions in tobacco smoke pollution and increases in support for smoke-free public places following the implementation of comprehensive smoke-free workplaces legislation in the Republic of Ireland: findings form the ITC Ireland/UK survey. Tobacco Control. 2005;15(Suppl 3):1–8. doi: 10.1136/tc.2005.013649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Diethelm PA, Rielle J-C, McKee M. The whole truth and nothing but the truth? The research that Philip Morris did not want you to see. Lancet. 2005;366:86–92. doi: 10.1016/S0140-6736(05)66474-4. [DOI] [PubMed] [Google Scholar]
- 23.Drope J, Bialous SA, Glantz SA. Tobacco industry efforts to present ventilation as an alternative to smoke-free environments in North America. Tob Control. 2004;13(Suppl 1):i41–7. doi: 10.1136/tc.2003.004101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dinno A, Glantz S. Clean indoor air laws immediately reduce heart attacks. Prev Med. 2007;45:9–11. doi: 10.1016/j.ypmed.2007.03.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pärna K, Lang K, Raju K, Väli K, McKee M. A rapid situation assessment of the market for surrogate and illegal alcohols in Tallinn, Estonia. Int J Public Health. 2007;52:402–410. doi: 10.1007/s00038-007-6112-z. [DOI] [PubMed] [Google Scholar]
- 26.Glantz SA, Kacirk KW, McCulloch C. Back to the future: Smoking in movies in 2002 compared with 1950 levels. Am J Public Health 2004. 94:261–3. doi: 10.2105/ajph.94.2.261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Song AV, Ling PM, Neilands TB, Glantz SA. Smoking in movies and increased smoking among young adults. Am J Prev Med. 2007;33:396–403. doi: 10.1016/j.amepre.2007.07.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Siapush M, McNiell A, Hammond D, Fong GT. Socieoeconomic and country variations in knowledge of health risks of tobacco smoker and toxic constituents of smoke: results from the 2002 International Tobacco Control (ITC) four country survey. Tobacco Control 2006. 15:65–70. doi: 10.1136/tc.2005.013276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hammond D, Fong GT, McNeill A, Borland R, Cummings M. Effectiveness of cigarette warning labels in informing mokers about the risks of smoking: evidence from the International Tobacco Control (ITC) four country survey. Tobacco Control. 2006;15(Suppl III):iii19–iii25. doi: 10.1136/tc.2005.012294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Danishevski K. [Kurenie I medicina, imeut li pravo vrachi umit’ ruki]. “Smoking and healthcare: can doctors “wash their hands””. Open Health Institute; Moscow: 2005. [11th May 2008]. URL: http://www.publichealth.ru/docs/Tobacco&docsDanishevski.pdf. [Google Scholar]
- 31.Levshin V. [11th May 2008];Smoking cessation program motivates Russian physicians to assist their patients and themselves. 2005 URL: http://www.ceche.org/communications/russian-cancer-cen/html.
- 32.Kozlowski LT, Goldberg ME, Yost BA, White EL, Sweeney CT, Pillitteri JL. Smokers' misperceptions of light and ultra-light cigarettes may keep them smoking. Am J Prev Med. 1998;15:9–16. doi: 10.1016/s0749-3797(98)00004-x. [DOI] [PubMed] [Google Scholar]
- 33.Gilmore A, Collin J, Cartwright S. World leader or also ran, paragon or pariah? The future of BAT.. European Conference on Tobacco or Health; Basel. 2007. [Google Scholar]
- 34. [11th May 2008]; URL: http://www.transparency.org/policy_research/surveys_indices/cpi/2007/faq.
- 35.Hammond D, Fong GT, Zanna MP, Thrasher JF, Borland R. Tobacco denormalization and industry beliefs among smokers from four countries. Am J Prev Med. 2006;31:225–32. doi: 10.1016/j.amepre.2006.04.004. [DOI] [PubMed] [Google Scholar]
- 36.Leatherdale ST, Sparks R, Kirsh VA. Beliefs about tobacco industry (mal)practices and youth smoking behaviour: insight for future tobacco control campaigns (Canada). Cancer Causes Control. 2006;17:705–11. doi: 10.1007/s10552-006-0004-z. [DOI] [PubMed] [Google Scholar]
- 37.Sly DF, Trapido E, Ray S. Evidence of the dose effects of an antitobacco counteradvertising campaign. Prev Med. 2002;35:511–8. doi: 10.1006/pmed.2002.1100. [DOI] [PubMed] [Google Scholar]