

Children under the age of one year (i.e. infants) with acute myeloid leukemia (AML) represent a distinct subgroup of patients with peculiar clinical and biological characteristics.1 As compared to older children, a higher prevalence of unfavorable clinical and cytogenetic/molecular features has frequently been reported in this age group.1,2 While the outcome of infants with acute lymphoblastic leukemia is still worse than that of older children,3 in recent years, this may not be the case for infants with AML. In particular, consistent with the significant progress generally achieved in the outcome of childhood AML,1 the event-free survival (EFS) of infants with AML has increased from less than 35% in the past4 to more than 50% in recently published studies.5 It is unclear whether and to what extent a wide use of allogeneic (ALLO) hematopoietic stem cell transplantation (HSCT) in first complete remission (CR), has contributed to the improved outcome of these particular patients. In the AML 2002/01 study of the Associazione Italiana di Ematologia e Oncologia Pediatrica (AIEOP)6, infants achieving CR1 were most often offered either allo-HSCT or, less frequently, autologous (auto)-HSCT as post-remission therapy. Here we report clinical/biological characteristics, as well as outcome, of infants, comparing the results with those of older children treated in that protocol. We analyzed children aged one year or under year at diagnosis, with de novo non-promyelocytic AML, treated between December 2002 and June 2011 according to the AIEOP AML 2002/01 protocol; children with Down syndrome were not included in this study as they were treated with a specific protocol (i.e. AIEOP AML 2002/02). Details on the diagnostic workup, as well as on the cytogenetic/molecular characterization, have been reported elsewhere.6
Infants of the AIEOP AML 2002/01 study6 received two courses of induction chemotherapy, including idarubicin, Ara-C and etoposide (see Pession et al.6 for details). Children achieving CR received two consolidation courses, containing high-dose (HD) Ara-C, combined with either etoposide or mitoxantrone in the first and second course, respectively. The dosage of cytotoxic drugs was adapted for infants according to the following formula: weight (kg) × dose (× m2)/30, the only exception being represented by the dose of HD-Ara-C, administered as 20%, 30%, 40%, 50% and 60% to infants aged under 3, 4–5, 6–7, 8–10 and 11–12 months, respectively, in view of the reduced Ara-C clearance of these patients.7 At the end of consolidation, infants carrying t(8:21), inv(16) or t(16;16) (standard risk group) received a fifth course of HD Ara-C. The remaining high-risk (HR) infants were offered allo-HSCT from either matched family donors (MFD) or alternative donors. In 7 children lacking a matched related or matched unrelated donor, the treating physician decided not to perform an allograft, but opted for auto-HSCT.
Infants’ clinical and biological features at presentation, compared with those of other age groups, are detailed in Table 1. Compared to older children, infants had significantly more central nervous system involvement at diagnosis (P=0.002) (Table 1). French-American-British (FAB) subtypes M1 (P=0.042) and M2 (P<0.001) were more common in older children, while infants presented more frequently with a FAB-M5 (P=0.008) or M7 subtype (P<0.001). In comparison to older children, infants were allocated more frequently to the HR group (P=0.001) (see Pession et al.6 for details).
Table 1.
Clinical, cytogenetic and biological features of infants enrolled in the AIEOP AML 2002/01 protocol compared with those of older patients.
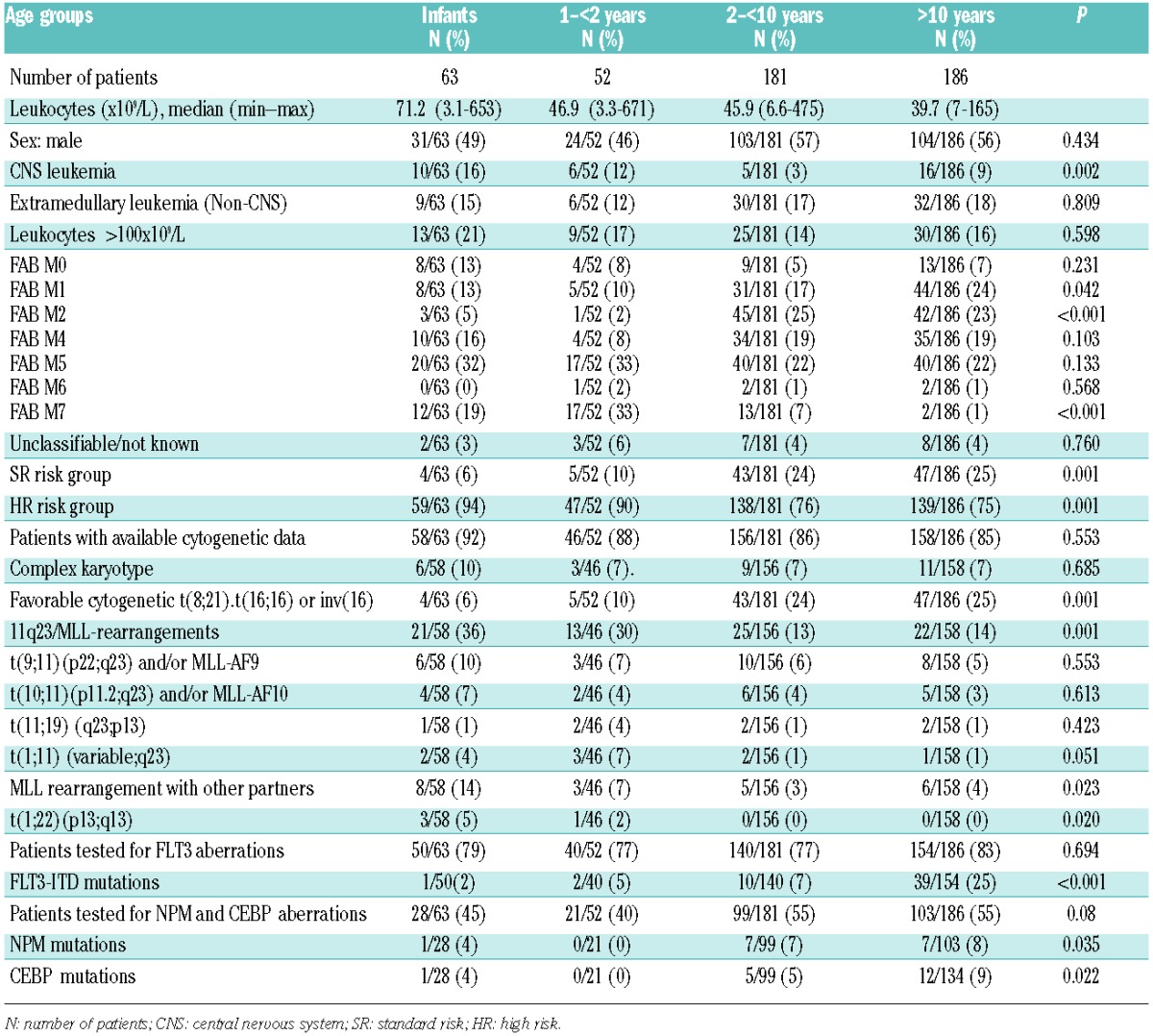
Infants showed a significantly higher incidence (i.e. 36%) of 11q23/MLL rearrangements (P=0.001) than older children. All cases with t(1;22)(p13;q13) but one were infants belonging to the FAB-M7 subtype (Table 1). FLT-3 aberrations, namely internal tandem duplication and activating loop mutations, were present only in 2% and 5% of patients aged under one year and those aged one to under two years, respectively, while they were found in 7–25% of older children (P=0.001). Notably, 6 (9.5%) out of the 63 infants harbored inv(16)(p13.3q24.3) encoding for the cryptic fusion transcript CBFA2T3-GLIS2 that we identified through whole-transcriptome sequencing and confirmed using Sanger techniques; 4 of them had a FAB-M7 blast morphology.8 This cryptic translocation is much less common than the classical inversion of chromosome 16 and can be detected only by specific molecular/cytogenetic probes.8,9
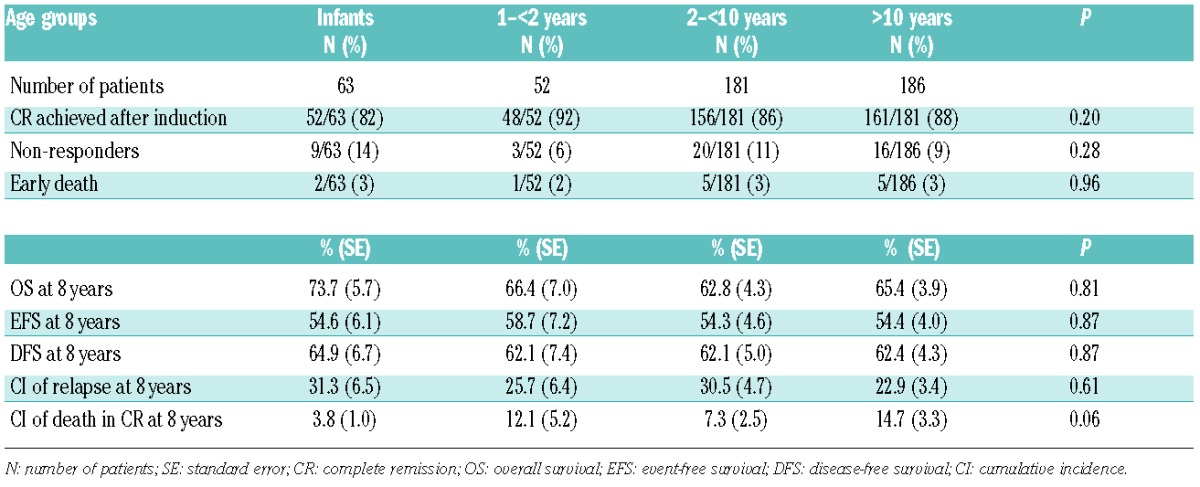
Results of the outcome of infants compared to those of other age groups are reported in Table 2. CR, early death and induction failure rates were 82%, 3% and 14%, respectively, with no statistical difference to rates for older patients. Only 3 infants died in CR: 2 during consolidation due to Gram-negative sepsis and one after transplantation. Compared to older children, severe mucositis occurred less frequently in infants (25% vs. 35%, respectively) (P=0.04), while the incidence of the remaining chemotherapy-related toxicities was superimposable. The cumulative incidence of relapse was 31%.
Table 2.
Outcome results of infants enrolled in the AIEOP AML 2002/01 protocol compared with older patients.
Four patients were not offered HSCT as they carried a favorable cytogenetic profile. All these 4 children are alive and disease free.
Forty-six infants out of 63 received HSCT in CR1: 7 children were given auto- and 39 allo-HSCT. With a median follow up of 57 months (range 12–130 months), the 8-year overall survival (OS) and EFS probabilities of the whole population of infants were 74% (Standard Error (SE) 5.7) and 55% (SE 6.4), respectively, showing no difference to those of other age groups (Table 2). In multivariate analysis, only blast count over 5% at time of hematologic recovery after induction negatively affected prognosis (P=0.03).
Overall survival and EFS of infants undergoing HSCT in CR1 was 72% (SE 6.8) and 58% (SE 7.1), respectively. Neither type of donor nor stem cell source influenced the probabilities of OS and EFS in allo-HSCT recipients (data not shown). Notably, the small group of infants harboring the CBFA2T3-GLIS2 fusion transcript had a significantly worse prognosis (EFS 32.3%, SE 19.2) compared with CBFA2T3-GLIS2 negative infants (59.6%, SE 6.6) (P<0.05). Outcome of infants was not influenced be the presence of 11q23 MLL rearrangement (data not shown). Among transplanted infants, 14% experienced growth deficiency, 3% decreased cardiac function, 9% hypothyroidism and 6% have impaired cognitive function.
Besides confirming and extending previously reported observations, our data demonstrate for the first time that, in infants, CBFA2T3-GLIS2 fusion transcript seems to be as frequent as OTT-MAL fusion in FAB-M7 AML, this lesion predicting a grim prognosis. Moreover, our results suggest that a treatment strategy combining intensive chemotherapy and a widespread use of HSCT in CR1 is able to abolish the impact of unfavorable prognostic characteristics of infants. The outcome of our patients is similar to that reported by the I-BFM,2 MRC10 and Japanese groups,5 in which, however, HSCT was not widely used. In the new AIEOP-AML study, post-remission treatment will be tailored to reduce the proportion of transplanted infants with predicted disease recurrence, in view of the more frequent and severe HCST-related long-term complications.11
Footnotes
Funding: this work was supported in part by grants from Fondazione Ginevra Caltagirone and Fondazione Umberto Veronesi (Milan) (RM), by Banca Popolare di Milano (AP) and by Associazione Italiana Ricerca sul Cancro (AIRC) Special Project 5 × mille #9962 (FL).
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Creutzig U, van den Heuvel-Eibrink MM, Gibson B, Dworzak MN, Adachi S, de Bont E, et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood. 2012;120(16):3187–205 [DOI] [PubMed] [Google Scholar]
- 2.Creutzig U, Zimmermann M, Bourquin J-P, Dworzak MN, Kremens B, Lehrnbecher T, et al. Favorable outcome in infants with AML after intensive first- and second-line treatment: an AML-BFM study group report. Leukemia. 2012;26(4):654–61 [DOI] [PubMed] [Google Scholar]
- 3.Pieters R. Infant acute lymphoblastic leukemia: Lessons learned and future directions. Curr Hematol Malig Rep. 2009;4(3):167–74 [DOI] [PubMed] [Google Scholar]
- 4.Pui CH, Raimondi SC, Srivastava DK, Tong X, Behm FG, Razzouk B, et al. Prognostic factors in infants with acute myeloid leukemia. Leukemia. 2000;14(4):684–7 [DOI] [PubMed] [Google Scholar]
- 5.Kawasaki H, Isoyama K, Eguchi M, Hibi S, Kinukawa N, Kosaka Y, et al. Superior outcome of infant acute myeloid leukemia with intensive chemotherapy: results of the Japan Infant Leukemia Study Group. Blood. 2001;98(13):3589–94 [DOI] [PubMed] [Google Scholar]
- 6.Pession A, Rondelli R, Basso G, Rizzari C, Testi AM, Fagioli F, et al. Treatment and long-term results in children with acute myeloid leukaemia treated according to the AIEOP AML protocols. Leukemia. 2005;19(12):2043–53 [DOI] [PubMed] [Google Scholar]
- 7.Periclou AP, Avramis VI. NONMEM population pharmacokinetic studies of cytosine arabinoside after high-dose and after loading bolus followed by continuous infusion of the drug in pediatric patients with leukemias. Cancer Chemother Pharmacol. 1996;39(1–2):42–50 [DOI] [PubMed] [Google Scholar]
- 8.Masetti R, Pigazzi M, Togni M, Astolfi A, Indio V, Manara E, et al. CBFA2T3-GLIS2 fusion transcript is a novel common feature in pediatric, cytogenetically normal AML, not restricted to FAB M7 subtype. Blood. 2013;121(17):3469–72 [DOI] [PubMed] [Google Scholar]
- 9.Gruber TA, Larson Gedman A, Zhang J, Koss CS, Marada S, Ta HQ, et al. An Inv(16)(p13.3q24.3)-encoded CBFA2T3-GLIS2 fusion protein defines an aggressive subtype of pediatric acute megakaryoblastic leukemia. Cancer Cell. 2012;22(5):683–97 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Webb DK, Harrison G, Stevens RF, Gibson BG, Hann IM, Wheatley K; MRC Childhood Leukemia Working Party. Relationships between age at diagnosis, clinical features, and outcome of therapy in children treated in the Medical Research Council AML 10 and 12 trials for acute myeloid leukemia. Blood. 2001;98(6):1714–20 [DOI] [PubMed] [Google Scholar]
- 11.Baker KS, Bresters D, Sande JE. The burden of cure: long-term side effects following hematopoietic stem cell transplantation (HSCT) in children. Pediatr Clin North Am. 2010;57(1):323–42 [DOI] [PubMed] [Google Scholar]