

Abstract
Background
Ischemia-modified albumin (IMA) is a sensitive marker of ischemic event. However, limited studies are available regarding role of IMA in acute ischemic stroke (AIS).
Purpose
The aim of this study was to evaluate time course of IMA in AIS patient to validate its prognostic value.
Methods
IMA level was estimated in serum samples collected from five AIS patients at admission, 24hrs, 48hrs, 72hrs, and 144hrs after admission and also from five control subjects.
Results
There was significant (p<0.05) increase in IMA level in AIS samples at admission, 24hrs, 48hrs and 144hrs respectively when compared with control. On comparing IMA levels in follow up AIS samples with that of admission value we found that it decreased in follow-up samples till 72hrs, and significant (p<0.05) decrease was observed at 24hrs and 72hrs.
Conclusion
Findings shows that follow up estimation of IMA level in AIS may help in the prediction of the clinical status and outcome.
Keywords: Acute ischemic stroke, Prognosis, Ischemia modified albumin, Biomarker, Serum marker
Introduction
Acute ischemic stroke (AIS) is the leading cause of death worldwide and one of the main causes of long-term disability.1 Biomarkers which help in outcome prediction and therapeutic decision makings are very important in the management of AIS patients and reducing mortality rates.2,3 Oxidative stress is proposed as a fundamental mechanism of brain damage in ischemic and hemorrhagic stroke.4 Earlier it was reported that free radical alters the N-terminus of albumin which decreases its binding capacity for metals and is termed as Ischemia-modified albumin (IMA).5 Further, IMA was reported to be a sensitive marker of ischemic events.6,7 Recently it was found that IMA increases cerebrovascular diseases and may serve as a biomarker for early identification of acute stroke.8 Despite all the available information, there is little information regarding the use of IMA for prognosis of AIS. Therefore, the current study was done for prognostic evaluation of time course of serum level of IMA in AIS patients.
Methods
Subjects
Five patients, aged 48 ± 20 years, admitted consecutively in Central India Institute of Medical Sciences, Nagpur, India, within 24 hrs of onset of symptoms of AIS were included in the present study. Diagnosis was based on WHO definition of stroke. CT scan was performed in all the cases for the confirmation of acute stroke. Patients with transient ischemic attacks and other types of brain injury were excluded from the present study. Neurological deficit was assessed as per National Institute of Health Stroke Scale (NIHSS) score during the hospitalization period and functional recovery was assessed by Modified Rankin scale (mRS) at the time of discharge. All the patients were kept in the Intensive Care Unit (ICU), where the ambient temperature was between 20° - 25°C. All patients received standard medical treatment which included anti-platelet agents (aspirin 150 mg, clopidregel 75 mg once a day); anti-edema measures mannitol 20%, 0.25–0.5 g/kg over 20 min, (not exceeding a total of 2 g/kg of body weight in 24 h) in patients with symptoms of raised intracranial pressure, and other supportive therapy for the treatment of concurrent illnesses such as hypertension and diabetes mellitus. One patient was thrombolysed using intravenous recombinant tissue-plasminogen activator. The protocol of this study was reviewed and approved by the Institutional Ethics Committee of Central India Institute of Medical Sciences, Nagpur.
Sample collection
Serum samples from AIS patients were collect immediately at the time of admission (0’hrs), 24hrs, 48hrs, 72hrs and 144hrs after admission. Blood sample from age and sex-matched healthy individuals (n = 5) were also taken as control group. All the specimens for analysis of IMA were stored at —80°C until used.
Analysis of ischemia-modified albumin in serum sample
IMA was measure by the colorimetric method as described by Bar-Or et al.6 Briefly, 200 μL of serum samples were placed separately in two glass tubes (i.e. experimental and control). In the experimental set, 50 μL of 0.1% CoCl2•6H2O was added. After gentle shaking, this was left for 10 minutes to ensure sufficient cobalt albumin binding. Then 50 μL of 1.5 mg/mL dithiotheitol (DTT) was added as a coloring agent. After 2 minutes, 1 mL of 0.9% NaCl was added to halt the binding between the cobalt and albumin. The procedure in the control set was similar to experimental sets, except that 50 μL of distilled water was used instead of 50 μL of 1.5 mg/mL DTT. Color formation in experimental sets was analyzed in comparison to respective control sets at 470 nm under UV-VIS spectrophotometer (Systronic, India) and results were expressed in absorbance units (ABSU).
Statistical analysis
Statistical analysis was performed using the MedCalc (Statistical software version10). Repeated measure ANOVA was used to detect the difference of IMA among control and follow-up serum samples from stroke patients. P-value <0.05 was considered as statistically significant
Results
Five patients (age, 48 ± 20 years) of AIS were included in the study. The general characteristics of the all 5 patients are shown in Table 1. IMA level in individual samples from follow-up AIS patients and control group are depicted in the 3D bar graph (Figure 1). It shows that IMA level was high in all the follow-up sample collected from AIS patients.
Table 1: Clinical characteristics of the AIS patients.
| Age | Sex | Etiological subtype |
CT Scan Volume |
NIHSS Score |
m-Rs Score |
Survival |
|---|---|---|---|---|---|---|
| 32 | M | Large Artery atherosclerosis |
176.88CC | 18 | 4 | Discharged |
| 62 | M | Cryptogenic | 165.40CC | 18 | 4 | Discharged |
| 40 | F | Cardioembolic | 145.18CC | 17 | 4 | Discharged |
| 31 | M | Cryptogenic | 166.38CC | 18 | 4 | Discharged |
| 77 | M | Lacunar Infarct | 97.09CC | 10 | 2 | Discharged |
Fig. 1:
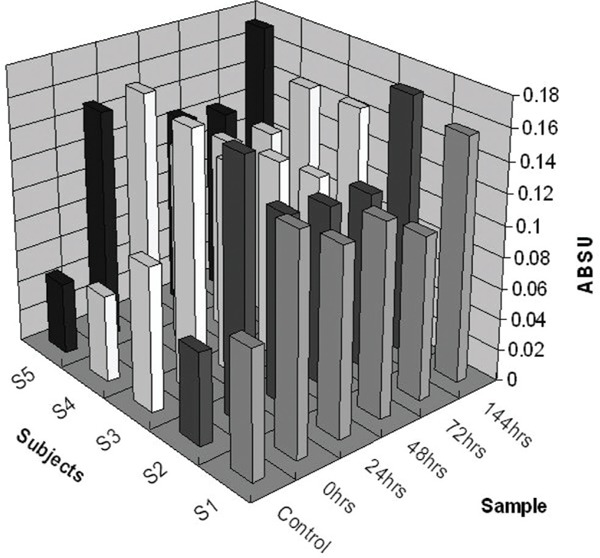
Distribution of the IMA in serum samples from control group (n =5) and follow-up samples of AIS patients (n =5)
The IMA levels in control group and AIS patients are given in the Figure 2. IMA concentrations are presented as the mean ± SD. The mean serum IMA levels in control subjects was 0.067 ± 0.019 ABSU. The mean serum IMA levels in follow up sample collected from stroke patients at admission, 24hrs, 48hrs, 72hrs and 44hrs were 0.159 ± 0.014, 0.124 ± 0.007, 0.124 ± 0.004, 0.115 ± 0.008 and 0.158 ± 0.012 ABSU respectively. There was a statistically significant (p < 0.05) increase in IMA level in serum samples of AIS at admission, 24hrs, 48hrs and 144hrs respectively when compared with control sample. Similarly, on comparing IMA levels in follow-up AIS samples with regard to admission we found that IMA level decreases in follow-up samples till 72hrs, and significant (p < 0.05) decrease was observed at 24hrs and 72hrs respectively which further increases at 144hrs ( p > 0.05 ).
Fig. 2:
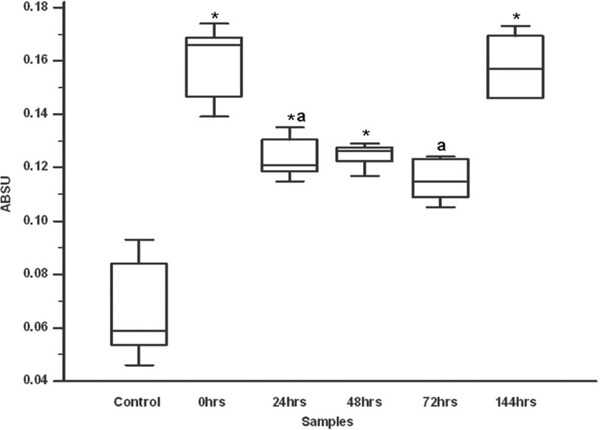
IMA level in control group (n =5) and AIS patients (n =5). *p - value <0.05, control vs. 0hrs, 24hrs, 48hrs, and 144hrs similarly ap - value <0.05 Admission (0hrs) vs. 24hrs, 48hrs, 72hrs 144hrs respectively
Discussion
In the current study we have evaluated the time course of serum level of IMA in AIS patients. We found that serum IMA level increases in AIS patients as compared to control. Significant increases in IMA level were observed at admission, 24hrs, 48hrs and 144hrs respectively when compared with control. Our results are in agreement with the earlier studies that IMA level increases in stroke patients.8 Albumin is a hemodiluting agent, and an increase CBF of both the normal and ischemic brain, by decreasing blood viscosity and by vasodilatation in response to diminished oxygen delivery thus serves as an endogenous neuroprotectant.9 Albumin therapy has been found to be very effective in the treatment of AIS patients.10 It may be possible that protective function of albumin is associated with the N-terminal of the albumin which gets modified by reactive oxygen species generated in response to ischemic event that leads to a loss in its protective ability and thereby an increase in the IMA in AIS patients.
It is reported that IMA levels may be reversible and return to normal level within a few hours (12 to 24 hours) with the removal of free radicals.7 We have also observed that IMA level decreases in the follow-up AIS samples (at 24, 48 and 72 hrs) as compared to admission value. The treatment regimens given to the AIS patients like anti-platelet and anti-edema agents also act as antioxidant.11 Thus, further decrease in IMA level in AIS samples could be the result of beneficial treatment procedure. However, we observe further increase in IMA level at 144h that may suggest further deterioration in the clinical status of AIS patients after initial improvement.
This study is the first to compare IMA in the follow-up samples from ischemic stroke patients. Our preliminary study shows that follow up estimation of IMA in AIS may help in the prediction of the clinical status and outcome in AIS patients. Although study population is small in number, results obtained are very encouraging to undertake a systematic study on large number of patients.
Footnotes
The article complies with International committee of Medical Journal Editor’s uniform requirements for the manuscripts.
Competing interests – None
Source of Funding – None
References
- 1.Banerjee TK, Das SK. Epidemiology of stroke in India. Neurology Asia. 2006;11:1–4. [Google Scholar]
- 2.Stringer KA. Clinical trials in thrombolytic therapy, Part 1: Outcome markers that go beyond mortality reduction. Am J Health Syst Pharm. 1997;54(1):S23–S26. doi: 10.1093/ajhp/54.suppl_1.S23. [DOI] [PubMed] [Google Scholar]
- 3.Kashyap RS, Kabra DP, Nayak AR et al. Protein electrophoretogram in serum of acute ischemic stroke patients and its correlation with S-100β and neuron specific enolase level: A pilot study. Annals of Neurosciences. 2006;13(2):36–40. [Google Scholar]
- 4.Cuzzocrea S, Riley DP, Caputi AP et al. Antioxidant therapy: a new pharmacological approach in shock, inflammation, and ischemia/reperfusion injury. Pharmacol Rev. 2001;53:135–159. [PubMed] [Google Scholar]
- 5.Roy D, Quiles J, Gaze DC et al. Role of reactive oxygen species on the formation of the novel diagnostic marker ischaemia modified albumin. Heart. 2006;92(1):113–114. doi: 10.1136/hrt.2004.049643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bar-Or D, Lau E, Winkler JV. A novel assay for cobalt-albumin binding and its potential as a marker for myocardial ischemia: a preliminary report. J Emerg Med. 2000;19(4):311–315. doi: 10.1016/s0736-4679(00)00255-9. [DOI] [PubMed] [Google Scholar]
- 7.Refaai MA, Wright RW, Parvin CA et al. Ischemia-modified albumin increases after skeletal muscle ischemia during arthroscopic knee surgery. Clin Chim Acta. 2006;366(1-2):264–268. doi: 10.1016/j.cca.2005.10.020. [DOI] [PubMed] [Google Scholar]
- 8.Gunduz A, Turedi S, Mentese A et al. Ischemia-modified albumin levels in cerebrovascular accidents. Am J Emerg Med. 2008;26(8):874–878. doi: 10.1016/j.ajem.2007.11.023. [DOI] [PubMed] [Google Scholar]
- 9.Sundt TM, Waltz AG, Sayre GP. Experimental cerebral infarction: modification by treatment with hemodiluting, hemoconcentrating, and dehydrating agents. J Neurosurg. 1967;26(1):46–56. doi: 10.3171/jns.1967.26.1part1.0046. [DOI] [PubMed] [Google Scholar]
- 10.Belayev L, Zhao W, Pattany PM et al. Diffusion-Weighted Magnetic Resonance Imaging Confirms Marked Neuroprotective Efficacy of Albumin Therapy in Focal Cerebral Ischemia. Stroke. 1998;29:2587–2599. doi: 10.1161/01.str.29.12.2587. [DOI] [PubMed] [Google Scholar]
- 11.Neurology in Clinical Practice: The neurological disorders. In: Biller J, Love BB, editors; Bradley WG, Daroff RB, Fenichel GM, Jankovic J, editors. 4th ed. Philadelphia: Butterworth Heinemann; 2004. pp. 1197–1243. [Google Scholar]