

Abstract
Background
Subtrochanteric and supracondylar femur fractures are difficult injuries to treat in children. Although elastic stable intramedullary nails are commonly used for pediatric femur shaft fractures, there is little information on their effectiveness for managing pediatric subtrochanteric and supracondylar femur fractures.
Questions/purposes
We (1) evaluated radiographic union rates and fracture alignment after elastic nailing of pediatric subtrochanteric and supracondylar femur fractures, (2) identified complications, and (3) determined risk factors for complications.
Methods
Between 2005 and 2011, 36 subtrochanteric fractures and eight supracondylar femur fractures were treated with elastic stable intramedullary nails and had complete followup until clinical and radiographic union. Elastic nailing was used for subtrochanteric fractures in children 5 to 12 years of age or after failed spica cast treatment in younger children and for displaced supracondylar fractures in children older than 5 years. Fracture alignment and union were measured on radiographs, and complications were identified from review of patient charts. Patients with and without complications were compared using nonparametric tests to identify risk factors.
Results
All fractures healed; 23 of 33 (70%) subtrochanteric femur fractures and five of seven (71%) supracondylar femur fractures healed with anterior angulation of about 5°. For subtrochanteric fractures, complications included repositioning/removal of nails before radiographic union (n = 4), malunion (n = 2), fracture (n = 1), irritation (n = 1) at nail insertion site, and limb length discrepancy (n = 1); despite these complications, there were 22 (61%) excellent, 12 (33%) satisfactory, and only two (6%) poor outcomes. For supracondylar fractures, complications included infection after nail removal (n = 1) and nail site irritation (n = 2); there were three (38%) excellent, five (62%) satisfactory, and no poor outcomes. Complications were more likely after subtrochanteric fracture during motor vehicle accident (p = 0.045).
Conclusions
Although complication rates are high with elastic nailing for pediatric subtrochanteric (22%) and supracondylar (38%) femur fractures, elastic nailing represents an important option for difficult-to-manage femur fractures.
Level of Evidence
Level IV, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Introduction
Elastic stable intramedullary nailing is widely used for the management of pediatric femur shaft fractures [6, 11, 15, 21]. Displaced femur fractures involving the proximal metadiaphysis (subtrochanteric) or the distal metadiaphysis (supracondylar) can be difficult to treat due to inherent fracture instability, a short metaphyseal fragment, and close proximity of the fracture to the growth plate [20, 22].
Subtrochanteric femur fractures are uncommon injuries in children, representing only 4% to 10% of pediatric femur fractures [4, 8]. Due to lack of a uniform definition of subtrochanteric fractures in children and varied fracture patterns, many studies tend to combine proximal shaft fractures with subtrochanteric fractures and report higher incidence rates for these fractures [7, 26]. Several unique characteristics make these fractures difficult to manage [7, 10, 22, 26]. One characteristic is a short proximal metaphyseal fragment, which usually displaces in flexion, abduction, and external rotation, causing difficulty in obtaining and maintaining reduction. The common fracture patterns (oblique or spiral) impart instability to the fracture, especially in maintaining length. The remodeling potential of these fractures is limited, as the growth from the proximal femur is less than the growth from the distal femur.
Supracondylar femur fractures are another uncommon and difficult-to-manage subset of injuries, with a reported prevalence of 1% to 12% of all pediatric femur fractures [3, 29]. These fractures are classified based on displacement and presence of pathologic bone [29]. Several unique characteristics make these fractures challenging to manage. When displaced, the short distal metaphyseal fragment and associated pull of gastrocnemius or adductors make it difficult to obtain and maintain reduction, especially with nonsurgical treatment. The effect of this fracture on the adjacent growth plate is not known. Since some of these fractures are pathologic, it can limit the purchase of internal fixation.
Elastic nailing has been described as a potential treatment for both pediatric subtrochanteric and supracondylar femur fractures [5, 12], but its effectiveness for managing subtrochanteric fractures has only been minimally reported [14, 22], and its effectiveness for managing supracondylar fractures has never been reported.
We therefore (1) evaluated union rate and fracture alignment on radiographs after elastic nailing of pediatric subtrochanteric and supracondylar femur fractures, (2) identified complications associated with the use of elastic nailing, and (3) determined risk factors for the development of complications.
Patients and Methods
Study Design
This study was approved by our institutional review board. We reviewed hospital records of 223 patients younger than 18 years treated with elastic stable intramedullary nails for a femur shaft fracture between January 2005 and March 2011. This represented 52% of the femoral shaft fractures (223 of 433) treated at our hospital during this period. To be included, selected patients were required to have (1) either a subtrochanteric or supracondylar femur fracture as confirmed on radiographs, (2) operative treatment with elastic nailing, and (3) followup until complete clinical and radiographic union or a minimum of 1 year. Subtrochanteric femur fractures were defined as fractures within 10% of total femur length below the lesser trochanter [22]. The total femur length was measured on preoperative or postoperative femur radiographs (Fig. 1). Supracondylar femur fractures were defined as fractures within the supracondylar region, extending from the femoral physis distally to proximally, a distance equivalent to the measurement of the widest part of the physis on AP radiographs (Fig. 2) [28]. Exclusion criteria included having (1) a congenital disorder, (2) an incomplete/impending fracture, or (3) incomplete medical records. Seven patients with subtrochanteric fractures were excluded (one impending fracture, two with osteogenesis imperfecta, two with cerebral palsy, two with spina bifida). Indications for elastic nailing differed by fracture location. During the study period, in general, elastic nailing was used for subtrochanteric fractures in children 5 to 12 years of age or after failed spica cast treatment in younger children, with plating and rigid intramedullary nailing as other options. Elastic nailing was generally used for displaced supracondylar fractures in children older than 5 years; however, depending on the physician’s preference, K-wires or plates were other treatment options.
Fig. 1A–C.

(A) Subtrochanteric femur fracture is defined when the fracture is within 10% of total femoral length below the lesser trochanter. (B) The total length of the femur is measured from the top of the femoral head to the distal aspect of lateral femoral condyle. (C) Supracondylar femur fracture is defined on an AP radiograph as a fracture within a square box whose sides are equivalent to the measurement of the distal femoral physis.
Fig. 2A–E.

(A) A long oblique subtrochanteric fracture is shown. (B) During elastic nailing, the medial nail is inserted further along the femoral neck and the lateral nail is advanced into or through the greater trochanter. (C) The lateral view helps to verify the position of the nail tips and avoid perforation of the femoral neck. (D, E) The nails are cut so that they are at or just above the level of distal femoral physis and fracture reduction and stability should be confirmed at the end of the procedure.
Patient Demographics
Medical charts were reviewed for age, sex, weight, mechanism of injury, fracture type (transverse/short oblique: < 30° angulation; long oblique or spiral: > 30° angulation [28]), fracture comminution according to the Winquist-Hansen classification [31], associated injuries, date and time of surgery (before or after 5 pm), nail size, postoperative immobilization, and date of implant removal.
Based on inclusion and exclusion criteria, we identified a group of 44 children (36 with subtrochanteric and eight with supracondylar femur fractures) whose injuries were managed using elastic nailing. All fractures were closed fractures without any neurovascular deficits. Subtrochanteric fractures were identified in 26 boys and 10 girls with a mean ± SD age of 6.5 ± 2.7 years (range, 1–12 years) (Table 1). Elastic nailing has been previously reported in very young children (younger than 2 years) with femoral shaft fractures [2]. The youngest patient in our sample was treated with elastic nailing after failing two closed reductions and spica cast treatments, with persistent reangulation into varus and flexion. Two patients had bilateral femur fractures, but only the side with the subtrochanteric fracture was included for our study. Associated injuries included odontoid fracture (n = 1), ipsilateral metacarpal fracture (n = 1), and ipsilateral acetabular and metatarsal fracture (n = 1). All four patients younger than 4 years had failed initial spica cast treatment. Supracondylar femur fractures were identified in two boys and six girls with a mean age of 9.0 ± 2.6 years (range, 6–14 years) (Table 1). Four of these patients had pathologic fractures involving nonossifying fibroma of the distal femur.
Table 1.
Characteristics of pediatric patients with subtrochanteric and supracondylar femur fractures treated with elastic stable intramedullary nails
| Variable | Subtrochanteric | Supracondylar |
|---|---|---|
| Age (years)* | 6.0 (5.0–8.8) | 9.0 (7.0–10.0) |
| Sex (number of patients) | ||
| Male | 26 (72%) | 2 (25%) |
| Female | 10 (28%) | 6 (75%) |
| Weight (kg)* | 24 (18–29) | 30 (26–41) |
| Fractured limb (number of patients) | ||
| Left | 16 (44%) | 4 (50%) |
| Right | 20 (56%) | 4 (50%) |
| Fracture type (number of patients) | ||
| Transverse | 8 (22%) | 4 (50%) |
| Oblique/spiral | 28 (78%) | 4 (50%) |
| Fracture comminution (number of patients) | ||
| Grade I | 2 (6%) | 1 (12.5%) |
| Grade II | 7 (19%) | 3 (37.5%) |
| Grade III | 6 (17%) | 0 (0%) |
| Cause of injury (number of patients) | ||
| Fall | 16 (44%) | 4 (50%) |
| Motor vehicle accident | 13 (36%) | 1 (12.5%) |
| Sport | 6 (17%) | 3 (37.5%) |
| Other | 1 (3%) | 0 (0%) |
| Time of surgery (number of patients) | ||
| Day (≤ 5 pm) | 25 (78%) | 2 (40%) |
| Night (> 5 pm) | 7 (22%) | 3 (60%) |
| Nail size (in pairs, 1 missing) (number of patients) | ||
| 2.5 mm | 5 (14%) | 0 (0%) |
| 3.0 mm | 16 (46%) | 0 (0%) |
| 3.5 mm | 9 (26%) | 6 (75%) |
| 4.0 mm | 5 (14%) | 2 (25%) |
| Postoperative immobilization (number of patients) | ||
| None | 12 (34%) | 2 (25%) |
| Knee Immobilizer | 21 (60%) | 4 (50%) |
| Cast | 2 (6%) | 2 (25%) |
* Values are expressed as median, with interquartile range in parentheses.
Surgical Description
For subtrochanteric femur fractures, two nails were inserted, one medial and one lateral, into the distal femoral metaphysis and driven retrograde to the fracture site, as per the surgical principles outlined by Metaizeau [18]. The technique was modified so that the medial nail would advance into the femoral neck, just short of the proximal femoral physis. The lateral nail was advanced and inserted into or through the trochanteric apophysis (Fig. 3) [22]. For supracondylar femur fractures, two nails were inserted (both laterally) either in the antegrade direction from just below the greater trochanter (one nail was C-shaped, one nail was S-shaped) in five patients or in a retrograde direction from just above the distal femoral physis in three patients; the choice of antegrade or retrograde nail insertion was based on surgeon preference (Fig. 4). An attempt was made to position both nails such that the tips were pointing in opposite directions on AP and lateral views [24]. The stability of the fracture was assessed under fluoroscopic guidance and selective postoperative immobilization was used. Patients were advised against weightbearing activities until clinical and radiographic healing was confirmed. Once radiographic fracture union was confirmed, nails were routinely removed. This was performed in 34 of 36 (94%) patients with subtrochanteric fractures at a mean of 5.7 ± 5.9 months after the initial surgery and in seven of eight (88%) patients with supracondylar fractures at a mean of 5.2 ± 1.4 months after the initial surgery.
Fig. 3A–E.

(A) A supracondylar femur fracture is shown. (B, C) The fracture is treated with antegrade nails such that a spread of the nails is achieved at the fracture site and the nail tips point away from each other. (D, E) Full-length femur radiographs show the insertion of the nail below the greater trochanter with one nail C-shaped and the other S-shaped.
Fig. 4A–B.
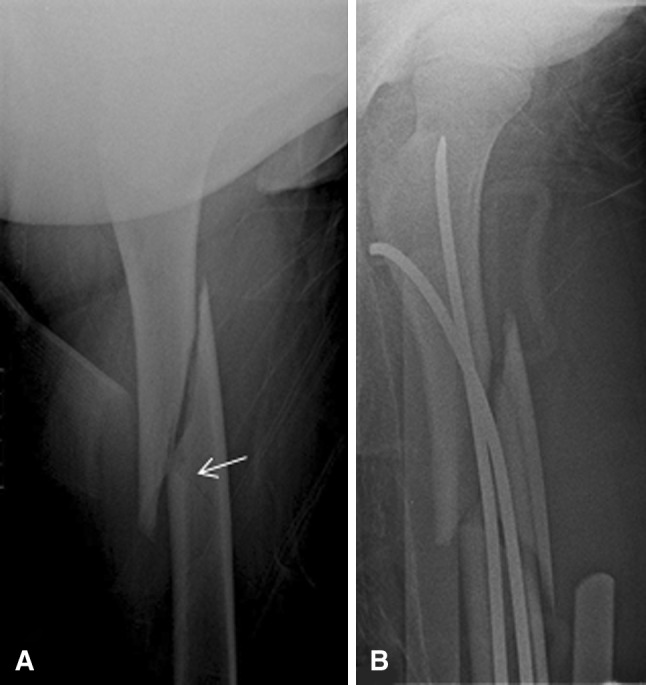
(A) A preoperative radiograph of a subtrochanteric fracture shows an undisplaced butterfly fragment (arrow). (B) A postoperative radiograph shows the iatrogenic comminution of the butterfly fragment.
Radiographic Evaluation
Implant position and coronal and sagittal plane angulation on the final AP and lateral radiographic views, respectively, were measured once by a single physician rater. Fracture healing was defined as bridged femoral cortices (three or four of four cortices) on AP and lateral views [30]. Malunion at latest followup was defined as angulation of greater than 10° on AP or lateral view.
Complications and Risk Factors
Complications, including patient-reported symptoms and unexpected return to the operating room, were identified by medical chart and radiographic review. The outcome scoring system proposed by Flynn et al. [6] was used to classify the results of elastic nailing treatment as excellent, good, or fair based on malalignment, leg length inequality, pain, and complications (Table 2). Statistical analyses were performed for the subtrochanteric femur fracture group. The percentages of complications were calculated. Patients with and without complications were compared in terms of sex and affected side using Fisher exact tests; cause of injury, fracture type, and postoperative treatment using chi-square tests; nail size and comminution grade using Cochran-Armitage trend tests; and degree of varus and valgus using Mann-Whitney tests. Nonparametric tests were selected due to the small sample size and nonnormal distribution of data. Accordingly, medians and interquartile ranges are reported for these comparisons instead of means and SDs as reported for all other variables in the study. Descriptive statistics were used to describe the supracondylar femur fracture group. Statistical significance was set at p values of less than 0.05.
Table 2.
Results according to the elastic nailing outcome scoring system (Flynn et al. [6])
| Variable | Excellent result | Satisfactory result | Poor result |
|---|---|---|---|
| Criteria | |||
| Malalignment (°) | ≤ 5 | 6–10 | > 10 |
| Leg length inequality (cm) | < 1.0 | 1.0–2.0 | > 2.0 |
| Pain | None | None | Present |
| Complications | None | Minor and resolved | Major complication and/or lasting morbidity |
| Results (number of patients) | |||
| Subtrochanteric femur fractures | 22 (61%) | 12 (33%) | 2 (6%) |
| Supracondylar femur fractures | 3 (38%) | 5 (62%) | 0 (0%) |
Results
Radiographic Results
The majority of fractures healed with anterior angulation (apex anterior). Of the subtrochanteric fractures, 11 of 32 (34%) healed in varus (5° ± 4°), 14 of 32 (44%) healed in valgus (4° ± 2°), 23 of 33 (70%) healed with anterior angulation that was apex anterior (5° ± 3°), and five of 33 (15%) healed with posterior angulation that was apex posterior (5° ± 1°). Of the supracondylar fractures, two of seven (29%) healed in varus (5° ± 4°), three of seven (43%) healed in valgus (4° ± 2°), five of seven (71%) healed with anterior angulation (5° ± 3°), and one of seven (14%) healed in posterior angulation (4° ± 0°). No nonunions were identified in either fracture group.
Complications
Of the 36 patients with subtrochanteric femur fractures, eight (22%) patients had a total of nine complications (Table 3). Four patients returned to the operating room for repositioning/removal of nails before complete radiographic fracture union at around 2 months after the initial surgery. Critical analysis of postoperative radiographs of these patients revealed that the nails could have been inserted further into the femoral neck and into the greater trochanter. One patient sustained a fracture at the nail insertion site after a fall, and the fracture was treated with cast immobilization with nails retained (Fig. 5). One patient had irritation at the nail entry site. One patient had a 2-cm limb length discrepancy, and two patients had malunion (one had 14° varus, one had 11° procurvatum); none of these three patients had symptoms requiring any treatment. No complications were encountered during nail removal. Five patients sustained iatrogenic comminution of the fracture (three Type II, two Type III) at the time of nail insertion, and these were identified on intraoperative fluoroscopic imaging. Careful evaluation of preoperative radiographs revealed a nondisplaced butterfly fragment in all five patients with iatrogenic comminution of the fracture. Despite complications, there were 22 (61%) excellent, 12 (33%) satisfactory, and two (6%) poor final outcomes, based on the criteria of Flynn et al. [6], after elastic nailing of subtrochanteric femur fractures (Table 2).
Table 3.
Complications of elastic stable intramedullary nailing for pediatric subtrochanteric and supracondylar femur fractures
| Patient | Sex | Age (years) | Injury cause | Fracture type | Comminution grade | Nail size (mm) | Complication | Treatment |
|---|---|---|---|---|---|---|---|---|
| Subtrochanteric femur fractures | ||||||||
| 1 | Male | 9 | Motor vehicle accident | Oblique | II | 3.5 | Prominent nails Malunion with 14° varus |
One nail removed, one nail advanced None (asymptomatic) |
| 2 | Male | 5 | Motor vehicle accident | Oblique | II | 2.5 | Exposed implant on the medial side | Nails removed Spica cast |
| 3 | Male | 5 | Sled riding | Transverse | 3 | Irritation at nail insertion site | None (routine nail removal) | |
| 4 | Male | 3 | Motor vehicle accident | Oblique | 2.5 | Loss of fracture reduction | Nail repositioned Spica cast |
|
| 5 | Male | 11 | Motor vehicle accident | Transverse | 4, 3.5 | Prominent nails | Nails advanced | |
| 6 | Male | 11 | Fall | Oblique | III | 4 | 2-cm leg length discrepancy | None (asymptomatic) |
| 7 | Male | 12 | Motor vehicle accident | Spiral | I | 4 | Fracture at nail insertion site | Nails retained Cast treatment |
| 8 | Male | 1 | Fall | Oblique | 2.5 | Malunion with anterior angulation of 11° | None (asymptomatic) | |
| Supracondylar femur fractures | ||||||||
| 1 | Female | 10 | Motor vehicle accident | Transverse | I | 3.5 (retrograde) | Pain/irritation at nail insertion site | None (routine nail removal) |
| 2 | Female | 6 | Fall | Transverse | 3.5 (antegrade) | Irritation at nail insertion site | None (routine nail removal) | |
| 3 | Female | 8 | Fall | Spiral | 3.5 (antegrade) | Infective bursitis of the greater trochanter | Irrigation and débridement Intravenous antibiotics |
|
Fig. 5A–B.

(A) A subtrochanteric femur fracture (arrow) was treated with elastic nailing. (B) The patient had a fall after the subtrochanteric fracture had healed and sustained a fracture at the level of nail entry.
Of the eight patients with supracondylar femur fractures, three (38%) had complications. Two patients had irritation at the nail insertion site, and one patient sustained a deep wound infection after removal of the antegrade nails from the greater trochanter that required surgical drainage and intravenous antibiotics. No patients had malunion or limb length discrepancy. There were three (38%) excellent, five (62%) satisfactory, and no poor final outcomes after elastic nailing of supracondylar femur fractures (Table 2).
Risk Factors for Complications
Complications were more common in patients whose subtrochanteric fractures were caused by motor vehicle accidents than after falls or sports injuries (p = 0.045; Table 4). Patients who had complications did not differ in age (p = 0.62), sex (p = 0.08), weight (p = 0.56), fractured limb (p = 0.71), fracture type (p = 1.00), fracture comminution (p = 0.69), time of surgery (p = 1.00), or nail size (p = 0.06), when compared to patients without complications.
Table 4.
Characteristics of pediatric patients with complications after subtrochanteric fracture treatment
| Variable | No complication | Complication | Difference |
|---|---|---|---|
| Age (years)* | 6.0 (5.0–8.0) | 7.0 (3.5–11.0) | 0.62† |
| Sex (number of patients) | 0.076‡ | ||
| Male | 18 (69%) | 8 (31%) | |
| Female | 10 (100%) | 0 (0%) | |
| Weight (kg)* | 24 (18–27) | 22 (18–43) | 0.56† |
| Fractured limb (number of patients) | 0.71‡ | ||
| Left | 13 (81%) | 3 (19%) | |
| Right | 15 (75%) | 5 (25%) | |
| Fracture type (number of patients) | 1.00‡ | ||
| Transverse | 6 (75%) | 2 (25%) | |
| Oblique/spiral | 22 (79%) | 6 (21%) | |
| Fracture comminution (n = 15) (number of patients) | 0.36§ | ||
| Grade I | 1 (50%) | 1 (50%) | |
| Grade II | 5 (71%) | 2 (29%) | |
| Grade III | 5 (83%) | 1 (17%) | |
| Cause of injury (number of patients) | 0.045∥ | ||
| Fall | 14 (88%) | 2 (12%) | |
| Motor vehicle accident | 8 (62%) | 5 (38%) | |
| Sport | 6 (100%) | 0 (0%) | |
| Other | 0 (0%) | 1 (100%) | |
| Time of surgery (n = 32) (number of patients) | 1.00‡ | ||
| Day (≤ 5 pm) | 19 (76%) | 6 (24%) | |
| Night (> 5 pm) | 6 (86%) | 1 (14%) | |
| Nail size (number of patients) | 0.064∥ | ||
| 2.5 mm | 2 (40%) | 3 (60%) | |
| 3.0 mm | 15 (94%) | 1 (6%) | |
| 3.5 mm | 7 (78%) | 2 (22%) | |
| 4.0 mm | 3 (60%) | 2 (40%) | |
* Values are expressed as median, with interquartile range in parentheses; †Mann-Whitney test; ‡Fisher exact test; §Cochran-Armitage trend test; ∥chi-square test.
Discussion
Pediatric subtrochanteric and supracondylar femur fractures can be challenging to treat due to instability and displacement of the short metaphyseal fragments, as well as limited remodeling potential of the proximal femur in subtrochanteric fractures and the pathologic nature of many supracondylar fractures [7, 10, 22, 26]. For these fractures, the option of elastic nailing is appealing as it is minimally invasive with decreased surgical morbidity, decreased hospital stay, and earlier return to function without the need for rigid immobilization or a spica cast. The effectiveness of elastic nailing has been minimally evaluated for pediatric subtrochanteric fractures [14, 22] and, to our knowledge, has not been evaluated for supracondylar femur fractures. We therefore evaluated radiographic union rates, fracture alignment, and complication rates after elastic nailing of these fractures. For subtrochanteric fractures, we also assessed the risk factors for developing complications after elastic nailing.
The limitations of this study include the lack of a control group of patients with alternative treatment options for comparison since most of these fractures at our institution are treated with elastic nailing. Length of followup varied, although all patients were followed until clinical and radiographic fracture union and return to full activity, which was typically a year after their initial surgery. This duration of followup for pediatric femur fractures in asymptomatic patients is considered to be adequate [6]. Due to the retrospective nature of the study, some vital information such as treatment of complications at another institution could have been missed.
Healing with an anterior angulation (apex anterior) was common after elastic nailing of pediatric subtrochanteric fractures. Fractures healed with more than 5° of angulation in 12 of 36 femurs (33%) in our study, compared to seven of 58 (12%) in the study of Flynn et al. [6] and four of 25 (16%) in the study of Li et al. [14]. Malalignment of greater than 10° was identified in two of our patients, compared to one in the study of Flynn et al. [6]. None of the studies, including ours, identified nonunion after elastic nailing treatment.
We found a complication rate of 22% (eight of 36) in patients with subtrochanteric femur fractures, which is considerably less than the 48% (12 of 25) complication rate identified by Li et al. [14] but greater than the 15% (two of 13) complication rate by Pombo and Shilt [22]. Four (11%) of our patients with subtrochanteric fractures required a return to the operating room before fracture union. Leg length inequality of 1 to 2 cm was a common complication, with two patients in our study, four in the study of Li et al. [14], and two in the study of Pombo and Shilt [22]. The need to return to the operating room for repositioning/removal of irritating, prominent nails has also been reported [14]. Flynn et al. [6] reported loss of reduction in three patients compared to one in our study. The outcomes of elastic nailing of subtrochanteric fractures in our study (61% excellent, 33% satisfactory, 6% poor) are similar to the previous studies on titanium elastic nailing by Flynn et al. [6] for any type of femur fracture, with 39 (67%) excellent, 18 (31%) satisfactory, and one (2%) poor result, and by Li et al. [14] for subtrochanteric fractures, with 13 (52%) excellent, 10 (40%) satisfactory, and two (8%) poor results. Better results, however, were identified by Pombo and Shilt [22] after titanium elastic nailing of subtrochanteric fractures, with 11 (85%) excellent, two (15%) satisfactory, and no poor results. Complications occurred in three of eight (38%) of our patients with supracondylar femur fractures, including deep wound infection after removal of the antegrade nails from the greater trochanter (n = 1) and irritation at the nail insertion site (n = 2). In our study, all patients treated with elastic nailing for supracondylar femur fractures achieved a satisfactory to excellent result. Closed reduction alone is reportedly difficult for these fractures [29]; however, similar outcomes, with eight of nine satisfactory results, have been achieved with closed reduction and percutaneous pinning [3].
In this study, complication rates were higher after motor vehicle accidents than after other injury causes, probably due to associated soft tissue injury or increased displacement of the subtrochanteric fracture. All complications occurred in boys. Other studies have found four times higher complication rates in length-unstable fractures (long oblique or spiral fracture with comminution) compared to length-stable subtrochanteric fractures [14, 27]; however, there was no difference in our sample. With few factors predicting complications, it is difficult to provide indications on when or when not to use elastic nailing for pediatric subtrochanteric fractures. The following are suggestions of technical modifications that may prevent and/or address complications. Adequate muscle relaxation and effective traction during surgery can help with fracture reduction. For subtrochanteric fractures, 10° to 15° of external rotation of the leg can help to align the distal fracture fragment with the proximal fragment, which is typically externally rotated. Similarly, flexion of the leg and anterior direction of the nail tip can help navigate the nail across the fracture, as the proximal fragment is typically flexed. Advancement of the medial nail deep into the proximal fragment along the femoral neck just short of the proximal femoral physis has been shown to reduce the risk of angular complications [22]. A lateral fluoroscopic view should confirm adequate nail placement in the femoral neck since posterior perforation of the femoral neck has been reported due to normal femoral anteversion [5, 19]. The nails should be cut short and impacted to lie along the metaphysis, at or just above the level of the distal femoral physis. To prevent soft tissue irritation, the nail should not be bent away from the femur. Leaving 1 to 2 cm of the nail outside of the femur and distal to the entry point aids in removal. Recommendations have been made to perforate the proximal femoral physis and to place end caps over the cut ends of the nail [5, 12]. Iatrogenic comminution can be avoided by directing the nail tip away from the long spikes of the fracture fragments [25]; however, this is not always possible when trying to navigate the fracture site. The other treatment options for subtrochanteric femur fractures, including cast treatment, plate fixation, external fixation, and rigid intramedullary nailing, each have their own associated complications [9, 13, 14, 16, 23, 27]. For supracondylar femur fractures, retrograde insertion, as in three of our eight patients, has shown acceptable stability when compared to antegrade insertion [17]. However, it can be technically challenging due to the low entry level for nail insertion and difficulty in crossing the nails distal to the fracture site [12]. Displaced supracondylar femur fractures typically need to be surgically stabilized due to higher failures rates with closed reduction and immobilization [29] and the potential for common peroneal nerve palsy and septic knee arthritis after closed reduction and percutaneous crossed pinning [3, 29]. Plate fixation and external fixation have shown promising results and are additional options for treatment of supracondylar fractures [1, 9, 13, 23, 29].
This retrospective study reports on the radiographic outcomes and complications of a large series of subtrochanteric and supracondylar femur fractures in children treated with elastic stable intramedullary nails. The results, including satisfactory to excellent results in 94% of subtrochanteric fractures and 100% of supracondylar fractures, suggest that elastic nailing is an option for the management of these pediatric femur fractures. Although the complication rates are high with elastic nailing for pediatric subtrochanteric (22%) and supracondylar (38%) fractures, elastic nailing represents an important option for difficult-to-manage pediatric fractures.
Acknowledgments
The authors thank Dr. Junichi Tamai, Dr. Charles Mehlman, Dr. Viral Jain, and Dr. Eric Wall at Cincinnati Children’s Hospital Medical Center for contribution of their surgical cases to this study.
Footnotes
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
This work was performed at Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA.
References
- 1.Baker P, McMurtry I, Port A. The treatment of distal femoral fractures in children using the LISS plate: a report of two cases. Ann R Coll Surg Engl. 2008;90:1–3. doi: 10.1308/147870808X302985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bopst L, Reinberg O, Lutz N. Femur fracture in preschool children: experience with flexible intramedullary nailing in 72 children. J Pediatr Orthop. 2007;27:299–303. doi: 10.1097/BPO.0b013e3180326713. [DOI] [PubMed] [Google Scholar]
- 3.Butcher CC, Hoffman EB. Supracondylar fractures of the femur in children: closed reduction and percutaneous pinning of displaced fractures. J Pediatr Orthop. 2005;25:145–148. doi: 10.1097/01.bpo.0000149860.50400.92. [DOI] [PubMed] [Google Scholar]
- 4.Daum R, Jungbluth KH, Metzger E, Hecker WC. [Results of treatment of subtrochanteric and supracondylous femoral fractures in children] [in German] Chirurg. 1969;40:217–220. [PubMed] [Google Scholar]
- 5.Dietz HG, Schmittenbecher PP, Slongo T, Wilkins KE. AO Manual of Fracture Management: Elastic Stable Intramedullary Nailing (ESIN) in Children. Clavadelerstrasse, Switzerland: AO Publishing; 2006. pp. 1–233. [Google Scholar]
- 6.Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: a multicenter study of early results with analysis of complications. J Pediatr Orthop. 2001;21:4–8. doi: 10.1097/01241398-200101000-00003. [DOI] [PubMed] [Google Scholar]
- 7.Ireland DC, Fisher RL. Subtrochanteric fractures of the femur in children. Clin Orthop Relat Res. 1975;110:157–166. doi: 10.1097/00003086-197507000-00020. [DOI] [PubMed] [Google Scholar]
- 8.Jeng C, Sponseller PD, Yates A, Paletta G. Subtrochanteric femoral fractures in children: alignment after 90 degrees-90 degrees traction and cast application. Clin Orthop Relat Res. 1997;341:170–174. doi: 10.1097/00003086-199708000-00026. [DOI] [PubMed] [Google Scholar]
- 9.Kanlic EM, Anglen JO, Smith DG, Morgan SJ, Pesántez RF. Advantages of submuscular bridge plating for complex pediatric femur fractures. Clin Orthop Rel Res. 2004;426:244–251. doi: 10.1097/01.blo.0000138961.34810.af. [DOI] [PubMed] [Google Scholar]
- 10.Kasser JR, Beaty JH. Femoral shaft fractures. In: Beaty JH, Kasser JR, editors. Rockwood and Wilkins’ Fractures in Children. 6. Philadelphia, PA: Lippincott Williams & Wilkins; 2006. pp. 893–936. [Google Scholar]
- 11.Kocher MS, Sink EL, Blasier RD, Luhmann SJ, Mehlman CT, Scher DM, Metheney T, Sanders JO, Watters WC, 3rd, Keith MW, Haralson RH, 3rd, Turkelson CM, Wies JL, Sluka P, Hitchcock K. Treatment of pediatric diaphyseal femur fractures. J Am Acad Orthop Surg. 2009;17:718–725. doi: 10.5435/00124635-200911000-00006. [DOI] [PubMed] [Google Scholar]
- 12.Lascombes P. Flexible Intramedullary Nailing in Children: the Nancy University Manual. Heidelberg, Germany: Springer; 2010. pp. 1–317. [Google Scholar]
- 13.Li Y, Hedequist DJ. Submuscular plating of pediatric femur fracture. J Am Acad Orthop Surg. 2012;20:596–603. doi: 10.5435/JAAOS-20-09-596. [DOI] [PubMed] [Google Scholar]
- 14.Li Y, Heyworth BE, Glotzbecker M, Seeley M, Suppan CA, Gagneir J, VanderHave KL, Caird MS, Farley FA, Hedequist D. Comparison of titanium elastic nail and plate fixation of pediatric subtrochanteric femur fractures. J Pediatr Orthop. 2013;33:232–238. doi: 10.1097/BPO.0b013e318288b496. [DOI] [PubMed] [Google Scholar]
- 15.Ligier JN, Metaizeau JP, Prévot J, Lascombes P. Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br. 1988;70:74–77. doi: 10.1302/0301-620X.70B1.3339064. [DOI] [PubMed] [Google Scholar]
- 16.MacNeil JA, Francis A, El-Hawary R. A systematic review of rigid, locked, intramedullary nail insertion sites and avascular necrosis of the femoral head in the skeletally immature. J Pediatr Orthop. 2011;31:377–380. doi: 10.1097/BPO.0b013e3182172613. [DOI] [PubMed] [Google Scholar]
- 17.Mehlman CT, Nemeth NM, Glos DL. Antegrade versus retrograde titanium elastic nail fixation of pediatric distal-third femoral-shaft fractures: a mechanical study. J Orthop Trauma. 2006;20:608–612. doi: 10.1097/01.bot.0000249414.59012.d9. [DOI] [PubMed] [Google Scholar]
- 18.Metaizeau JP. Stable elastic intramedullary nailing for fractures of the femur in children. J Bone Joint Surg Br. 2004;96:954–957. doi: 10.1302/0301-620X.86B7.15620. [DOI] [PubMed] [Google Scholar]
- 19.Narayanan UG, Hyman JE, Wainwright AM, Rang M, Alman BA. Complications of elastic stable intramedullary nail fixation of pediatric femoral fractures, and how to avoid them. J Pediatr Orthop. 2004;24:363–369. doi: 10.1097/01241398-200407000-00004. [DOI] [PubMed] [Google Scholar]
- 20.Parikh SN, Jain VV, Denning J, Tamai J, Mehlman CT, McCarthy JJ, Wall EJ, Crawford AH. Complications of elastic stable intramedullary nailing in pediatric fracture management. J Bone Joint Surg Am. 2012;94:e184. doi: 10.2106/JBJS.L.00668. [DOI] [PubMed] [Google Scholar]
- 21.Parikh SN, Wells L, Mehlman CT, Scherl SA. Management of fractures in adolescents. J Bone Joint Surg Am. 2010;92:2947–2958. doi: 10.2106/00004623-201012150-00010. [DOI] [PubMed] [Google Scholar]
- 22.Pombo MW, Shilt JS. The definition and treatment of pediatric subtrochanteric femur fractures with titanium elastic nails. J Pediatr Orthop. 2006;26:364–370. doi: 10.1097/01.bpo.0000203005.50906.41. [DOI] [PubMed] [Google Scholar]
- 23.Sabharwal S. Role of Ilizarov external fixator in the management of proximal/distal metadiaphyseal pediatric femur fractures. J Orthop Trauma. 2005;19:563–569. doi: 10.1097/01.bot.0000174706.03357.26. [DOI] [PubMed] [Google Scholar]
- 24.Sagan ML, Datta JC, Olney BW, Lansford TJ, McIff TE. Residual deformity after treatment of pediatric femur fractures with flexible titanium nails. J Pediatr Orthop. 2010;30:638–643. doi: 10.1097/BPO.0b013e3181efb8e2. [DOI] [PubMed] [Google Scholar]
- 25.Schmittenbecher PP, Dietz HG, Linhart WE, Slongo T. Complications and problems in intramedullary nailing of children’s fractures. Eur J Trauma. 2000;26:287–293. doi: 10.1007/PL00002453. [DOI] [Google Scholar]
- 26.Segal LS. Custom 95 degree condylar blade plate for pediatric subtrochanteric femur fractures. Orthopedics. 2000;23:103–107. doi: 10.3928/0147-7447-20000201-10. [DOI] [PubMed] [Google Scholar]
- 27.Sink EL, Faro F, Polousky J, Flynn K, Gralla J. Decreased complications of pediatric femur fractures with a change in management. J Pediatr Orthop. 2010;30:633–637. doi: 10.1097/BPO.0b013e3181efb89d. [DOI] [PubMed] [Google Scholar]
- 28.Slongo TF, Audigé L, AO Pediatric Classification Group Fracture and dislocation classification compendium for children: the AO pediatric comprehensive classification of long bone fractures (PCCF) J Orthop Trauma. 2007;21:S135–S160. doi: 10.1097/00005131-200711101-00020. [DOI] [PubMed] [Google Scholar]
- 29.Smith NC, Parker D, McNicol D. Supracondylar fractures of the femur in children. J Pediatr Orthop. 2001;21:600–603. [PubMed] [Google Scholar]
- 30.Wall EJ, Jain V, Vora V, Mehlman CT, Crawford AH. Complications of titanium and stainless steel elastic nail fixation of pediatric femoral fractures. J Bone Joint Surg Am. 2008;90:1305–1313. doi: 10.2106/JBJS.G.00328. [DOI] [PubMed] [Google Scholar]
- 31.Winquist RA, Hansen ST, Clawson DK. Closed intramedullary nailing of femoral fractures: a report of five hundred and twenty cases. J Bone Joint Surg Am. 1984;66:529–539. [PubMed] [Google Scholar]