

Abstract
Esophageal duplication cyst (EDC) is classified as a subgroup of foregut duplication cyst. They are very rare and predominantly detected in children. We present an unusual cause of wheezing in a 2-month-old infant. The diagnosis of EDC was suspected by bronchoscopy, provisionally confirmed by magnetic resonance imaging, and followed by successful surgical excision of the cyst. We conclude that foregut duplication cyst of the esophagus is very rare, and must be considered in the differential diagnosis of persistent wheezing in infants who do not respond to conventional treatment.
Keywords: Esophageal duplication cyst, infant, wheezing
Introduction
Esophageal duplications are rare congenital anomalies and are the second most common duplications of the gastrointestinal tract in children.[1] Patients usually present with respiratory distress because of airway compression (due to enlarging mass), or are asymptomatic with a thoracic mass found incidentally on chest radiograph.[1] They are prone to develop complications (bleeding, infection, etc.,) and even malignancies. The treatment of choice for these cysts is surgical excision.[2] Very few case reports have been described in literature in infants. We are reporting a rare case of esophageal duplication cyst in a 2-month-old infant who presented with persistent wheezing.
Case Report
A 2-month-old, male infant presented with a history of fever and increased respiratory rate for 3 days. Infant was born as full term, weighing 2600 g, through caesarean section to a primigravida mother. Antenatal and perinatal history was uneventful. On physical examination, he had tachycardia, tachypnea with sub costal retractions, maintaining oxygen saturation of 88% at room air. There was no facial dysmorphism and other obvious congenital malformation. Bilateral rhonchi were present on auscultation of the chest. Other systemic examination was normal.
Hemogram and other biochemical parameters were normal. Chest radiograph revealed only bilateral hyperinflation [Figure 1]. The provisional diagnosis of bronchiolitis was made, and the infant was kept on supportive treatment. Despite all supportive measures, wheezing persisted even after 7 days, so we thought of investigating for alternative diagnosis. The bronchoscopy was done, which revealed external airway compression. Magnetic resonance imaging (MRI) scan of the neck was done, which revealed a well-defined lobulated smoothly marginated lesion of altered signal intensity in pre-/left para-esophageal region at subcarinal level. Lesion was abutting the esophagus medially, trachea anteriorly and aortic arch laterally. A provisional diagnosis of foregut duplication cyst was made [Figures 2 and 3].
Figure 1.
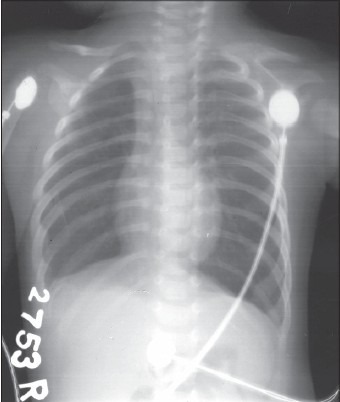
Chest radiograph showing bilateral hyperinflation
Figure 2.
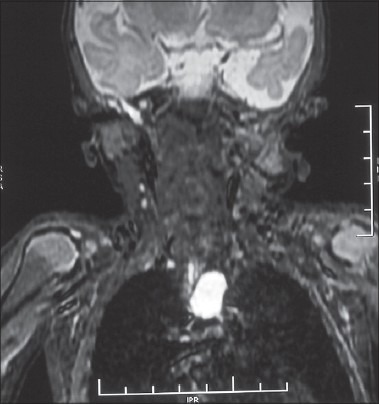
Magnetic resonance imaging scan of the neck showing welldefined lobulated smoothly marginated lesion of altered signal intensity in pre-/left para-esophageal region at subcarinal level measuring approximately 18 mm × 12 mm in size (AP view)
Figure 3.
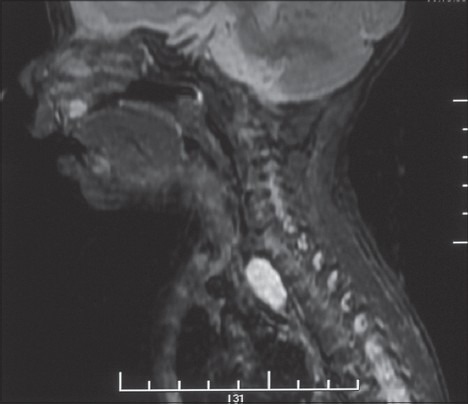
Magnetic resonance imaging scan of the neck showing welldefined lobulated smoothly marginated lesion of altered signal intensity in pre-/left para-esophageal region at subcarinal level measuring approximately 18 mm × 12 mm in size (Lateral view)
The infant underwent a right anterolateral thoracotomy. The cyst was dissected from the adjacent tissues and totally excised. The baby recovered uneventfully. Histopathological examination showed gastric-type mucosa with well-developed sub mucosa, muscularis propria, and serosa. These findings confirmed the radiological diagnosis. On follow-up at 6 months, infant had shown normal growth and development.
Discussion
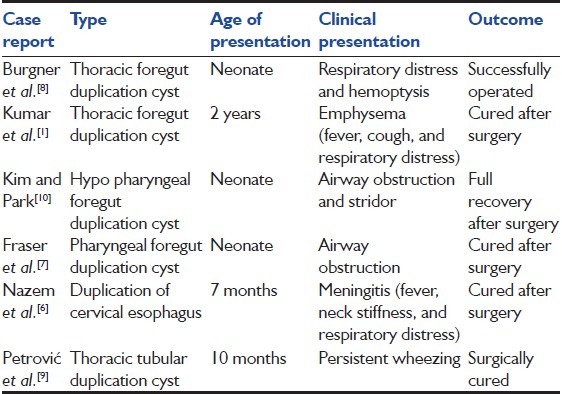
Esophageal duplication cysts result from a defect in the tubulation (vacuolization) of the esophagus, occurring in the 6th week of embryonic life.[3] The incidence of congenital esophageal cyst is estimated to be 1:8200, with male sex predominance (2:1).[4] Esophageal duplication can be associated with other congenital anomalies, such as small intestinal duplication, esophageal atresias distal to the duplication, tracheoesophageal fistulas, and spinal abnormalities, including scoliosis, hemi vertebrae, and fusion.[5] In our patient, there were no associated anomalies. Table 1 shows the recent case reports of foregut duplication cysts in children.[1,6,7,8,9,10]
Table 1.
Recent case reports of foregut duplication cyst
The duplication of the esophagus may be of three forms: (1) A cystic form (most common) that may or may not communicate with the esophageal lumen, (2) a tubular form or (3) a diverticular form.[6] They are usually found in the posterior mediastinum with protrusion into either the right (common) or left thoracic cavity beneath the parietal pleura, with the majority of lesions in the lower half of esophagus.[1] Computer tomography scan and MRI helps in delineating the size, location, extent, and the anatomic association of the mass to other organs. Esophagogram also helps in diagnosis.[3]
After diagnosis, surgery should be done as early as possible to avoid complications such as infection, mass effects, hemorrhage, rupture, or neoplastic degeneration.[2] The treatment of choice is complete surgical excision due to the possibility of degeneration and ease of removal.[2] The prognosis for these lesions is excellent, with no reports in the literature of recurrence following excision.
Conclusion
Foregut duplication cysts of the esophagus are very rare, need strong clinical suspicion for diagnosis, and must be considered in the differential diagnosis of persistent wheezing in infants who do not respond to conventional treatment.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Kumar D, Samujh R, Rao KL. Infected esophageal duplication cyst simulating empyema. Indian Pediatr. 2003;40:423–5. [PubMed] [Google Scholar]
- 2.Stringer MD, Spitz L, Abel R, Kiely E, Drake DP, Agrawal M, et al. Management of alimentary tract duplication in children. Br J Surg. 1995;82:74–8. doi: 10.1002/bjs.1800820126. [DOI] [PubMed] [Google Scholar]
- 3.Shew SB, Holcomb GW., III . Alimentary tract duplications. In: Ashcraft KW, Murphy JP, Holcomb GW III, editors. Pediatric Surgery. 4th ed. Amsterdam: Elsevier; 2005. pp. 543–52. [Google Scholar]
- 4.Arbona JL, Fazzi JG, Mayoral J. Congenital esophageal cysts: Case report and review of literature. Am J Gastroenterol. 1984;79:177–82. [PubMed] [Google Scholar]
- 5.Sethi GK, Marsden J, Johnson D. Duplication cysts of the esophagus. South Med J. 1974;67:616–8. doi: 10.1097/00007611-197405000-00025. [DOI] [PubMed] [Google Scholar]
- 6.Nazem M, Amouee AB, Eidy M, Khan IA, Javed HA. Duplication of cervical oesophagus: A case report and review of literatures. Afr J Paediatr Surg. 2010;7:203–5. doi: 10.4103/0189-6725.70429. [DOI] [PubMed] [Google Scholar]
- 7.Fraser L, Howatson AG, MacGregor FB. Foregut duplication cyst of the pharynx. J Laryngol Otol. 2008;122:754–6. doi: 10.1017/S0022215107001260. [DOI] [PubMed] [Google Scholar]
- 8.Burgner DP, Carachi R, Beattie TJ. Foregut duplication cyst presenting as neonatal respiratory distress and haemoptysis. Thorax. 1994;49:287–8. doi: 10.1136/thx.49.3.287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Petrović S, Ljuština R, Lovrenski J, Milović I, Barišić N. Persistent wheezing as manifestation of esophageal tubular duplication cyst. Ups J Med Sci. 2011;116:216–9. doi: 10.3109/03009734.2011.574165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kim JK, Park KK. Foregut duplication cyst of the hypopharynx: A rare cause of upper airway obstruction. J Pediatr Surg. 2007;42:E5–7. doi: 10.1016/j.jpedsurg.2006.11.007. [DOI] [PubMed] [Google Scholar]