

Abstract
Aims
Nonscaphoid fractures comprise approximately 40% of all carpal fractures. But the exact incidence of these rare injuries is still not clear. Missed or late diagnosis can lead to serious ligamentous disruption and permanent wrist dysfunction.
Methods
A retrospective analysis of wrist X-rays and CT scans were carried out for a period of 3 years. Incidence and associated injuries from this study was compared with literature. A total of 33 patients were included in our study. Both wrist X-rays and CT scans were reviewed individually by two authors. DASH scores were recorded for each patient.
Results
There were 26 male and 7 female patients. Out of 33 patients 13 (35%) were Triquetral fractures, 10 (27%) were Hamate fractures, 5 (14%) were Capitate fractures, 4 (11%) were Lunate fractures, 3 (8%) were Trapezium fractures and 2 (5%) were Pisiform fractures. There were no Trapezoid fractures in our study.
Conclusion
Incidence of nonscaphoid carpal fractures in our study is considerably higher when compared to literature. We propose that high index of suspicion should always be borne in mind when dealing with carpal fractures and detailed examination of wrist should be conducted even when X-rays does not show any obvious bony injuries. CT scans and other specialized images should be judiciously used in areas of suspicion for early diagnosis, to initiate immediate treatment, for early mobilisation and good functional recovery.
Keywords: Nonscaphoid injuries, Carpal injuries, Incidence
1. Introduction
Fall on an outstretched hand and injuring the wrist is a common presentation in A&E and also in Orthopaedic fracture clinic. Carpal fractures are more commonly seen nowadays but it is also easily missed. However the incidence of carpal fractures in UK is not clear. Carpal fractures worldwide account for 8%–19% among all hand injuries.1 Nonscaphoid fractures account for 3.2%–7.7% (Bishop and Beckenbaugh, 1988).1 Scaphoid fractures constitute around 62–87% of all carpal fractures and fractures of carpal bones excluding Scaphoid account for approximately 40% of all carpal fractures.2 Nonscaphoid carpal fractures and the associated injuries which occur with them are frequently missed and difficult to diagnose due to difficult radiologic interpretation and the rarity in presentation. Studies have shown that missed or late diagnosis of these fractures can lead to serious ligamentous disruption and permanent wrist dysfunction.3
This study aims at identifying the exact incidence of nonscaphoid carpal injuries in our institution and compared with literature. Also we looked into associated bony or ligamentous injuries which present along with them and compared the pattern with the literature. Our hypothesis was incidence of nonscaphoid injuries will be higher than what we think.
2. Patients and methods
A retrospective analysis of all wrist X-rays was carried out for a period of 3 years from 2008 to 2011 at Darlington memorial hospital. A total of 33 patients were included in our study. All isolated scaphoid fractures were excluded from this study. We have included all nonscaphoid carpal fractures and associated injuries. CT scans were done for all our 33 patients and were reviewed by authors (AR & PK). Casenotes were accessed to gather data pertaining to admission details, clinic reviews, examination findings, assessment of wrist function and presence of any residual stiffness or pain during discharge. Data including age, gender, occupation, dominant hand, mechanism of injury, type of fracture, presence of associated injuries, management, residual problems and DASH scores were recorded in a proforma and transferred to excel sheet for analysis. We also compared our incidence and associated injuries of these fractures with literature.
3. Results
There were 26 males and 7 female patients. Majority (72%) were right hand dominant. Mean age of those patients were 41.15yrs ± 15.93 yrs (range 10–78 years). 10 patients out of 33 presented with a history of fall on outstretched hand which equaled to 30% of the study population. 4 patients slipped on ice and they all presented during the winter months during snowfall. 5 patients were seen after sports related injury (Golf, Rugby & Football). Among all nonscaphoid carpal fractures, Triquetral fractures are the most commonest found on our study.
Many studies have proven this frequency of Triquetral fracture presentation in literature.
Out of 33 patients 13 (35%) were Triquetral fractures, 10 (27%) were Hamate fractures, 5 (14%) were Capitate fractures, 4 (11%) were Lunate fractures, 3 (8%) were Trapezium fractures and 2 (5%) were Pisiform fractures (Tables 1 and 2). There were no Trapezoid fractures in our study. Vigler et al, 20064 pointed that Trapezoid fractures actually account only for about 0.2% of all carpal fractures and their presentation is very rare.
Table 1.
Number of carpal fractures in our study excluding scaphoid.
| Carpal bones excluding scaphoid | Number |
|---|---|
| Triquetrum | 13 |
| Hamate | 10 |
| Capitate | 5 |
| Lunate | 4 |
| Trapezium | 3 |
| Pisiform | 2 |
| Trapezoid | 0 |
Table 2.
Comparison of incidence between our study and literature.
| Fracture | Our study | Literature |
|---|---|---|
| Triquetrum | 35% | 4–31% |
| Hamate | 27% | 7% |
| Capitate | 14% | 1.3% |
| Lunate | 11% | 1% |
| Trapezium | 8% | 3–5% |
| Pisiform | 5% | 1–2% |
3.1. Triquetral fractures
12–25% of Triquetral injuries are the result of Perilunate fracture dislocation as well as fracture of distal radius and ulna.5–7 Out of our 13 Triquetral fractures eight (8) of them had other associated injuries. 3 patients had associated scaphoid fractures, 4 had fracture of distal radius and ulna, and one patient had transscaphoid transcapitate perilunate dislocation (Fig. 1) and a Lunotriquetral dislocation. One was associated with a volar plate injury of ring finger. Incidence from various studies has quoted between 4 and 31% and our study showed an incidence of 35%.1,2,5,8
Fig. 1.
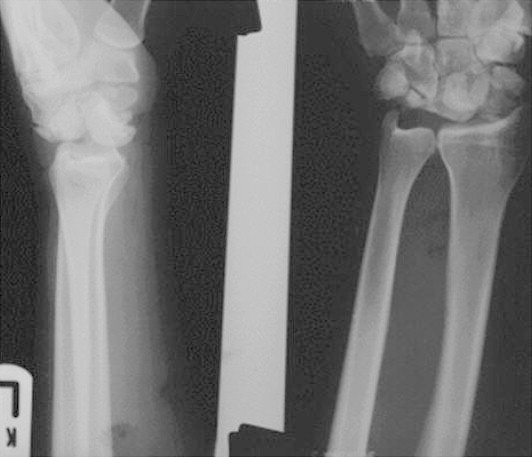
X-ray showing transcaphoid transcapitate transtriquetral fracture with perilunate dislocation.
2 patients had open reduction and internal fixation (one – Comminuted fracture Triquetrum with captitate fracture and another was fracture triquetrum associated with scaphoid fracture, transscaphoid transcapitate perilunate dislocation and a Lunotriquetral dislocation). Remaining 11 patients were managed conservatively. Average DASH score for these patients was 2.8. A total of 5 patients including operated patients developed stiffness at 4 months followup. But they got eventually better after physiotherapy.
3.2. Hamate fractures
These fractures are usually associated with dorsal fracture dislocation of 4th and 5th carpometacarpal (CMC) joints,9 Ulnar nerve injury10 and flexor tendon rupture especially of 4th and 5th 85 fingers.11 There were a total of 10 Hamate fractures out of which 6 patients had associated injuries.
Incidence of this fracture is approximately 7%2 although our study has shown an incidence of 27%.
3 patients had intraarticular fracture of distal radius, 2 with fracture dislocation of 4th and 5th CMC joint (Figs. 3 and 4) and one had subluxation of 3rd and 4th base of metacarpal. Although surgery was done for associated injuries, only one of our Hamate fractures had excision of hook. This was due to non-union and persistent symptoms of this fracture secondary to delayed presentation (4 months) as it was treated as soft tissue injury by local GP. Mean DASH score was 1.5.
Fig. 3.

Hamate fracture with fracture dislocation of 4th and 5th metacarpal base.
Fig. 4.
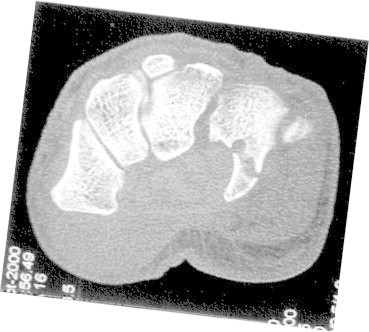
CT-scan showing Hook of Hamate fracture.
3.3. Capitate fractures
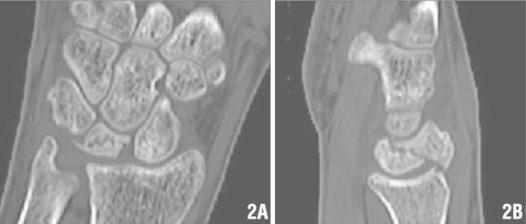
Vigler et al, 2006 have quoted the incidence of this fracture to 1.3% which signifies the rarity of this injury.4 We had 5 Capitate fractures out of 33 accounting to an incidence of 14% among nonscaphoid carpal fractures. Most common associated injury is scaphoid fracture. Our study had 2 patients with associated scaphoid fracture and one with transcaphoid transcapitate perilunate dislocation (Figs. 1 and 2). All isolated fractures were treated conservatively with no residual problems. 2 patients with associated injuries underwent surgery with postop. stiffness at 4 months followup which settled after intense physiotherapy. We haven't had treatment information for one patient as he was not living locally and therefore has to be referred. Average DASH score was 13.
Fig. 2.

Triquetral fracture – X-ray, T2 weighted and T1 weighted MRI.
3.4. Lunate fractures
Hove, 1993 stated that Lunate fractures account for approximately 1% of all carpal fractures.12 Kienbock's disease as a diagnosis should be considered if one is suspecting a Lunate fracture as isolated fractures are very rare. In our study we had 4 Lunate fractures contributing to an incidence of 11%. None of them were diagnosed as Kienbock's disease. Vigler et al, 20064 had noted that 50% of Lunate fractures are associated with injuries to distal radius, carpus or metacarpals.
Our study showed 2 patients with associated scaphoid fracture, one with fracture of distal radius and 2 patients with transscaphoid perilunate dislocation. Operative fixation was carried out for 2 patients with Lunate fracture associated with transcaphoid perilunate dislocation. Fig. 5 shows a CT scan image of Lunate fracture. Surgery for Lunate fracture was not carried for the other 2 patients although scaphoid and distal radius fractures were fixed operatively. All 4 patients developed stiffness postop. and it got improved after intense physiotherapy. Mean DASH score was 2.3.
Fig. 5.
CT-scan showing Lunate fracture.
3.5. Trapezium fractures
Trapezium fracture comprise between 3% and 5% of all carpal fractures.1,2,13 Our study showed an incidence of 8% (3 patients). McGuigan and Culp14 have noticed 4 patients associated with Bennett's fracture and 2 radius fractures out of 11 patients. In our study we had only one with associated clavicle and lateral femoral condyle fracture sustained due to major road traffic accident. He underwent MUA + K wire and intercarpal stabilization for his Trapezium fracture.
Among the other two trapeziums, one was comminuted and the other was isolated injury and both were managed conservatively with no untoward complications during discharge from clinic. We accept the fact that our numbers are less to get any significant associated injuries as mentioned in various other studies. Average DASH score was 1.8.
3.6. Pisiform fractures
Pisiform fractures account for 1–2% of all carpal fractures.15 We had 2 Pisiform fractures in our study contributing to 5% incidence of our study population. Distal radius fracture, perilunate dislocation or additional carpal fractures can occur in 50% of Pisiform fractures.16 There was one associated with distal radius fracture and another was with Hamate fracture. Both were managed conservatively with good results. Mean DASH score was 2.9.
4. Discussion
Our Hospital caters to a population of approximately 130,000. Our Orthopaedic department is one of the tertiary referral centre for Specialist UpperLimb services in that region. We had three Specialist UpperLimb Surgeons and one Specialist Hand Surgeon onsite to accept referrals from other centres, to provide advice and also to conduct exclusive UpperLimb Surgeries regularly.
Incidence of nonscaphoid carpal fractures in our study is considerably higher when compared to literature. This could be due to having an high index of suspicion for these fractures and associated injuries, effective use of specialized radiographic views and CT scans and also immediate availability of specialist hand and UpperLimb Surgeons in our department. Even though our study population is less in number we have to realize the fact that these injuries are quite rare in presentation. This study has proven the importance of conducting a detailed examination of the wrist even when X-rays does not show any obvious bony injuries but presence of persistent symptoms. This will trigger to investigate further using specialized images and to initiate adequate treatment without any delay. As mentioned earlier in this article, because of severe ligamentous damage and disruption this injury can cause, the sooner the diagnosis is made, better the results for the patient and early mobilization can be planned for good functional results. Therefore we would also stress the importance of always looking for any associated injuries with any type of carpal fractures based on our study findings.
Our limitation for this study is small population size and we suggest that further multicentric prospective study with active coordination among all Orthopaedic Surgeons can help in finding out the exact incidence and the outcome of this rare injury.
Author's contributions
AKR and KPK have designed the study. AKR have prepared the proforma. AKR and KPK have reviewed all X-rays and CT scans together. AKR analysed the data and wrote the manuscript. KPK did the final revision of manuscript.
Conflicts of interest
All authors have none to declare.
References
- 1.Bishop A.T., Beckenbaugh R.D. Fracture of hamate hook. J Hand Surg Am. 1988;13:135–139. doi: 10.1016/0363-5023(88)90217-1. [DOI] [PubMed] [Google Scholar]
- 2.Boulas J.H., Milek M.D. Hook of hamate fractures: diagnosis, treatment and complications. Orthop Rev. 1990;29:518–528. [PubMed] [Google Scholar]
- 3.Schadel-Hopfner M., Prommersberger K.J., Eisenschenk A. Treatment of carpal fractures. Recommendations of the hand surgery Group of the German Trauma Society. Unfallchirurgie. 2011;113:741–754. doi: 10.1007/s00113-010-1822-8. [Abstract only – English. Article in German] [DOI] [PubMed] [Google Scholar]
- 4.Vigler M., Aviles A., Lee S.K. Carpal fractures excluding the scaphoid. Hand Clin. 2006;22:501–516. doi: 10.1016/j.hcl.2006.07.007. [DOI] [PubMed] [Google Scholar]
- 5.De Beer J.D., Hudson D.A. Fractures of the triquetrum. J Hand Surg Br. 1987;12:52–53. doi: 10.1016/0266-7681_87_90056-8. [DOI] [PubMed] [Google Scholar]
- 6.Papp S. Carpal bone fractures. Hand Clin. 2010;26:119–127. doi: 10.1016/j.hcl.2009.08.014. [DOI] [PubMed] [Google Scholar]
- 7.Shah M., Viegas S. Fractures of carpal bones excluding scaphoid. J Hand Surg Am. 2002;2:129–140. [Google Scholar]
- 8.Garcia-Elias M. Lippincott Williams & Wilkins; Philadelphia: 2001. Carpal Bone Fractures (Excluding Scaphoid). The Wrist; pp. 173–186. [Google Scholar]
- 9.Borgeskov S., Christiansen B., Kajer A. Fractures of the carpal bones. Acta Orthop Scand. 1966;37:276–287. doi: 10.3109/17453676608989415. [DOI] [PubMed] [Google Scholar]
- 10.Fleege M.A., Jebson P.J., Renfrew D.L. Pisiform fractures. Skeletal Radiol. 1991;20:169–172. doi: 10.1007/BF00241660. [DOI] [PubMed] [Google Scholar]
- 11.Van Onselen E.B.H., Karim R.B., Hage J.J., Ritt M.J.P.F. Prevalence and distribution of hand fractures. J Hand Surg Br. 2003;28:491–495. doi: 10.1016/s0266-7681(03)00103-7. [DOI] [PubMed] [Google Scholar]
- 12.Hove L.M. Fractures of the hand: distribution and relative incidence. Scand J Plast Reconstr Surg. 1993;27:317–319. [PubMed] [Google Scholar]
- 13.Bostock S. Fractures of the carpus and hand (Review Article) Surgery (Oxford) 2010;28:70–74. [Google Scholar]
- 14.McCuigan F.X., Culp R.W. Surgical treatment of intra-articular fractures of the trapezium. J Hand Surg Am. 2002;27:697–703. doi: 10.1053/jhsu.2002.33705. [DOI] [PubMed] [Google Scholar]
- 15.Cohen M.S. Fractures of carpal bones. Hand Clin. 1997;13:587–599. [Abstract only] [PubMed] [Google Scholar]
- 16.Brach P., Goitz R. An update on the management of carpal fractures. J Hand Ther. 2003;16:152–160. doi: 10.1016/s0894-1130(03)80010-8. [DOI] [PubMed] [Google Scholar]