

Abstract
Overweight and obesity have become a global health problem. Obesity and excessive weight gain during pregnancy have a serious impact on maternal, fetal and neonatal outcomes. Pre-conceptional obesity and excessive weight gain during pregnancy are associated with weight gain in women following childbirth leading to associated risks such as metabolic syndrome, cardiovascular disease and diabetes. Long-term risks for the offspring are an increased risk for early cardiovascular events, metabolic syndrome and decreased life expectancy as adults. German health care has not yet adequately responded to this development. There are no clinical guidelines for obesity before, during or after pregnancy, there are no concerted actions amongst midwives, obstetricians, health advisors, politicians and the media. Research projects on effective interventions are lacking although health care concepts would be urgently needed to reduce future metabolic and cardiovascular risks for women and children as well as to minimize the associated costs for the society.
Key words: obesity during pregnancy, metabolic syndrome, diabetes, prevention
Abstract
Zusammenfassung
Adipositas ist inzwischen ein globales gesundheitliches Problem. Adipositas und starke Gewichtszunahme in der Schwangerschaft haben in Industrieländern zu einer Zunahme von Komplikationen während der Gravidität geführt, die mütterliches und kindliches Outcome beeinträchtigen. Nicht nur die präkonzeptionelle Adipositas, sondern auch die übermäßige Gewichtszunahme während der Gravidität sind verantwortlich für eine Gewichtszunahme von Frauen nach der Geburt sowie den assoziierten Risiken wie metabolisches Syndrom, kardiovaskuläre Erkrankungen und Diabetes, aber auch für Langzeitrisiken der Kinder wie Adipositas, höhere Morbidität und frühere Sterblichkeit als Erwachsene. In Deutschland hat man bisher nicht adäquat auf diese Entwicklung reagiert – es gibt weder klinische Richtlinien für die Schwangerschaft, noch konzertierte Aktionen von Hebammen, Geburtsmedizinern, Gesundheitsberatern, Politik und Medien. Untersuchungsprojekte über effektive Interventionen fehlen. Dies alles wäre jedoch erforderlich, um die gesundheitlichen Risiken für Frauen und Kinder sowie die damit verbundenen Kosten für das Gesundheitssystem und letztlich für unsere Gesellschaft einzuschränken.
Schlüsselwörter: Adipositas in der Schwangerschaft, Metabolisches Syndrom, Diabetes, Prävention
Introduction
Overweight and obesity have become epidemic in industrialized nations and even in developing countries 1, 2. Obstetric care givers should be concerned about the increased rate of maternal complications and mortality, the immediate risks for fetus and newborn, the long-term effects on womenʼs health and the life expectancy of future generations.
Ad 1) Overweight or obesity increase the rate of maternal complications and of maternal mortality. Between 2003 and 2005, more than 50 % of maternal deaths in the UK were associated with overweight or obesity 3. Unfortunately, the aetiology and risk factors of maternal deaths are not evaluated in Germany, but there seems to be a similar trend.
Ad 2) Pre-conceptional obesity is associated with an increased rate of congenital defects, regardless of the malformations which are difficult to recognize 4. According to a British cohort study of 287 213 pregnancies, the risk of stillbirth increases from 4/1000 with a normal BMI to 6.9/1000 with a BMI > 30, even after adjusting for diabetes, pre-eclampsia, maternal age, parity or nicotine abuse 5. In a meta-analysis, the risk was judged to be twice as high 6. A dramatic increase in prenatal mortality has been observed in the case of a combination of poor fetal growth and a maternal BMI > 25 with an odd ratio (OR) of 75, and a 95 % confidence interval (CI) of 14–350 7. Furthermore, (iatrogenic) prematurity and the risk of neonatal injuries and hypoglycaemia are increased.
Ad 3) Pregnant women with a high BMI have an increased risk of metabolic syndrome 8, type 2 diabetes and cardiovascular disease in their later life 9.
Ad 4) As concluded from 37 709 birth records from 1950 up to now, cause mortality was increased in offspring of obese mothers (BMI > 30) compared with mothers with normal BMI even after adjustment for maternal age at delivery, socioeconomic status, sex of offspring, current age, birth weight, gestation at delivery, and gestation at measurement of BMI (OR 1.35, 95 % CI 1.17–1.55). Adult offspring of obese mothers also had an increased risk of hospital admission for a cardiovascular event and a higher risk of adverse outcomes 10. They also suffer from health problems in early life, even after adjusting for age, socioeconomic status, gender, birth weight and gestational age at birth 11. Similarly, “programming of a shortened life” was found in the offspring of animals who were exposed to a high caloric diet during pregnancy whereby the effect could be reversed by “exercise” 12.
This overview is alarming. Although there is a German guideline on gestational diabetes of more than 90 pages, there is no guideline on how to prevent or treat obesity during pregnancy, although it is combined with a higher risk for subsequent metabolic syndrome than gestational diabetes 8.
We therefore have accepted the invitation to write this review integrating the expertise from guidelines used in Canada, the US, the UK and the Netherlands (Table 1) 13, 14, 15, 16.
Table 1 Key to evidence statements and grading of recommendations, using the ranking of the Canadian Task Force on Preventive Health Care.13.
| Criteria | Measures |
|---|---|
| I: Evidence obtained from at least one properly randomized controlled trial | A. There is good evidence to recommend the clinical preventive action |
| II-1: Evidence from well-designed controlled trial without randomization | B. There is fair evidence to recommend the clinical preventive action |
| II-2: Evidence from well-designed cohort (prospective or retrospective) or case-control studies, preferably from more than one centre or research group | C. The existing evidence is conflicting and does not allow to make a recommendation for or against use of the clinical preventive action; however, other factors may have an influence on decision-making |
| II-3: Evidence obtained from comparisons between times or places with or without the intervention. Dramatic results in uncontrolled experiments (such as the results of treatment with penicillin in the 1 940 s) could also be included in this category | D. There is fair evidence to recommend against the clinical preventive actionE. There is good evidence to recommend against the clinical preventive action |
| III: Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees | L. There is insufficient evidence (in quantity or quality) to make a recommendation; however, other factors may influence decision-making |
Pre-conceptional Obesity/Interventions
Definition
Obese patients suffer from an elevated body mass index (BMI) which is defined as weight/height (kg/m2). The WHO classifications and corresponding recommendations for weight gain are shown in Table 2 17, 18, 19; recommendations for patients with a BMI greater than 35 are not yet completely based on clear evidence 18. Women should set pregnancy weight gain goals based on their pre-pregnancy BMI or the BMI during the first antenatal visit.
Table 2 Weight classification/WHO 17, with modified criteria of the Canadian guidelines 13 and recommended weight gain according to the Institute of Medicine (IOM) 19, commented by Rasmussen 18, 40.
| Criteria | BMI (kg/m2) | Recommended weight gain | ||
|---|---|---|---|---|
| Course of pregnancy | 2nd and 3rd trimester | |||
| Singleton pregnancy | Twin pregnancy | Singleton pregnancy | ||
| Underweight | < 18,5 | 12.5–18 kg | no information | 0.51 (0.44–0.58) kg/gestational week |
| Normal weight | 18.5–24.9 | 11.5–16 kg | 17–25 kg | 0.42 (0.35–0.50) kg/gestational week |
| Overweight | 25–29.9 | 7–11.5 kg | 14–23 kg | 0.28 (0.23–0.33) kg/gestational week |
| Obesity class I | 30–34.9 | 5–9 kg | 11–19 kg | 0.22 (0.17–0.27) kg/gestational week |
| Obesity class II | 35–39.9 | 5–9 kg | 11–19 kg | 0.22 (0.17–0.27) kg/gestational week |
| Obesity class III | > 40 | 5–9 kg | 11–19 kg | 0.22 (0.17–0.27) kg/gestational week |
Ethnic differences exist 20. The physiologic increase of BMI during pregnancy in about 50 % of women caused by an increase of intra- and extravascular fluid cannot be used as an indicator of body fat 13. In 2009, the Institute of Medicine (IOM) in the US revised the pregnancy recommendations not regarding ethnicity, age, smoking behaviour and parity (Table 2) 19. Trimester-specific recommendations for weight gain were defined and evidence-based absolute and relative risks (RR) for mother and child were finally used for recommendations 21. Morbid obesity identifies patients with a BMI of > 40 kg/m2. Other definitions refer to a weight that is 50–100 % above the ideal weight.
In new guidelines, waist circumference and co-morbidity are used as criteria for weight reduction in obese non-pregnant patients. Regardless of the BMI, women who followed the weight gain guidelines (Table 2) had fewer adverse outcomes (Caesarean delivery, gestational hypertension, birth weight < 2500 g or > 4000 g) 13.
Unfortunately, the identification of women at risk is not routinely followed by interventions. Suggested strategies include behavioural weight loss treatment and counselling regarding exercise, diet, and pregnancy weight gain. So far, no diet offers clear advantages 22. Early counselling by paediatricians, general practitioners, at schools and universities should be promoted. In adolescents between 11 and 15 years of age, a good breakfast and physical activity were the main negative predictors for obesity 23.
Pre-conceptional counselling/interventions
It is critical that women are informed prior to pregnancy about the need to be as healthy as possible before becoming pregnant, which includes having a normal BMI, eating a balanced diet, and participating in regular exercise. According to international guidelines it is encouraged that overweight and obese women who are planning a pregnancy should be referred to pre-conception assessment and counselling (II-B). Weight reduction is essential prior to infertility treatment (I-A). A pregnancy should only be considered with a BMI < 30, and ideally with a BMI < 25 kg/m2 (I-B). In comparison to women of normal weight, women with a BMI > 50 are at risk of pregnancy-induced hypertension (19.7 vs. 4.8 %, OR 1.56; 95 % CI 1.33–1.82), gestational diabetes (21.1 vs. 1.5 %, OR 2.04; 95 % CI 1.74–2.38), shoulder dystocia (7.1 vs. 1.4 %, OR 1.51; 95 % CI 1.05–2.19), Caesarean delivery (60.6 vs. 25.0 %, OR 1.46; 95 % CI 1.29–1.65), long duration of hospital stay (14.3 vs. 4.7 %, OR 1.42; 95 % CI 1.07–1.89), childʼs birth weight ≥ 4000 g (38.0 vs. 11.9 %, OR 1.58; 95 % CI 1.38–1.80) or ≥ 4500 g (16.9 vs. 2.1 %, OR 1.87; 95 % CI 1.57–2.23), for neonatal metabolic problems (8.5 vs. 2.0 %, OR 1.50; 95 % CI 1.20–1.86), for admission of the child (16.9 vs. 7.8 %, OR 1.28; 95 % CI 1.07–1.52) or stillbirth (1.4 vs. 0.2 %, OR 1.68; 95 % CI 1.00–2.82) (I) 24. Long-term maternal risks include osteoarthritis, malignant disease and sleep apnoea. These risks can be limited by regular exercise (II-B) 11. Nutrition consultation should be offered prior to conception 25. Women with a BMI > 50 frequently smoke (II-2) 26 but vice versa, women who stop smoking are at an increased risk of weight gain 27.
First Trimester Risks/Impact for Clinical Practice
Risk of miscarriage
The risk of spontaneous abortion is higher in obese women compared to pregnant women with a normal BMI (OR 3.98; 95 % CI, 1.06–14.92). However, no significant differences have been found in overweight pregnant women (OR 1.02; 95 % CI 0.72–1.45) 28. The risk of miscarriage increases from 13.3 % in normal weight to 38.7 % in obese women (I) 29. The association between obesity and increased rates of spontaneous abortion (OR 1.2, 95 % CI 1.01–1.46) and recurrent (> 3) early miscarriages (OR 3.5, 95 % CI 1.03–12.01) have been described by a retrospective case-control study (II-2) 18. Several cohort studies have shown that overweight and obese women have a higher risk of miscarriage in patients with infertility treatment (I) 29, 30, 31.
Malformations
The rate of malformations is increased in pregnancies of overweight and obese mothers. Although most malformations develop during the first trimester, they are frequently diagnosed at an advanced stage of pregnancy, or even post partum due to decreased visibility 32. Women with a high BMI are at increased risk for neural tube defects (NTD) even after adjusting for diabetes with an OR of 1.22 (95 % CI 0.99–1.49), 1.70 (95 % CI 1.34–2.15) and 3.11 (95 % CI 1.75–5.46) for overweight, obese and severely obese women compared with women and normal BMI (II-1) 33, 34, 35.
Interventions
Obese pregnant women should be counselled with regard to diet, supplements, exercise, and weight gain (II-2-B). Compared to women with a BMI < 27, women with a BMI ≥ 27 have lower serum folate levels even after controlling for folate intake (II) suggesting that obese women should receive higher doses of folate supplementation in order to minimize the risk of fetal NTD. It is uncertain to what extent folic acid > 400 micrograms has a beneficial effect on reducing congenital malformations (III–C) 35.
Pre-pregnancy BMI is inversely associated with serum vitamin D concentrations in pregnant women. Health professionals should therefore check that women with a booking BMI > 30 take 10 micrograms Vitamin D supplementation daily during pregnancy and while breastfeeding (III–C) 15.
Women should set pregnancy weight gain goals based on the BMI as shown in Table 2 at their first antenatal visit. In addition, they should be advised that regular exercise reduces future risks for herself and the offspring unless there are contraindications (II-1-B) 36. Right from the first visits women can be questioned and advised about their diet and if the BMI is > 30 they should be screened for gestational diabetes already at the first visit 15. Exercise habits and nutritional counselling can be a helpful adjunct for women not meeting the weight gain guidelines (I-B) 37. In addition, they may be motivated by knowing that following these guidelines would reduce their risks for a Caesarean, hypertension and abnormal birth weights in their children 36. Up to now, randomized trials on behavioural interventions in obese mothers have not been convincing 38 and a diet restricting protein and any energy intake should be avoided (III–C) 39.
Second and Third Trimester/Impact for Clinical Practice
Obesity is associated with an increased risk of a number of serious adverse outcomes during the second and third trimester including stillbirth, hypertension, pre-eclampsia and gestational diabetes. From the second trimester onwards, weekly weight gain can be used to predict total weight gain 19, 40 and, if necessary, to prompt interventions 41. Re-assessment of maternal weight during the second and third trimester will allow to consider future risks and to make appropriate plans for equipment and personnel required during labour and delivery.
Unexplained stillbirth
Pre-pregnancy obesity is the most prevalent risk factor for unexplained stillbirth 42. In women with a BMI > 35 the OR was 2.79 (95 % CI 1.94–4.02) compared to normal-weight women (II-1) 43. To determine the risks of stillbirth after 22 gestational weeks, 96/6963 population-based studies were selected. A BMI > 25 was the most significant risk factor (more than age and cigarette smoking) and contributed to around 8000 stillbirths per year in studies from 5 countries (II-1) 44. In a recent Scandinavian study, these differences were less pronounced 45. Reasons for the increased risk may include that fetal movements are not recognized, that hyperlipidaemia limits placental blood flow and that sleep apnoea could be associated with fetal hypoxia 46. Pre-conceptional care and audits of perinatal deaths are steps towards reducing stillbirth rate in high-income countries (II-2-C) 47.
Hypertension
An appropriate size of arm cuff should be used for blood pressure measurements during all antenatal consultations. The cuff size used should be documented in the medical records (II-B) 48.
A retrospective study compared 79 005 women stratified by maternal pre-pregnancy weight between 55 and 75 kg, 9355 women between 90 and 120 kg (moderate obesity) and 779 women of more than 120 kg (severe obesity). The risk of pregnancy-induced hypertension rose significantly in moderate obesity: OR 2.38, 95 % CI 2.24–2.52 and severe obesity: OR 3.00, 95 % CI 2.49–3.62. Accordingly, obesity also increased the likelihood that women would experience severe hypertension and HELLP syndrome with an OR of 1.56, 95 % CI 1.35–1.8 in moderate obese and an OR of 2.34, 95 % CI 1.59–3.46 in severely obese women. One in every 10 moderately obese and in every 7 severely obese women had serious complications (II-2) 49. These findings have been confirmed by a prospective study with > 2000 (seriously) obese women (II-1) 50.
Gestational diabetes
Maternal obesity is known to be an important risk factor for gestational diabetes (GDM) with a number of large cohort studies reporting a three-fold increased risk compared to women with a healthy weight 15. In women with a BMI > 35 the OR was 2.6, 95 % CI 2.1–3.4, and increased to an OR of 4.0, 95 % CI 3.1–5.2 in women with a BMI>40 compared to women with a BMI < 30 (II-2) 50. This also increased the risk for children > 4000 g: OR 1.7, 95 % CI 1.4–2.0, for obese mothers: OR 2.0, 95 % CI 1.5–2.3, for very obese pregnant women and for children > 4500 g: OR 2.0, 95 % CI 1.4–3.0 and OR 2.4, 95 % CI 1.5–3.8 (II-1) 29.
Malformations and ultrasound
The ability to evaluate fetal structures is largely dependent on maternal size. Approximately 15 % of normally visible structures will be suboptimally seen in women with a BMI above the 90th percentile; in women with a BMI above the 97.5th percentile, only two thirds of structures are well visualized. As a result, repeat examinations 2 to 4 weeks later or second opinion examinations will reduce the number of poorly viewed fetuses; however, up to 20 % (depending on BMI class) will remain poorly visualized 52. Obstetric care providers consider the BMI when arranging for fetal anatomic assessment, since there is a two-fold increase in the rate of NTD in children of mothers with a high BMI 53, 54 and an increased rate of cardiac malformations, abdominal wall defects, cleft lips and cleft palates 53.
Twin pregnancy
According to a population-based cohort study, a high BMI and excessive weight gain during pregnancy (Table 2) are associated with poorer outcomes in twin pregnancies 55. In a French cohort study of 514 twin pregnancies, obese mothers reported an increased rate of pregnancy-induced hypertension (34.1 % vs. 17.9 %, p = 0.011), pre-eclampsia (27.3 % vs.14.4 %, p = 0.028) and gestational diabetes (22.2 % vs. 4.7 %, p < 0.001) compared to mothers of normal weight (II-2) 56.
Interventions in the second and third trimester
Retrospective cohort studies have shown a 24–60 % reduction in pre-eclampsia in nulliparous women who had increasing levels of exercise both in the year prior to conception and during the pregnancy (II-1) 43, 44. The protective mechanisms include enhanced placental growth and vascularity, prevention and reduction of oxidative stress and correction of vascular endothelial function 45. Exercise reduces medical problems of diabetes – also during pregnancy. More relevant, a 34 % reduction in the development of gestational diabetes was reported in obese women who did not participate in vigorous exercise but who did participate in brisk walking compared to easy pace walking 47. Dietary advice should potentially be continued in relation to gestational diabetes and weight gain. Social stress factors should be discussed and support should be offered appropriately.
Risks and Interventions during Delivery
Overweight and obese pregnant women have an increased rate of Caesarean delivery, shoulder dystocia, problems of anaesthesia, blood loss, thromboembolism and impaired wound healing. Antenatal consultation of pregnant women with a BMI > 30 should be performed and documented. Delivery in a perinatal centre is indicated, as children of obese mothers are more likely to require neonatal intensive care (II–C) 57, 58.
Caesarean section and Vaginal Birth after Caesareans (VBAC)
The risk of Caesarean delivery is increased in obese parturients as analyzed in 24 423 nulliparous women stratified by pre-pregnancy BMI and pregnancy complications. The Caesarean rate was 14.3 % for lean women with a BMI < 19.8, 26.5 % in women with a BMI of 20–25, 32.8 % in women with a BMI between 25 and 30, and 42.6 % in women with a BMI > 35. The risk of Caesareans rose gradually even in women without any other complications: OR 1.4, 95 % CI 1.0–1.8 (BMI of 25–29.9), OR 1.5, 95 % CI 1.1–2.1 (BMI 30–34.9) and OR 3.1, 95 % CI 2.3–4.8 (BMI ≥ 35) 3. Other studies have shown similar results 29, 59.
The increase in the rate of Caesarean deliveries may be partly due to the fact that overweight and obese nulliparous women progress more slowly through the first stage of labour. Obstetricians might be afraid of legal consequences of shoulder dystocia during a vaginal (operative) delivery, although its rate is even lowered in one study 60. The clinical assessment of progression during vaginal delivery is more complex in obese women. If fully dilatation is achieved, transperineal ultrasound allowing to determine the “angle of progression” can facilitate the indication for vaginal (operative) delivery or in other words prevent a Caesarean delivery 61 (III-B), which is combined with high risks of prolonged operative time and wound healing, increased blood loss, endometritis despite antibiotic prophylaxis and thromboembolism 62, 63. Wound infection in women undergoing Caesareans is extremely common in obese women mainly if it is combined with gestational diabetes: OR 9.3, 95 % CI 4.5–19.2; women who require a vertical skin incision have a 12 % rate of wound complications serious enough to require opening the incision 62, 64. Hospitals should ensure that the equipment of the operating theatre can accommodate obese parturients (appropriate instrumentation and operating tables).
Obese women are less likely to be successful in delivering vaginally after previous Caesarean delivery. In women with a BMI < 29 the success rate was 54–68 % 65, 66; the rate is further reduced in heavier women – it was only 13 % in women of > 136 kg 67.
In case of an emergency Caesarean delivery, the time from decision and from incision to delivery is prolonged due to a more complex set-up of anaesthesia and logistics. In case of a subcutaneous layer of > 2 cm, the application of a subcutaneous suture is recommended (I-A) 68.
Some studies suggest that a Caesarean delivery is associated with an increased rate of diabetes and obesity of the child in later life, although these results are still debated 69, 70. A high maternal BMI and/or poor intrauterine growth are associated with obesity and type 2 diabetes in adulthood 71.
Vaginal birth
The increased rate of post-term pregnancies suggests that obesity is associated with impaired myometrial function 43. In a retrospective cohort study in singleton pregnancies from the Danish Medical Birth Registry, women with a preconceptional BMI > 50 required induction of labour more frequently than mothers with BMI ≤ 50: 38.4 % vs. 13.2 % with a RR of 2.91 and a 95 % CI of 2.33–3.63. Requiring oxytocin during labour was also increased: RR 1.41, 95 % CI: 1.13–1.77 (II-1) 26. Examination of the case records showed that the rate of emergency Caeesareans was nearly doubled (21 % vs. 12 %).
The precise risks of secondary Caesareans depend on the knowledge and skills of the whole obstetric team how to balance oxytocin, encouragement and decisions during first and second stage of labour including the use of transperineal ultrasound.
In nulliparous women with spontaneous onset of labour and a high BMI, the first stage of labour is prolonged while the second stage may be shorter which should be considered for future protocols. External monitoring of fetal heart rate (FHR) and contractions is impaired and may require internal monitoring (III–C). Recently, electromyographic monitoring was performed in obese women showing a better recording quality compared to conventional tocography 72.
In a cohort of 126 080 pregnancies without hypertension or diabetes obese women (BMI > 30) had an increased risk of fetal macrosomia with an OR of 1.4 (95 % CI 1.2 to 1.7) (II-1). Nevertheless, the risk for shoulder dystocia did not increase 73. Similar results were found in another cohort 74.
It has been reported that the estimated fetal weight (> 4000 g, delivery within 3 days) was greater than the actual birth weight in 77 % of obese women 75. When fetal macrosomia was incorrectly predicted, the rate of Caesarean deliveries was significantly greater compared to normal fetal weight prediction: 42.3 % versus 24.3 %, RR 1.74 (95 % CI, 1.09 to 2.78) (II-1) 76. Although fetal macrosomia is a risk factor for shoulder dystocia, the absolute risk of a severe shoulder dystocia associated with permanent impairment or death, remains low. Considering the sensitivity and specificity of ultrasound to predict a birth weight > 4500 g, 3695 non-diabetic women would have to undergo a Caesarean in order to prevent one plexus paralysis 77!
Injuries of the maternal pelvic floor have not yet been studied with regard to maternal BMI and seem to depend rather on fetal size than on the phenomenon of obesity.
Complications during delivery
Both immobility and obesity are independent risk factors of thromboembolism; in combination, however, they may pose a much greater risk. This interaction has been demonstrated by a case-control study that reported an OR of 62.3 (95 % CI 11.5–337.6) for antenatal venous thromboembolism (VTE) and 40.1 (95 % CI 8.0–201.5) for postnatal VTE in women with a BMI ≥ 25 where there was evidence of immobilisation, compared with women with a BMI < 25 and no immobilisation. In contrast, women with a BMI ≥ 25 without evidence of immobilisation had a much lower OR of 1.8 (95 % CI 1.3–2.4) for antenatal VTE and 2.4 (95 % CI 1.7–3.3) for postnatal VTE 78.
A case-control study conducted in the United Kingdom reported that a BMI ≥ 30 was associated with an OR of 2.65 (95 % CI 1.09–6.45) for antenatal pulmonary thromboembolism (PTE) (II) 15.
Obese women requiring pharmacological thromboprophylaxis should be prescribed appropriate doses of low molecular weight heparin (LMWH) according to national guidelines and additional risk factors and should be encouraged to mobilize as early as possible following childbirth (IIB) 15. Women with a BMI ≥ 30 who have two or more additional persisting risk factors should be given graduated compression stockings in addition to LMWH mainly in the case of immobilisation (III–C) 15.
Regardless of BMI, all women undergoing Caesarean delivery should be offered a single prophylactic dose of first generation cephalosporin or ampicillin to reduce postoperative infections (endometritis, urinary tract or wound infections) (I) and in obese women the dose should be adapted (IIIC).
Obese mothers have an increased risk of postpartum haemorrhage, post partum anaemia and the need for blood transfusion, therefore active management during the third stage of labour is recommended 15, 57.
Obstetric anaesthesia
Rates of difficult or failed intubation are increased in obese patients. A 6-year review of failed intubations in obstetric patients with an average BMI of 33 in a region of the United Kingdom reported 36/8970 (1/249) cases of failed intubation 79. The equipment and expertise required to manage a difficult intubation should be readily available. In obese patients, also the risk of epidural failure is increased. The initial failure rate for epidural catheter placement was reported to be 42 % 80; multiple attempts at catheter placement may be required in up to 75 % of very obese patients 62. It is not yet clear, whether ultrasound diagnosis may facilitate the placement in these women 81. According to a Danish cohort study, regional anaesthesia was impossible in 25 % of all women with a BMI > 50 26. In the case of failed epidural or spinal anaesthesia, the patient has to be treated with general anaesthesia; however, this is associated with elevated risks for both mother and child. Therefore, early epidural anaesthesia during the first stage of labour should be considered in order to avoid time delay in case of emergency (III–C).
Postnatal Care and Follow-up after pregnancy
Breastfeeding
Obesity is associated with low breastfeeding initiation and maintenance rates 82, 83. Obese women should receive dedicated breastfeeding support regarding the benefits, initiation and maintenance of breastfeeding (II-2). Anatomical problems during breastfeeding and reduced prolactin levels could play a role why breastfeeding is more difficult 84. Randomized trials have shown that prenatal breastfeeding support may increase the rate and duration of breastfeeding (I-A) 85. Reduced cognitive abilities were demonstrated up to school age in the children of mothers with a BMI > 30; the mechanisms – and whether it is a reduced breastfeeding rate- are still unclear 86.
Lifestyle interventions/surgical and pharmacological therapy
A small number of randomized trials have assessed the effect of postnatal lifestyle interventions on weight reduction. Maternity services need to identify what services are available locally to provide this follow up. A Swedish population-based study of > 150 000 women examined the inter-pregnancy weight gain showing that an increased BMI in the second pregnancy was linearly correlated to the risk of pre-eclampsia, gestational diabetes, macrosomia, Caesarean delivery and stillbirth (II-2) 77.
An inter-pregnancy weight loss of 4.5 kg in > 4000 mothers showed a reduction of gestational diabetes by 40 % in the next pregnancy 78. Women with a BMI > 30 should be offered professional advice to modify dietary and physical activity leading to weight loss (I-A) 87, 88, 89. Several systematic reviews of randomized and non-randomized trials 4 form the basis for evidence-based recommendations 84, 85. Diet and increased activity contribute to weight loss; diet alone bears the risk that fat-free tissue will be reduced, which is prevented with parallel activity 90. Unfortunately, obese mothers are less aware of their pregnancy risks compared to women with gestational diabetes (15.5 vs. 75.0 %, p < 0.01) and are frequently not sufficiently informed about modifications of their lifestyles 91.
In a randomized trial (“lifestyle in pregnancy”, LIP study), 360 obese pregnant women were offered life style interventions during pregnancy such as regular dietary counselling by trained dieticians and physical activity such as to be moderately active 30–60 min/day equipped with a pedometer, free full-time membership in a fitness centre with physiotherapists for 1 h each week. A total of 304 (84 %) women were followed up until delivery. The intervention group had a significantly lower gestational weight gain (GWG) compared with the control group of 7.0 (4.7–10.6) vs. 8.6 kg (5.7–11.5; p = 0.01). The IOM recommendations on GWG were exceeded in 35.4 % of women in the intervention group compared with 46.6 % in the control group (p = 0.058). Overall, the obstetric outcomes between the two groups were not significantly different 4.
Investigations during breastfeeding are lacking. A meta-analysis demonstrated that women with obesity and gestational diabetes have an increased risk of type-2 diabetes compared to women without gestational diabetes (I): RR 7.43, 95 % CI 4.79–11.51 92 until 5 years after birth 93.
Systematic reviews show that obese patients may benefit from surgical interventions such as bariatric or gastric bypass surgery 94. Whether it can be concluded to recommend surgery for pre-pregnancy weight loss and to refer patients to pre-pregnancy surgery is contradictory. Patients should be informed that surgical (band dislocation, maternal bowel obstruction) and internal (nutrient deficiency, severe growth restriction) problems may arise during pregnancy 95. After inserting a duodenal bypass between two pregnancies, some offspring showed reduced rates of obesity until puberty from 60 % to 35 % which was more pronounced in boys than in girls 96. More recently, 340 followed children of 230 mothers who had undergone bariatric surgery showed no significant differences before and after maternal surgery; by 10 years of age, girls even had a higher weight compared to controls. Consequently, obese women should be informed risks and benefits (II–D) 97.
With regard to pharmacological treatment, a double blind study was performed on 564 non-pregnant patients with a BMI between 30 and 40 using different doses of the glucagon-like peptide-1 receptor agonist liraglutide (1.2 mg, 1.8 mg, 2.4 mg, and 3.0 mg) as well as orlistat and a placebo. All patients followed the same diet and fitness program. Weight loss in patients with liraglutide was more pronounced (up to 4.4 kg,95 % CI 2.9–6.0) compared to those taking the placebo and orlistat; 76 % of patients taking 3 mg liraglutide vs. 30 % in the placebo group had a weight loss of more than 5 %. In addition, they had a lower blood pressure and the prevalence of pre-diabetes was reduced (I-A) 98. It is currently investigated to what extent liraglutide may also prevent pre-diabetes (I) 99.
Regional and national interventions
The problems combined with obesity before, during and after pregnancy require guidelines at a local and national level 100. The Royal College of Obstetrics and Gynaecology (RCOG) recommends that maternity units should have accessible multidisciplinary guidelines which are communicated to individuals and organisations providing care to pregnant women with a booking BMI > 30. These guidelines should include facilities and equipment, care in pregnancy, place of birth and care in labour, provision of anaesthetic services, management of obstetric emergencies and postnatal follow-up.
In Germany, there are no systematic investigations with respect to the early diagnosis or interventions. There is not even a guideline. National campaigns and intervention strategies are urgently needed. It has been shown that maternal obesity is recognized as a public problem, but that counselling frequently fails if the counsellors are also overweight 101. Increased parity, low income and insufficient education are associated with maternal obesity 102. This makes efficient interventions more complex. Stigmatisation of patients should be avoided, but the consequences of further weight gain should be pointed out. Gynaecologists and midwives are inadequately trained for structured interviews and effective nutritional counselling 103. A referral to a dietician might help to concentrate on diet and lifestyle, rather than only on weight gain. Even in countries with well-established guidelines, the required information is not provided to patients in more than 25 % of cases 104. Self-assessment is difficult, as 74 % of obese women estimate their BMI to be lower and 64 % the permitted weight gain to be higher 105. A meta-analysis of 12 international studies showed that a so-called sugar-tax can lead to a weight reduction in the population (II-B) 106.
Public “campaigns” on TV and in social media could support the efforts of patients and their caregivers. In English-spoken media, there are already more than 1500 informative and interactive iTunes and Google Plays on the topic of pregnancy (“shared maternity care”) 107. Health care politicians could use these opportunities. Evidence-based interventions and respectful communication are essential since the costs may rise by around 2 trillion pounds annually in the US and England, and are expected to increase to more than 50 trillion pounds per year by 2020 108. Clinical admissions of overweight, obese and very obese women are increased by 16 %, 45 % and 88 % respectively. The average additional costs during pregnancy were 350.75 (95 % CI £284.82–416.69) pounds for women with a BMI > 40 (II-2) 108.
Conclusions for Clinical Practice
The time before, during and after pregnancy should be viewed a window of opportunities to minimize the short- and long-term health risks for women and their children at an early stage in their life span. Pragmatic proposals are suggested according to international studies (Fig. 1). No other pregnancy risk is associated with such a high rate of miscarriage and stillbirth. Both mother and child suffer irreversible short- and long-term risks.
Fig. 1.
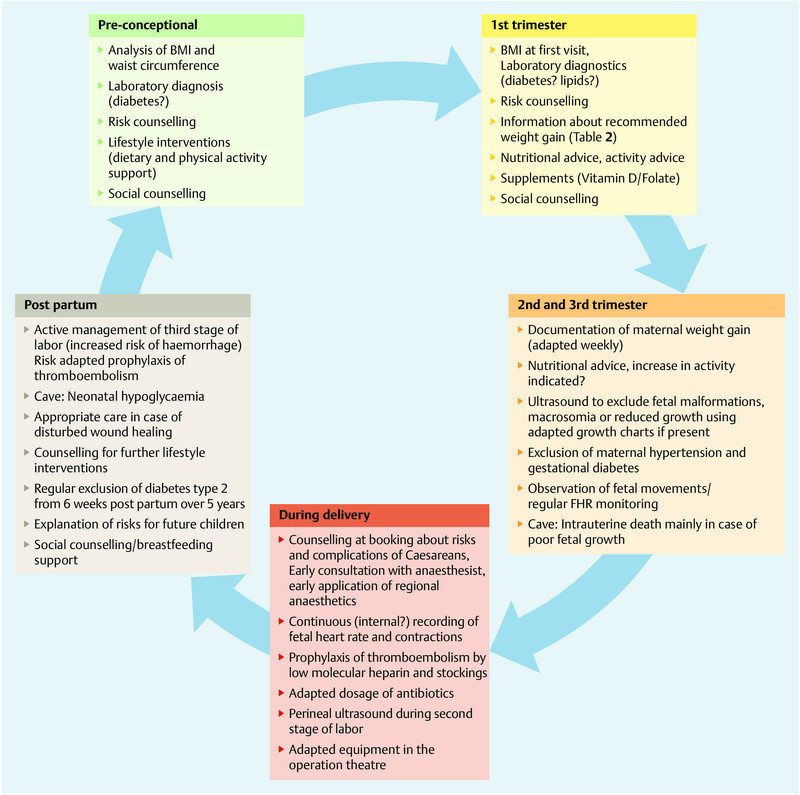
Pragmatic flow chart of treatment of overweight and obese women pre-, peri- and postnatally.
Obstetric medicine is a predominantly preventive discipline; otherwise it would be called obstetric surgery. It is doubtful whether efforts, which are offered by individual colleagues or professional organizations may (want to) cope with this problem. Therefore patients have to continue to rely on their own initiatives or to wait for social and political efforts, which usually take too much time since nobody invests in the virtual value of future health. Concerted actions of politicians, media, general practitioners, midwives and obstetricians are urgently needed as in other fields of our predominantly human, intellectual and preventive specialty with a view to future generation.
Footnotes
Conflict of Interest None.
Supporting Information
German supporting informations for this article
References
- 1.WHO . Geneva, Switzerland: World Health Organization; 2006. Global NCD Infobase. [Google Scholar]
- 2.Flegal K M, Carroll M D, Kit B K. et al. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA. 2012;307:491–497. doi: 10.1001/jama.2012.39. [DOI] [PubMed] [Google Scholar]
- 3.Dietz P M, Callaghan W M, Morrow B. et al. Population-based assessment of the risk of primary cesarean delivery due to excess prepregnancy weight among nulliparous women delivering term infants. Matern Child Health J. 2005;9:237–244. doi: 10.1007/s10995-005-0003-9. [DOI] [PubMed] [Google Scholar]
- 4.Vinter C A, Jensen D M, Ovesen P. et al. The LiP (Lifestyle in Pregnancy) study: a randomized controlled trial of lifestyle intervention in 360 obese pregnant women. Diabetes Care. 2011;34:2502–2507. doi: 10.2337/dc11-1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sebire N J, Jolly M, Harris J P. et al. Maternal obesity and pregnancy outcome: a study of 287,213 pregnancies in London. Int J Obes Relat Metab Disord. 2001;25:1175–1182. doi: 10.1038/sj.ijo.0801670. [DOI] [PubMed] [Google Scholar]
- 6.Chu S Y, Bachman D J, Callaghan W M. et al. Association between obesity during pregnancy and increased use of health care. N Engl J Med. 2008;358:1444–1453. doi: 10.1056/NEJMoa0706786. [DOI] [PubMed] [Google Scholar]
- 7.Frøen J F, Gardosi J O, Thurmann A. et al. Restricted fetal growth in sudden intrauterine unexplained death. Acta Obstet Gynecol Scand. 2004;83:801–807. doi: 10.1111/j.0001-6349.2004.00602.x. [DOI] [PubMed] [Google Scholar]
- 8.Ijäs H, Morin-Papunen L, Keränen A K. et al. Pre-pregnancy overweight overtakes gestational diabetes as a risk factor for subsequent metabolic syndrome. Eur J Endocrinol. 2013;169:605–611. doi: 10.1530/EJE-13-0412. [DOI] [PubMed] [Google Scholar]
- 9.Alberti K G, Zimmet P, Shaw J. The metabolic syndrome – a new worldwide definition. Lancet. 2005;366:1059–1062. doi: 10.1016/S0140-6736(05)67402-8. [DOI] [PubMed] [Google Scholar]
- 10.Reynolds R M, Allan K M, Raja E A. et al. Maternal obesity during pregnancy and premature mortality from cardiovascular event in adult offspring: follow-up of 1323275 person years. BMJ. 2013;347:f4539. doi: 10.1136/bmj.f4539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Salem S Y Kessous R Pariente G et al. Obesity in pregnancy: whatʼs next? Long-term cardiovascular morbidity in a follow-up period of more than a decade Am J Obstet Gynecol 20142101. Suppl.S45S68 [DOI] [PubMed] [Google Scholar]
- 12.Antony K Ma J Mitchell K et al. Excess gestational weight gain (GWG) is associated with alterations in metabolic function of the microbiome Am J Obstet Gynecol 20142101. Suppl.S45S69 [Google Scholar]
- 13.Davies G A, Maxwell C, McLeod L. et al. Society of Obstetricians and Gynaecologists of Canada . SOGC Clinical Practice Guidelines: Obesity in pregnancy. No. 239, February 2010. Int J Obstet Gynecol. 2010;32:167–173. doi: 10.1016/j.ijgo.2010.03.008. [DOI] [PubMed] [Google Scholar]
- 14.ACOG Committee opinion no. 549: Obesity in pregnancy. Obstet Gynecol. 2013;121:213–217. doi: 10.1097/01.aog.0000425667.10377.60. [DOI] [PubMed] [Google Scholar]
- 15.CMACE/RCOG Guideline. Management of women with obesity in pregnancy. Jointly published by the Centre for Maternal and Child Enquiries and the Royal College of Obstetricians and Gynaecologists. London. 2010.
- 16.NVOG Obesitas en zwangerschapOnline:http://www.nvog.nllast access: 2009
- 17.WHO . WHO technical report series; 2000. Obesity: preventing and managing the global epidemic; p. 894. [PubMed] [Google Scholar]
- 18.Rasmussen K M, Catalano P M, Yaktine A L. New guidelines for weight gain during pregnancy: what obstetrician/gynecologists should know. Curr Opin Obstet Gynecol. 2009;21:521–526. doi: 10.1097/GCO.0b013e328332d24e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Institute of Medicine (IOM) . Washington: National Research Council; 2009. Weight gain during pregnancy: re-examining the guidelines. Committee to reexamine IOM pregnancy weight guidelines. [Google Scholar]
- 20.Deurenberg P, Andreoli A, Borg P. et al. The validity of predicted body fat percentage from body mass index and from impedance in samples of five European populations. Eur J Clin Nutr. 2001;55:973–979. doi: 10.1038/sj.ejcn.1601254. [DOI] [PubMed] [Google Scholar]
- 21.Viswanathan M, Siega-Riz A M, Moos M K. Research Triangle Park, NC: RTI International–University of North Carolina Evidence-based Practice Center; 2008. Outcomes of maternal weight gain. Evidence report/technology assessment, number 168 (AHRQ Publication No. 08-E09) [Google Scholar]
- 22.Jensen M D, Ryan D H. New obesity guidelines: promise and potential. JAMA. 2014;311:23–24. doi: 10.1001/jama.2013.282546. [DOI] [PubMed] [Google Scholar]
- 23.Haug E, Rasmusssen M, Samdal O. et al. HBSC Obesity Writing Group . Overweight in school-aged children and its relationship with demographic and lifestyle factors: results from the WHO-Collaborative Health Behaviour in School-aged Children (HBSC) study. Int J Public Health. 2009;54 02:167–179. doi: 10.1007/s00038-009-5408-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Crane J M, Murphy P, Burrage L. et al. Maternal and perinatal outcomes of extreme obesity in pregnancy. J Obstet Gynaecol Can. 2013;35:606–611. doi: 10.1016/S1701-2163(15)30879-3. [DOI] [PubMed] [Google Scholar]
- 25.Olafsdottir A S, Skuladottir G V, Thorsdottir I. et al. Maternal diet in early and late pregnancy in relation to weight gain. Int J Obes (Lond) 2006;30:492–499. doi: 10.1038/sj.ijo.0803184. [DOI] [PubMed] [Google Scholar]
- 26.Bonnesen B, Secker N J, Møller L K. et al. Pregnancy outcomes in a cohort of women with a preconception body mass index > 50 kg/m(2) Acta Obstet Gynecol Scand. 2013;92:1111–1114. doi: 10.1111/aogs.12174. [DOI] [PubMed] [Google Scholar]
- 27.Olafsdottir A S, Skuladottir G V, Thorsdottir I. et al. Combined effects of maternal smoking status and dietary intake related to weight gain and birth size parameters. BJOG. 2006;113:1296–1302. doi: 10.1111/j.1471-0528.2006.01077.x. [DOI] [PubMed] [Google Scholar]
- 28.Metwally M, Saravelos S H, Ledger W L. et al. Body mass index and risk of miscarriage in women with recurrent miscarriage. Fertil Steril. 2010;94:290–295. doi: 10.1016/j.fertnstert.2009.03.021. [DOI] [PubMed] [Google Scholar]
- 29.Bellver J, Rossal L P, Bosch E. et al. Obesity and the risk of spontaneous abortion after oocyte donation. Fertil Steril. 2003;79:1136–1140. doi: 10.1016/s0015-0282(03)00176-6. [DOI] [PubMed] [Google Scholar]
- 30.Fedorcsák P, Storeng R, Dale P O. et al. Obesity is a risk factor for early pregnancy loss after IVF or ICSI. Acta Obstet Gynecol Scand. 2000;79:43–48. [PubMed] [Google Scholar]
- 31.Wang J X, Davies M J, Norman R J. Obesity increases the risk of spontaneous abortion during infertility treatment. Obes Res. 2002;10:551–554. doi: 10.1038/oby.2002.74. [DOI] [PubMed] [Google Scholar]
- 32.Dashe J S, McIntire D D, Twickler D M. Effect of maternal obesity on the ultrasound detection of anomalous fetuses. Obstet Gynecol. 2009;113:1001–1007. doi: 10.1097/AOG.0b013e3181a1d2f5. [DOI] [PubMed] [Google Scholar]
- 33.Shaw G M, Velie E M, Schaffer D. Risk of neural tube defect-affected pregnancies among obese women. JAMA. 1996;275:1093–1096. doi: 10.1001/jama.1996.03530380035028. [DOI] [PubMed] [Google Scholar]
- 34.Waller D K, Mills J L, Simpson J L. et al. Are obese women at higher risk for producing malformed offspring? Am J Obstet Gynecol. 1994;170:541–548. doi: 10.1016/s0002-9378(94)70224-1. [DOI] [PubMed] [Google Scholar]
- 35.Werler M M, Louik C, Shapiro S. et al. Prepregnant weight in relation to risk of neural tube defects. JAMA. 1996;275:1089–1092. doi: 10.1001/jama.1996.03530380031027. [DOI] [PubMed] [Google Scholar]
- 36.Davies G A, Wolfe L A, Mottola M F. et al. Exercise in pregnancy and the postpartum period. J Obstet Gynaecol Can. 2003;25:516–529. doi: 10.1016/s1701-2163(16)30313-9. [DOI] [PubMed] [Google Scholar]
- 37.Piirainen T, Isolauri E, Lagström H. et al. Impact of dietary counselling on nutrient intake during pregnancy: a prospective cohort study. Br J Nutr. 2006;96:1095–1104. doi: 10.1017/bjn20061952. [DOI] [PubMed] [Google Scholar]
- 38.Polley B A, Wing R R, Sims C J. Randomized controlled trial to prevent excessive weight gain in pregnant women. Int J Obes Relat Metab Disord. 2002;26:1494–1502. doi: 10.1038/sj.ijo.0802130. [DOI] [PubMed] [Google Scholar]
- 39.Kramer M S Kakuma R Energy and protein intake in pregnancy Cochrane Database Syst Rev 20034CD000032 [DOI] [PubMed] [Google Scholar]
- 40.Rasmussen K M, Abrams B, Bodnar L M. et al. Recommendations for weight gain during pregnancy in the context of the obesity epidemic. Obstet Gynecol. 2010;116:1191–1195. doi: 10.1097/AOG.0b013e3181f60da7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chmitorz A, von Kries R, Rasmussen K M. et al. Do trimester-specific cutoffs predict whether women ultimately stay within the Institute of Medicine/National Research Council guidelines for gestational weight gain? Findings of a retrospective cohort study. Am J Clin Nutr. 2012;95:1432–1437. doi: 10.3945/ajcn.111.033704. [DOI] [PubMed] [Google Scholar]
- 42.Fretts R C. Etiology and prevention of stillbirth. Am J Obstet Gynecol. 2005;193:1923–1935. doi: 10.1016/j.ajog.2005.03.074. [DOI] [PubMed] [Google Scholar]
- 43.Cedergren M I. Maternal morbid obesity and the risk of adverse pregnancy outcome. Obstet Gynecol. 2004;103:219–224. doi: 10.1097/01.AOG.0000107291.46159.00. [DOI] [PubMed] [Google Scholar]
- 44.Flenady V, Koopmans L, Middleton P. et al. Major risk factors for stillbirth in high-income countries: a systematic review and meta-analysis. Lancet. 2011;377:1331–1340. doi: 10.1016/S0140-6736(10)62233-7. [DOI] [PubMed] [Google Scholar]
- 45.Waldenström U, Aasheim V, Nilsen B V. et al. Adverse pregnancy outcomes related to advanced maternal age compared with smoking and being overweight. Obstet Gynecol Clin North Am. 2014;123:104–112. doi: 10.1097/AOG.0000000000000062. [DOI] [PubMed] [Google Scholar]
- 46.Thomas J, Paranjothy S, James D. National cross sectional survey to determine whether the decision to delivery interval is critical in emergency caesarean section. BMJ. 2004;328:665. doi: 10.1136/bmj.38031.775845.7C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Flenady V, Middleton P, Smith G C. et al. Stillbirths: the way forward in high-income countries. Lancet. 2011;377:1703–1717. doi: 10.1016/S0140-6736(11)60064-0. [DOI] [PubMed] [Google Scholar]
- 48.Maxwell M H, Waks A U, Schroth P C. et al. Error in blood-pressure measurement due to incorrect cuff size in obese patients. Lancet. 1982;2:33–36. doi: 10.1016/s0140-6736(82)91163-1. [DOI] [PubMed] [Google Scholar]
- 49.Robinson H E, OʼConnell C M, Joseph K S. et al. Maternal outcomes in pregnancies complicated by obesity. Obstet Gynecol. 2005;106:1357–1364. doi: 10.1097/01.AOG.0000188387.88032.41. [DOI] [PubMed] [Google Scholar]
- 50.Weiss J L, Malone F D, Emig D. et al. Obesity, obstetric complications and cesarean delivery rate – a population-based screening study. Am J Obstet Gynecol. 2004;190:1091–1097. doi: 10.1016/j.ajog.2003.09.058. [DOI] [PubMed] [Google Scholar]
- 51.Berger H, Crane J, Farine D. et al. Screening for gestational diabetes mellitus. J Obstet Gynaecol Can. 2002;24:894–912. doi: 10.1016/s1701-2163(16)31047-7. [DOI] [PubMed] [Google Scholar]
- 52.Wolfe H M, Sokol R J, Martier S M. et al. Maternal obesity: a potential source of error in sonographic prenatal diagnosis. Obstet Gynecol. 1990;76(3 Pt 1):339–342. [PubMed] [Google Scholar]
- 53.Nuthalapaty F S Rouse D J The impact of obesity on obstetrical practice and outcome Clin Obstet Gynecol 200447898–913.discussion 980–981 [DOI] [PubMed] [Google Scholar]
- 54.Anderson J L, Waller D K, Canfield M A. et al. Maternal obesity, gestational diabetes, and central nervous system birth defects. Epidemiology. 2005;16:87–92. doi: 10.1097/01.ede.0000147122.97061.bb. [DOI] [PubMed] [Google Scholar]
- 55.Yeh J, Shelton J A. Association of pre-pregnancy maternal body mass and maternal weight gain to newborn outcomes in twin pregnancies. Acta Obstet Gynecol Scand. 2007;86:1051–1057. doi: 10.1080/00016340701417026. [DOI] [PubMed] [Google Scholar]
- 56.Fox N S, Roman A S, Saltzman D H. et al. Obesity and adverse pregnancy outcomes in twin pregnancies. J Matern Fetal Neonatal Med. 2014;27:355–359. doi: 10.3109/14767058.2013.818654. [DOI] [PubMed] [Google Scholar]
- 57.Usha Kiran T S, Hemmadi S, Bethel J. et al. Outcome of pregnancy in a woman with an increased body mass index. BJOG. 2005;112:768–772. doi: 10.1111/j.1471-0528.2004.00546.x. [DOI] [PubMed] [Google Scholar]
- 58.Bianco A T, Smilen S W, Davis Y. et al. Pregnancy outcome and weight gain recommendations for the morbidly obese woman. Obstet Gynecol. 1998;91:97–102. doi: 10.1016/s0029-7844(97)00578-4. [DOI] [PubMed] [Google Scholar]
- 59.Dempsey J C, Ashiny Z, Qiu C F. et al. Maternal pre-pregnancy overweight status and obesity as risk factors for cesarean delivery. J Matern Fetal Neonatal Med. 2005;17:179–185. doi: 10.1080/14767050500073456. [DOI] [PubMed] [Google Scholar]
- 60.Steinfeld J D, Valentine S, Lerer T. et al. Obesity-related complications of pregnancy vary by race. J Matern Fetal Med. 2000;9:238–241. doi: 10.1002/1520-6661(200007/08)9:4<238::AID-MFM10>3.0.CO;2-5. [DOI] [PubMed] [Google Scholar]
- 61.Kalache K D, Dückelmann A M, Michaelis S A. et al. Transperineal ultrasound imaging in prolonged second stage of labor with occipitoanterior presenting fetuses: how well does the ‘angle of progression predict the mode of delivery? Ultrasound Obstet Gynecol. 2009;33:326–330. doi: 10.1002/uog.6294. [DOI] [PubMed] [Google Scholar]
- 62.Perlow J H, Morgan M A. Massive maternal obesity and perioperative cesarean morbidity. Am J Obstet Gynecol. 1994;170:560–565. doi: 10.1016/s0002-9378(94)70227-6. [DOI] [PubMed] [Google Scholar]
- 63.Myles T D, Gooch J, Santolaya J. Obesity as an independent risk factor for infectious morbidity in patients who undergo cesarean delivery. Obstet Gynecol. 2002;100(5 Pt 1):959–964. doi: 10.1016/s0029-7844(02)02323-2. [DOI] [PubMed] [Google Scholar]
- 64.Schneid-Kofman N, Sheiner E, Levy A. et al. Risk factors for wound infection following cesarean deliveries. Int J Gynaecol Obstet. 2005;90:10–15. doi: 10.1016/j.ijgo.2005.03.020. [DOI] [PubMed] [Google Scholar]
- 65.Durnwald C P, Ehrenberg H M, Mercer B M. The impact of maternal obesity and weight gain on vaginal birth after cesarean section success. Am J Obstet Gynecol. 2004;191:954–957. doi: 10.1016/j.ajog.2004.05.051. [DOI] [PubMed] [Google Scholar]
- 66.Juhasz G, Gyamfi C, Gyamfi P. et al. Effect of body mass index and excessive weight gain on success of vaginal birth after cesarean delivery. Obstet Gynecol. 2005;106:741–746. doi: 10.1097/01.AOG.0000177972.32941.65. [DOI] [PubMed] [Google Scholar]
- 67.Chauhan S P, Magann E F, Carroll C S. et al. Mode of delivery for the morbidly obese with prior cesarean delivery: vaginal versus repeat cesarean section. Am J Obstet Gynecol. 2001;185:349–354. doi: 10.1067/mob.2001.116729. [DOI] [PubMed] [Google Scholar]
- 68.Royal College of Obstetricians and Gynaecologists (RCOG) . London: RCOG; 2004. Caesarean section. [Google Scholar]
- 69.Goldani M Z, Barieri M A, da Silva A A. et al. Cesarean section and increased body mass index in school children: two cohort studies from distinct socioeconomic background areas in Brazil. Nutr J. 2013;12:104. doi: 10.1186/1475-2891-12-104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Hermansson H, Hoppu U, Isolauri E. Elective caesarean section is associated with low adiponectin levels in cord blood. Neonatology. 2014;105:172–174. doi: 10.1159/000357178. [DOI] [PubMed] [Google Scholar]
- 71.Maged C The effect of mode of delivery on childhood obesity Am J Obstet Gynecol 201421001120S7724060444 [Google Scholar]
- 72.Raban O Hadar E Biron-Shental T et al. A comparison between electrical uterine monitoring, tocodynamometry and intra uterine pressure catheter for assessment of uterine activity during labor Am J Obstet Gynecol 201421001565S273 [Google Scholar]
- 73.Sheiner E, Levy A, Menes T S. et al. Maternal obesity as an independent risk factor for caesarean delivery. Paediatr Perinat Epidemiol. 2004;18:196–201. doi: 10.1111/j.1365-3016.2004.00557.x. [DOI] [PubMed] [Google Scholar]
- 74.Jensen D M, Damm P, Sørensen B. et al. Pregnancy outcome and prepregnancy body mass index in 2459 glucose-tolerant Danish women. Am J Obstet Gynecol. 2003;189:239–244. doi: 10.1067/mob.2003.441. [DOI] [PubMed] [Google Scholar]
- 75.Delpapa E H, Mueller-Heubach E. Pregnancy outcome following ultrasound diagnosis of macrosomia. Obstet Gynecol. 1991;78(3 Pt 1):340–343. [PubMed] [Google Scholar]
- 76.Parry S, Severs C P, Sehdev H M. et al. Ultrasonographic prediction of fetal macrosomia. Association with cesarean delivery. J Reprod Med. 2000;45:17–22. [PubMed] [Google Scholar]
- 77.Sacks D A, Chen W. Estimating fetal weight in the management of macrosomia. Obstet Gynecol Surv. 2000;55:229–239. doi: 10.1097/00006254-200004000-00022. [DOI] [PubMed] [Google Scholar]
- 78.Jacobsen A F, Skjeldestad F E, Sandset P M. Ante- and postnatal risk factors of venous thrombosis: a hospital-based case-control study. J Thromb Haemost. 2008;6:905–912. doi: 10.1111/j.1538-7836.2008.02961.x. [DOI] [PubMed] [Google Scholar]
- 79.Barnardo P D, Jenkins J G. Failed tracheal intubation in obstetrics: a 6-year review in a UK region. Anaesthesia. 2000;55:690–694. doi: 10.1046/j.1365-2044.2000.01536.x. [DOI] [PubMed] [Google Scholar]
- 80.Hood D D, Dewan D M. Anesthetic and obstetric outcome in morbidly obese parturients. Anesthesiology. 1993;79:1210–1218. doi: 10.1097/00000542-199312000-00011. [DOI] [PubMed] [Google Scholar]
- 81.Grau T, Bartusseck E, Conradi R. et al. Ultrasound imaging improves learning curves in obstetric epidural anesthesia: a preliminary study. Can J Anaesth. 2003;50:1047–1050. doi: 10.1007/BF03018371. [DOI] [PubMed] [Google Scholar]
- 82.Amir L H, Donath S. A systematic review of maternal obesity and breastfeeding intention, initiation and duration. BMC Pregnancy Childbirth. 2007;7:9. doi: 10.1186/1471-2393-7-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Mok E, Multon C, Piguel L. et al. Decreased full breastfeeding, altered practices, perceptions, and infant weight change of prepregnant obese women: a need for extra support. Pediatrics. 2008;121:e1319–e1324. doi: 10.1542/peds.2007-2747. [DOI] [PubMed] [Google Scholar]
- 84.Rasmussen K M, Kjolhede C L. Prepregnant overweight and obesity diminish the prolactin response to suckling in the first week postpartum. Pediatrics. 2004;113:e465–e471. doi: 10.1542/peds.113.5.e465. [DOI] [PubMed] [Google Scholar]
- 85.Dyson L McCormick F Renfrew M J Interventions for promoting the initiation of breastfeeding Cochrane Database Syst Rev 20052CD001688 [DOI] [PubMed] [Google Scholar]
- 86.Paulson J Mehta S Sokol R et al. Maternal obesity and long-term cognitive function of offspring Am J Obstet Gynecol 201421001225S446 [DOI] [PubMed] [Google Scholar]
- 87.Leermakers E A, Anglin K, Wing R R. Reducing postpartum weight retention through a correspondence intervention. Int J Obes Relat Metab Disord. 1998;22:1103–1109. doi: 10.1038/sj.ijo.0800734. [DOI] [PubMed] [Google Scholar]
- 88.Lovelady C A, Garner K E, Moreno K L. et al. The effect of weight loss in overweight, lactating women on the growth of their infants. N Engl J Med. 2000;342:449–453. doi: 10.1056/NEJM200002173420701. [DOI] [PubMed] [Google Scholar]
- 89.OʼToole M L, Sawicki M A, Artal R. Structured diet and physical activity prevent postpartum weight retention. J Womens Health (Larchmt) 2003;12:991–998. doi: 10.1089/154099903322643910. [DOI] [PubMed] [Google Scholar]
- 90.Amorim Adegboye A R Linne Y M Diet or exercise, or both, for weight reduction in women after childbirth Cochrane Database Syst Rev 20137CD005627 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Siddik-Ahmad R Garabedian M Ianovich F et al. Gestational diabetes, obesity, and self perceived risk of type 2 diabetes Am J Obstet Gynecol 2014210(Suppl.)S168–S169. [Google Scholar]
- 92.Bellamy L, Casas J P, Hingorani A D. et al. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. 2009;373:1773–1779. doi: 10.1016/S0140-6736(09)60731-5. [DOI] [PubMed] [Google Scholar]
- 93.Kim C, Newton K M, Knopp R H. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care. 2002;25:1862–1868. doi: 10.2337/diacare.25.10.1862. [DOI] [PubMed] [Google Scholar]
- 94.Colquitt J Clegg A Loveman E et al. Surgery for morbid obesity Cochrane Database Syst Rev 20054CD003641 [DOI] [PubMed] [Google Scholar]
- 95.Weiss H G, Nehoda H, Labeck B. et al. Pregnancies after adjustable gastric banding. Obes Surg. 2001;11:303–306. doi: 10.1381/096089201321336647. [DOI] [PubMed] [Google Scholar]
- 96.Kral J G, Biron S, Simard S. et al. Large maternal weight loss from obesity surgery prevents transmission of obesity to children who were followed for 2 to 18 years. Pediatrics. 2006;118:e1644–e1649. doi: 10.1542/peds.2006-1379. [DOI] [PubMed] [Google Scholar]
- 97.Willmer M, Berglind D, Sørensen T I. et al. Surgically induced interpregnancy weight loss and prevalence of overweight and obesity in offspring. PLoS One. 2013;8:e82247. doi: 10.1371/journal.pone.0082247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Astrup A, Rössner S, Van Gaal L. et al. Effects of liraglutide in the treatment of obesity: a randomised, double-blind, placebo-controlled study. Lancet. 2009;374:1606–1616. doi: 10.1016/S0140-6736(09)61375-1. [DOI] [PubMed] [Google Scholar]
- 99.Foghsgaard S, Vedtofte L, Mathiesen E R. et al. The effect of a glucagon-like peptide-1 receptor agonist on glucose tolerance in women with previous gestational diabetes mellitus: protocol for an investigator-initiated, randomised, placebo-controlled, double-blinded, parallel intervention trial. BMJ Open. 2013;3:e003834. doi: 10.1136/bmjopen-2013-003834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Authority Clinical Negligence Scheme for Trusts . NHS Litigation Authority; 2009. Maternity clinical risk management standards. [Google Scholar]
- 101.Knight-Agarwal C R, Kaur M, Williams L T. et al. The views and attitudes of health professionals providing antenatal care to women with a high BMI: a qualitative research study. Women Birth. 2013 doi: 10.1016/j.wombi.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 102.Sutherland G, Brown S, Yelland J. Applying a social disparities lens to obesity in pregnancy to inform efforts to intervene. Midwifery. 2013;29:338–343. doi: 10.1016/j.midw.2012.01.016. [DOI] [PubMed] [Google Scholar]
- 103.Johnson M, Campbell F, Messina J. et al. Weight management during pregnancy: a systematic review of qualitative evidence. Midwifery. 2013;29:1287–1296. doi: 10.1016/j.midw.2012.11.016. [DOI] [PubMed] [Google Scholar]
- 104.Wilkinson S A, Poad D, Stapleton H. Maternal overweight and obesity: a survey of cliniciansʼ characteristics and attitudes, and their responses to their pregnant clients. BMC Pregnancy Childbirth. 2013;13:117. doi: 10.1186/1471-2393-13-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Shub A, Huning E Y, Campbell K J. et al. Pregnant womenʼs knowledge of weight, weight gain, complications of obesity and weight management strategies in pregnancy. BMC Res Notes. 2013;6:278. doi: 10.1186/1756-0500-6-278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Cabrera Escobar M A, Veerman J L, Tollman S M. et al. Evidence that a tax on sugar sweetened beverages reduces the obesity rate: a meta-analysis. BMC Public Health. 2013;13:1072. doi: 10.1186/1471-2458-13-1072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Tripp N, Hainey K, Liu A. et al. An emerging model of maternity care: Smartphone, midwife, doctor? Women Birth. 2014;27:64–67. doi: 10.1016/j.wombi.2013.11.001. [DOI] [PubMed] [Google Scholar]
- 108.Denison F C, Norwood P, Bhattacharya S. et al. Association between maternal body mass index during pregnancy, short-term morbidity, and increased health service costs: a population-based study. BJOG. 2014;121:72–81. doi: 10.1111/1471-0528.12443. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
German supporting informations for this article