

Abstract
Background:
Caucasian norms are still used in the orthodontic treatment of Iranian patients, despite the different ethnic backgrounds of Iranians. The aims of this study were to evaluate the cephalometric features of an Iranian population and to establish cephalometric norms for Iranian living in the central region of Iran (Isfahan).
Materials and Methods:
A total of 238 lateral cephalometric radiographs and dental casts of Iranians (142 females and 96 males; aged 6-17 years) with acceptable profiles and Class I dental relationships were analyzed in five age groups. The mean value, standard deviation and range of 20 angular and linear variables were calculated. The resulting norms for Iranian were compared with Caucasian norms and results of other studies on Iranian population using t-test. Male and female groups were also compared using the independent t-test (P < 0.05).
Results:
Iranians tend to have an increased angle of convexity and IMPA (incisor to mandibular plane angle) and bimaxillary protrusion as compared with norms of Down's analysis. Anterior lower face height and anterior face height were greater than Burrstone's sample measurement. Sella-Nasion (S-N) length was greater than Rakosi's norm. Iranians tend to have an increased ANB (A point-Nasion-B point) angle as compared with Steiner's norms. Males tend to have greater cranial dimensions than females as indicated by the statistically significant increase in anterior face height and S-N length (P < 0.05).
Conclusion:
Iranians have distinct cephalometric features, which should be used as a reference in treating Iranian orthodontic patients.
Keywords: Cephalometry, face, normal occlusion, reference standards
INTRODUCTION
Radiographic cephalometry was firstly introduced to dentistry in 1931 by Broadbent in the USA. Thereafter, many cephalometric analyses became popular for planning orthodontic treatment. Downs (1948) developed a method of analysis on the basis of a study on 20 individuals with excellent occlusions. Over the years, his recommended standard values have proved to be remarkably consistent despite variation in the methods of study.[1,2] In 1953, Steiner developed a system of cephalometry based on simplicity and clarity of use, with the SN plane as a reference line.[3] In 1988, McNamara and Ellis surveyed the records of 125 white individuals over the age of 16 who possessed ideal facial aesthetics and balance and Class I occlusions.[4] Until today, the planning of orthodontic treatment often consists of the comparison of craniofacial measurements of a patient to the norm. However, populations show differences regarding various details of facial hard and soft-tissue. These differences are clearly discernible when individuals with different ethnic background are compared. Therefore, the orthodontic literature contains a lot of studies involving cephalometric and profile standards of European-American, African-American, Japanese and Chinese populations; but little for Iranians. Hajighadimi et al.[5] compared Iranian children with Tweed's and Steiner's standards. They found that Iranians have a more convex soft-tissue profile compared with Tweed's and Steiner's standards and this result was somehow related to the shape of the nose and the form of the lips.
Sexual dimorphism in craniofacial structures naturally appears between 12 and 15 years of age. Therefore, both male and female population groups in this age bracket must have their own cephalometric normative data for meaningful diagnosis.
The purposes of this study were: (1) to study hard tissue measurements of the facial profile for Iranian population using some of Downs, Steiner and McNamara analysis parameters, (2) to compare Iranian hard tissue values with Caucasian norms and (3) to determine any sexual or age differences in the hard tissue facial profile measurements of Iranian population.
MATERIALS AND METHODS
From the elementary, middle and high school students(6151 examined students) of five Isfahan areas, 238 subjects (96 males, 142 females) were selected who fulfilled the following criteria: (1) Iranian with Iranian grandparents, (2) acceptable facial profile and facial symmetry determined clinically, (3) class I occlusion with well-aligned maxillary and mandibular dental arches, (4) no previous orthodontic or prosthodontic therapy or cosmetic or maxillofacial surgery and (5) no significant medical history, no history of trauma and no congenital abnormalities. Clinical examinations were conducted and records (e.g., name, birthday, sex, health status) were obtained to ensure that the established criteria were observed strictly. Radiographs were only taken if both parents and subjects were informed of the amount of radiation and risks and they consented to the procedure. On the basis of chronological age, the subjects were divided into five groups within 2 years interval, starting from 6 years old except last one that were14-17 (Group 1; 6-8 years of age; Group 2; 8-10 years of age; Group 3; 10-12 years of age; Group 4; 12-14 years of age; and Group 4; 14-17 years of age). Intraoral examination, study models and lateral cephalograms were obtained from participants.
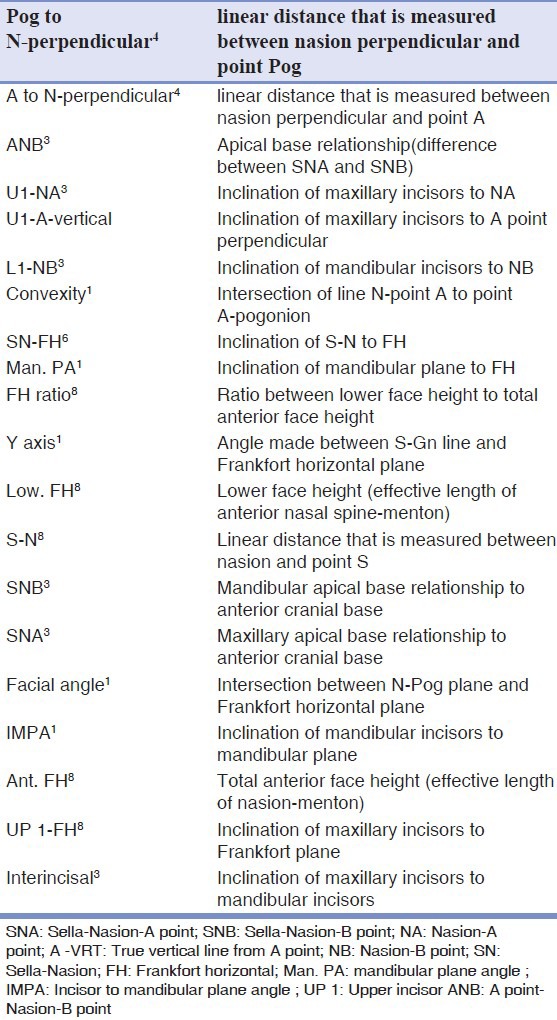
The cephalometric films of all subjects were obtained using the same X-ray unit (plan Meca 2000, USA) at natural head position, with teeth in maximum interdigitation and lips in a relaxed posture. The distance from focus to the film and from the midsagittal plane of patient head to the film for each subject was 165 cm and 20.5 cm, respectively. Therefore, cephalograms carried magnification of 8% and the adjustment for enlargement factor has been made in the linear measurements reported in the results section. The authors traced all head films according to established procedures,[6] identified all the relevant landmarks and measured both linear and angular parameters. The glossary for the parameters applied in this study is presented in Table 1. Descriptive statistics (mean, standard deviation, minimum and maximum) were computed for all measured variables. The resulting norms for Iranians were compared with Caucasian norms derived from Downs,[1,2] Steiner,[3] McNamara and Ellis,[4] Riedel,[7] Rakosi,[8] Ricketts,[9] Bolton[10] and Burstone[11] studies using t-test. The resulting Standards compared with other Iranian norms (studies of Makaarem and Sahaafian,[12] Davoody and Sassouni,[13] Sodaagar,[14] Ramezanzade[15]) using t-test. Independent t-test was performed to assess the intergender differences in measurements (P < 0.05).
Table 1.
Different linear and angular measurements used
RESULTS
Mean values and standard deviations were calculated within age and gender for the 20 measurements [Table 2]. Intergender comparison is demonstrated in [Table 3]. Table 4 demonstrates Iranian standards as compared with Caucasian and other Iranian standards.
Table 2.
Cephalometric measurements of Iranian samples according to age group and overall

Table 3.
Cephalometric measurements (mean and SD,) of samples according to sex
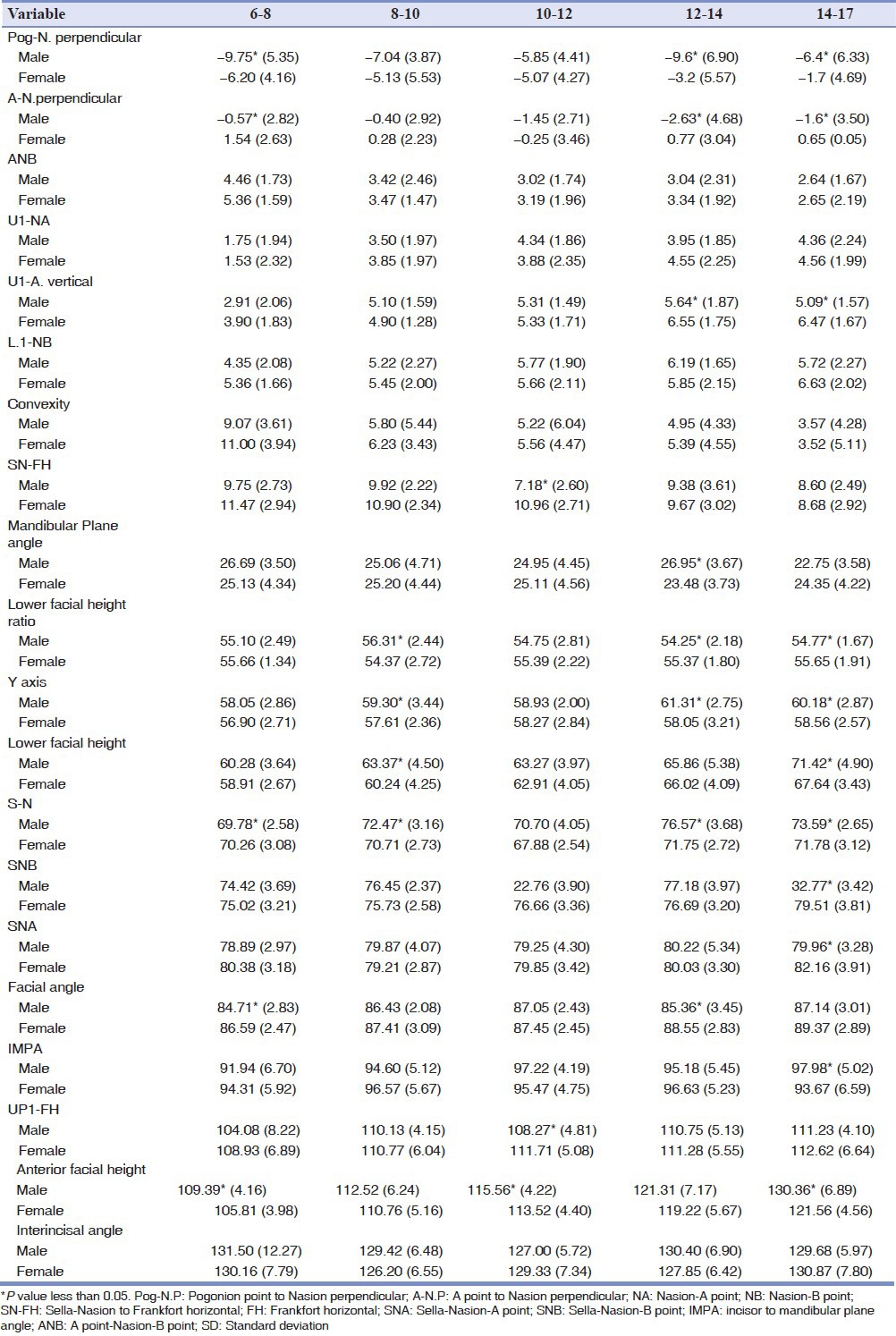
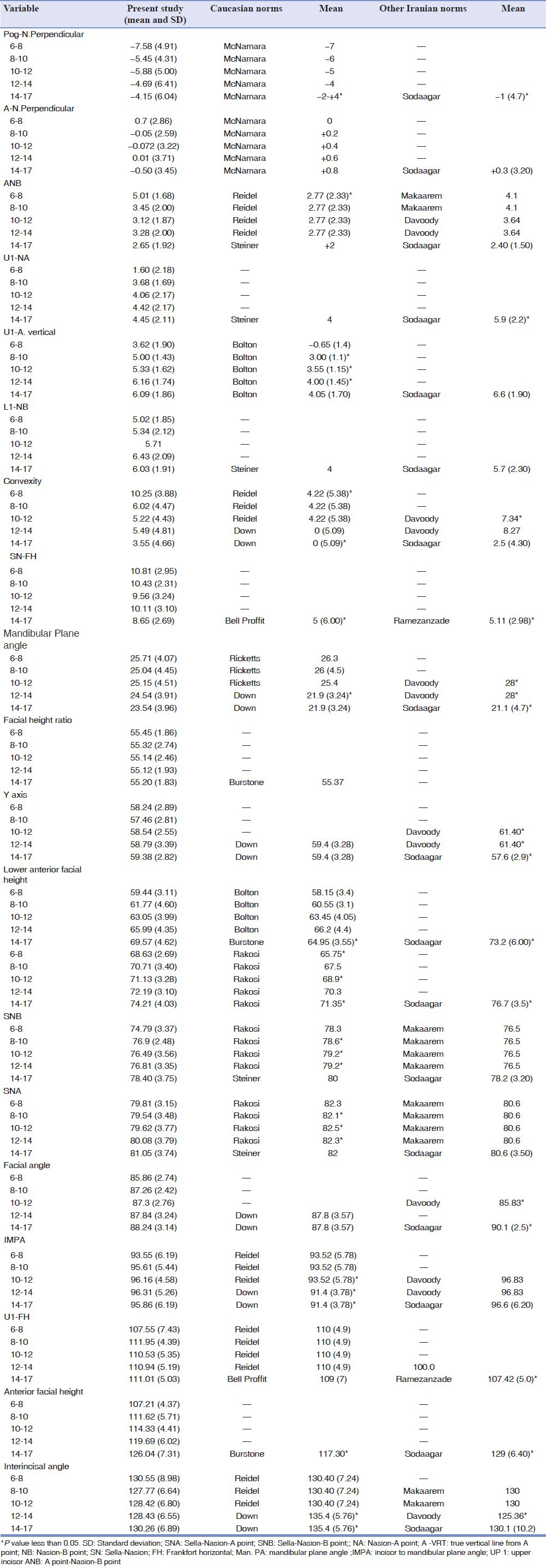
Table 4.
Iranian standards as compared with caucasians and other Iranian standards using t-test
DISCUSSION
Nowadays, large numbers of Iranians are seeking orthodontic treatment; Hence, it is important to determine cephalometric norms for this particular ethnic group and to base our treatment plans accordingly. Few studies have been carried out to define the cephalometric norms of Iranians and to determine if there are any differences between Iranians and Caucasians. The objectives of this study were to evaluate the cephalometric features of an Iranian population and to establish norms for the Iranians living in the central region of Iran. This study was performed using a larger sample size from the Iranian population than those used in previous studies. Children (6-17 years old) of both sexes were included. The data were separated on the basis of age and sex to obtain more specific and useful cephalometric normative values. In our study, we used some parameters of Down, Steiner and McNamara analysis because they present the hard tissue more in details with simplicity and directness in mind and they are widely used for evaluation of hard tissue profiles.
Since most orthodontic treatments are performed in this age group, we compared values of Group 5 (14-17 years old) with Caucasian norms.[2,3,4,7,8,9,11] When we compared Down's norms with our sample values, we found that they were similar except for the angle of convexity and IMPA(incisor to mandibular plane angle) that were greater and interincisal angle that was less than Down norms. Therefore, Iranians tend to have bimaxillary protrusion and more convex profile. Our sample values (Group 5) showed no statistically significant differences compared with Steiner's norm. They had a more posteriorly placed chin (Pog to N- perpendicular was greater than norm) as compared with McNamara norms.
The length of the anterior cranial base Sella-Nasion (S-N) increased 0.68 mm yearly (from 6 to 17 years) and is significantly greater than Caucasian values. S-N was found larger in boys in Groups 3 and particularly in Group 5. 14-17 years olds showed significant dimorphism probably because of greater growth of frontal sinus in males.
S-N to FH(Frankfort horizontal) angle decreased 0.26° yearly and is only less than Caucasian value in Group 5. This measurement showed a dimorphism in Group 4.
Angle of convexity decreased 0.81° yearly and showed no dimorphism over the entire 11-year span. Our results suggest that Iranians have slightly more convex profiles when compared with Down's norms.
A to N perpendicular were often positive in girls and negative in boys. However, a statistically significant sexual dimorphism was not evident.
SNA(Sella-Nasion-A point) and SNB(Sella-Nasion-B point) Within each age group showed no intergender differences with some exceptions in the 14-17 age groups where female growth velocity showed a spurt. Both values (SNA and SNB) were smaller than Caucasian norms.
ANB(A point-Nasion-B point) significantly decreased with age. Within each age group, ANB exhibited no sexual dimorphism. Important finding is the increased ANB angle as compared with European-Americans with Class I skeletal relationship.
Pog to N-perpendicular and facial angle of the female group was less than that of the male group. A statistically significant sexual dimorphism was evident in Groups 4 and 5 in both measurements, probably because of female growth spurt. Pog was more posterior relative to N-perpendicular as compared with Caucasian norms. Facial angle increased 0.29° a year and was less than European-Americans value.
Y-axis increments between Group 1 and Group 5 described a vertical growth pattern. Y-axis was statistically more pronounced in the male than in the female in Groups 4 and 5. Nevertheless, no statistically significant differences were present as compared with Caucasian norms.
In addition, total and lower anterior facial height tends to increase with age 2.28 and 1.22 mm each year respectively, which could be attributed to the cephalocaudal gradient of growth of the facial bones. Total and lower anterior facial height were found larger in boys, statistically more pronounced in the Group 5. Both were statistically larger in our sample than Caucasians.
Lower face height/anterior face height ratio was almost constant with age and did not show any intergender difference.
Mandibular plane angle decreased 0.26° a year from 6 to 17 years. In general, all age groups showed no statistical differences in the mandibular plane angle with Caucasian norms except in Group 4. There was no sexual dimorphism.
Most of the values for dental measurements (U1 to FH, U1 to NA and L1 to NB) in Iranians were found to be similar to the ideal norms of Caucasians and showed no dimorphism.
Interincisal angle and IMPA were less and greater than Caucasian values, respectively.
The polygon is known to be a versatile tool for practical use, which simplifies its presentation to patients. The resulting data of the 14-17 years old (means and standard deviations) were represented diagrammatically in the form of a polygon (wiggle) [Figure 1]. The two standard deviations (with different colors) were used instead of the maximum and minimum readings in the polygon, unlike the classic wiggle of Vorhies and Adams.[16]
Figure 1.
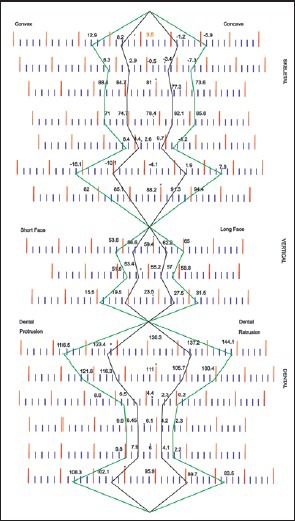
Proposed polygon
CONCLUSION
In this study, cephalometric standards for Iranian population were developed:
Iranians tend to have an increased angle of convexity and IMPA and bimaxillary protrusion as compared with norms of Down's analysis.
Anterior lower face height and anterior face height were greater than Burrstone's sample measurement.
S-N length was greater than Rakosi's norm.
Iranians tend to have an increased ANB angle as compared with Steiner's norms.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Downs WB. Analysis of the dentofacial profile. Angle Orthod. 1956;26:191. [Google Scholar]
- 2.Downs WB. Variations in facial relationships; their significance in treatment and prognosis. Am J Orthod. 1948;34:812–40. doi: 10.1016/0002-9416(48)90015-3. [DOI] [PubMed] [Google Scholar]
- 3.Steiner CC. The use of cephalometrics as an aid to planning and assessing orthodontic treatment. Am J Orthod. 1960;29:8. [Google Scholar]
- 4.McNamara JA, Jr, Ellis E., 3rd Cephalometric analysis of untreated adults with ideal facial and occlusal relationships. Int J Adult Orthodon Orthognath Surg. 1988;3:221–31. [PubMed] [Google Scholar]
- 5.Hajighadimi M, Dougherty HL, Garakani F. Cephalometric evaluation of Iranian children and its comparison with Tweed's and Steiner's standards. Am J Orthod. 1981;79:192–7. doi: 10.1016/0002-9416(81)90317-1. [DOI] [PubMed] [Google Scholar]
- 6.Jacobson A. Chicago, IL: Quintessence Publishing Co.Inc; 2006. Radiographic Cephalometry: From Basic to Video imaging; pp. 53–61. [Google Scholar]
- 7.Riedel RA. The relation of maxillary structures to cranium in malocclusion and in normal occlusion. Angle Orthod. 1952;22:142–5. [Google Scholar]
- 8.Rakosi T. 1st ed. St. Louis, Missouri: Mosby; 1982. An Atlas and Manual of Cephalometric Radiography; p. 228. [Google Scholar]
- 9.Ricketts RM. Planning treatment on the basis of the facial pattern and an estimate of its growth. Angle Orthod. 1957;27:14. [Google Scholar]
- 10.Broadbent BH, Sr, Broadbent BH, Jr, Golden WH. St. Louis: C. V. Mosby; 1975. Bolton Standard of Dentofacial Developmental Growth. [Google Scholar]
- 11.Burstone CJ. Integumental contour and extension patterns. Angle Orthod. 1959;23:146–57. [Google Scholar]
- 12.Makaarem A, Sahaafian A. A cephalometric study of dentoskeletal form on school children of Mashhad, Iran (Downs and Ballard's method) J Mash Dent Sch. 1358;3:14–25. [Google Scholar]
- 13.Davoody PR, Sassouni V. Dentofacial pattern differences between Iranians and American caucasians. Am J Orthod. 1978;73:667–75. doi: 10.1016/0002-9416(78)90227-0. [DOI] [PubMed] [Google Scholar]
- 14.Sodaagar A. Unpublished Master's Thesis. Isfahan, Iran: Medical Science University of Isfahan; 1994. Hard tissue cephalometric norms for 14-18 year-old Isfahan students. [Google Scholar]
- 15.Ramezanzade B. Unpublished Master's Thesis. Isfahan, Iran: Medical Science University of Isfahan; 1994. Dentoskeletal pattern of adults with normal occlusion. [Google Scholar]
- 16.Vorhies JM, Adams JW. Polygonic interpretation of cephalometric findings. Angle Orthod. 1951;21:194–7. doi: 10.1043/0003-3219(1951)021<0194:PIOCF>2.0.CO;2. [DOI] [PubMed] [Google Scholar]