

Abstract
Background:
The aim of the present study was to investigate the quality of root canal obturation performed by 6th year undergraduate dental students at the Dental School, University of Mashhad, Iran.
Materials and Methods:
A random 200 sample records of patients who received endodontic treatment at the Dental School, University of Mashhad between 2009 and 2010 was investigated. The quality of root canal filling was determined in relation to the adequate density and length of root filling. Statistical analysis of the data was carried out using statistical package for the social sciences (SPSS 12.0, SPSS Inc., Chicago, IL, USA) with Chi-square test. P < 0.05 was considered as significant.
Results:
About 38% of teeth fulfilled the criteria of an acceptable root canal filling. Adequate length and density of root filling was found in 73% and 66% of teeth respectively. There was significant difference between maxillary and mandibular teeth according to the quality (P = 0.009), length (P = 0.039) and density (P = 0.005) of root filling. The frequency of root canals with an acceptable filling was significantly greater in the anterior teeth than in molars.
Conclusion:
The technical quality of root canal treatment performed by undergraduate dental students was found to be less than ideal. Thus, the training course of the students at the preclinic and clinic has to be revised.
Keywords: Dental student education, periapical radiograph, root canal treatment, undergraduate student
INTRODUCTION
Retention of a high number of natural teeth is becoming more popular in contemporary society.[1] Hence, endodontic therapy is becoming an increasingly routine part of general dental practice.[2] Success of root canal treatment has been shown in the range between 53% and 94%.[3,4]
The evaluation methods used to investigate the outcome of endodontic treatment has been based on radiographic evaluation only,[5,6,7] radiographic evaluation combined with clinical findings[8,9,10] or histological examination.[11,12]
The quality of root canal treatment performed by general practitioners in different populations has also been extensively investigated.[7,13,14,15] The results from these studies showed high percentages of inadequate root canal treatment. The reasons for this are complex and may be related to the endodontic teaching that was undertaken at the dental schools.[16]
Some of the problems in endodontic teaching may be due to limitation of time allocated to endodontics, poor staff to student ratio and that teaching was mostly not undertaken by endodontists.[17]
Dental students of Mashhad University of Iran are taught endodontics in five levels. A preclinical course is given in the 3rd year in two terms, where students are trained to perform root canal treatment on extracted teeth. They are expected to complete root canal treatment of at least five anteriors, two bicuspids and four molar teeth. The other three courses are clinical, where students are expected in their 4th, 5th and 6th years to perform endodontic treatment on a variety of teeth.
The aim of this study was to evaluate the technical quality of root fillings using radiographs of teeth treated by 6th year undergraduate dental students at a dental teaching center in Mashhad, Iran.
MATERIALS AND METHODS
A random sample of 252 records of patients who had received endodontic treatment by 6th year undergraduate students at the Dental School, Mashhad University during the period of 2009 to 2010 were evaluated. Teeth with excessive root curvature were not treated by undergraduate students. Records that did not include pre- and post-operative periapical radiographs, those where the endodontic treatment was not completed, and those in which the radiographic quality was poor were excluded. The final sample consisted of 200 root filled teeth. A total of 49 were anterior teeth, 57 were premolar and 94 were molar teeth. All root canal treatments were performed by 6th year undergraduate students. An aseptic technique with rubber dam isolation was applied in all cases. Working lengths were determined with the use of radiographs. All teeth were instrumented with passive step-back technique using stainless steel K-files (Dentsply, Tulsa, OK, USA) of 0.02 taper and irrigation with 2.5% sodium hypochlorite solution. Root fillings were carried out with lateral compaction technique using gutta-percha and AH-26 sealer (Dentsply). The teeth were restored with temporary filling materials.
Clinical supervision was provided by teaching staff and post-graduate students of the department with an average staff to student ratio of 1:5.
The radiographs were examined independently by two investigators using a magnifying lens (×2) and an X-ray viewer. The results were compared and a final consensus was agreed. In case of disagreement, a third investigator was asked to read the radiograph and a final agreement was reached.
The tooth was considered as a unit with the highest score of all roots contributing the score.
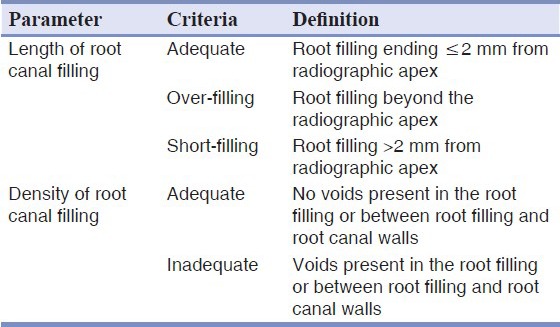
The quality of endodontic treatment was determined by the length of the root filling in relation to the radiographic apex and the density of the obturation according to presence of voids [Table 1]. “Acceptable” filling quality was defined as adequate length and density with the absence of any procedural error.
Table 1.
The criteria for the assessment of radiographic quality of root canal filling
Statistical analysis of the data was carried out using statistical package for the social sciences (SPSS) (SPSS Inc., Chicago, IL, USA) with Chi-square test (P < 0.05 was considered as significant).
RESULTS
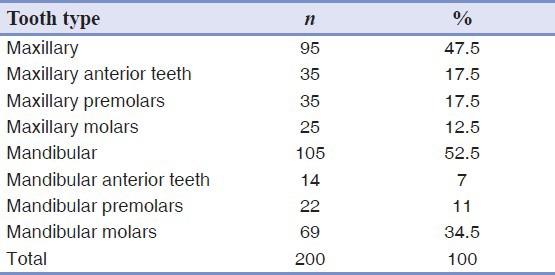
The teeth were classified according to their location in the arches. The frequency of teeth examined in this study is shown in Table 2. 95 teeth were from the maxilla and 105 were from the mandible. Each root was scored individually and the tooth was considered as a unit. The highest score of all roots (in multi-rooted teeth) was assigned and ultimately, failure of one root will lead to failure of the tooth as a whole.
Table 2.
Distribution of teeth in maxillary and mandibular arches
Quality, length and density of root canal filling are shown in Table 3. 76 of 200 teeth (38%) fulfilled the criteria of an acceptable root canal filling. Adequate length of the root filling was found in 73% of teeth, while 11% were short and 16% were overfilled. Adequate density was found in 66% of teeth.
Table 3.
Overall quality, length and density of root canal fillings

There was statistical significant difference between maxillary and mandibular teeth according to the quality of the root fillings (P = 0.009). Furthermore, there was significant difference between maxillary and mandibular teeth according to the length (P = 0.039) and density (P = 0.005) of the root fillings. 6.7% of mandibular and 15.8% of maxillary teeth had short fillings, while 12.6% of maxillary and 19% of mandibular teeth were overfilled. Adequate density was found in 24.2% of maxillary teeth and 57.1% of mandibular teeth [Table 4].
Table 4.
Quality, length and density of root canal fillings in relation to teeth position

There was relationship between tooth type and the quality of root filling. A significant difference was observed between molars and the remaining tooth types (P = 0.000). The frequency of root canals with an “acceptable” filling was significantly greater in the anterior teeth (55.1%) than in premolars (47.4%) or in molars (23.4%) [Table 5].
Table 5.
Quality, length, and density of root canal fillings according to teeth type

DISCUSSION
This study was performed to evaluate the quality of root canal fillings carried out by 6th year undergraduate students in Dental School, Mashhad University. Post-operative periapical radiographs were used for assessment. Because periapical radiographs can render only a two dimensional image, the clinical radiograph of a root filling, will lead to superimposition of the buccal and lingual images. This limitation of conventional radiographs may result in a clinical error in evaluation. Cone beam computed tomography (CBCT) can display the surface of the root and internal root canal space in three dimensions. In this way, CBCT can roughly locate the apical foramen and accordingly diagnose obturations that extend into periapical tissue or have obvious unfilled canal space. This overcomes the diagnostic limitations of periapical radiograph for the most part.[18] However, special attention should be paid to the root canal filling evaluation of endodontically treated teeth because the density of filling materials may produce image artifacts and potential risks of misdiagnosis.[19]
The quality of the root fillings was evaluated according to the criteria of Barrieshi-Nusair et al.[16] Studies evaluating the radiographic quality of root canal treatment were mostly based on the evaluation of the length and the density of the root filling.[20,21,22,23] The result of the present study indicated that adequate quality of the root fillings was achieved in 38% of teeth, which was similar to study performed by Barrieshi-Nusair et al.[16] Such frequency was lower than the 91.05% reported by Benenati and Khajotia,[24] 76% reported by Al-Yahya,[25] 63% reported by Lynch and Burke[26] and 55% reported by Eleftheriadis and Lambrianidis.[27] Furthermore, the result was higher than 13% reported by Hayes et al.[28]
The result of this study showed less than ideal root canal filling. The reasons for this are complex and may be related to the endodontic teaching that was undertaken at the dental schools.[16]
The quality of maxillary root fillings was better than mandibular in this study (P = 0.009). This may be explained by the anatomy of mandibular molars for example multi-canalled roots and their curvature. The frequency of teeth with an “acceptable” root filling was significantly greater in the anterior teeth (55.1%) than molars (23.4%) (P = 0.000). Such results are consistent with the findings of Boucher et al.[29] and Eleftheriadis and Lambrianidis[27] who reported that the technical quality was “acceptable” more often in anterior teeth. This may be explained partly by the anatomy of such teeth.
The percentage of root fillings with adequate length was 73% in the present study, which was similar to results (72.4%) reported by Er et al.[30] The percentage of root fillings with adequate length was greater when compared with those reported by Barrieshi-Nusair et al.[16] (61.3%) and Chueh et al.[31] (61.7%). However, estimation of the root filling length was probably not reproduced correctly in all radiographs because post-operative radiographs taken by undergraduate students used bisecting-angle technique. Forsberg[32] demonstrated that root fillings are projected shorter and more coronally on the X-rays exposed with the bisecting-angle technique than with the paralleling technique.
In the present study, short fillings were found in 11% of all the teeth. The highest percentage of short fillings was found in mandibular molars. This finding concurs with studies of Barrieshi-Nusair et al.[16] and Er et al.[30] This may be explained by the anatomy of these teeth such that difficult access to posterior teeth, multi-canalled roots and their curvature, makes root canal treatment more challenging for the students.
In this study, over filling was found in 16% of all the teeth. The highest percentage of over fillings was found in mandibular molars, but there was no significant difference between tooth types. Periapical lesion was found to be the most significant factor affecting the incidence of over filling. The higher percentage of over fillings reported by this study may be due to the higher incidence of the teeth with preexisting periapical radiolucency in our study. These lesions can result in resorption and destruction of the apical constriction and this loss may have influenced working length control by undergraduate students.
Inadequate density of root canal filling may lead to failure of root canal treatment because of microleakage along the root filling.[22] Eriksen and Bjertness reported that the incidence of apical periodontitis was higher in root filled teeth with inadequate densities.[33] The results of the present study indicated that adequate density occurred in 66% of cases. Such frequency was consistent with the study of Yoldas et al.[34] who reported that adequate density was achieved in 64% of teeth. On the contrary, it was greater than the 35% and 53% reported by Balto et al.[35] and Er et al.[30] respectively. However, it is difficult to compare the studies as a result of differences in the sample size.
In Dental School, Mashhad University, passive step-back instrumentation using conventional stainless steel files and cold lateral condensation have been taught to our undergraduate dental students. These techniques are the most widely taught and used technique in the dental schools.[36] A number of schools have incorporated the usage of rotary nickel–titanium instrumentation in their undergraduate teaching courses.[37] Some studies reported that when dental students used either hand or rotary nickel–titanium instruments, canals were prepared with less procedural errors and more successful treatment occurred compared with using conventional stainless steel instruments.[38,39,40,41]
In our school, preclinical endodontics is taught in two academic terms. Each term lasts 4 months with an allocation of 3 h/week at the phantom head laboratory. This short time tends to limit student's preclinical training in endodontics with consequent problems during clinical practice. Some investigators evaluating undergraduate endodontic teaching have addressed similar teaching problems.[17,37,42]
Overall, to improve the technical quality of root canal treatment performed by the undergraduate dental students, the endodontic curriculum has to be revised. Thus, the period of training of the students at the preclinic and clinic has to be extended and subsequently the clinical requirements for the endodontics have to be increased, with the result that the student will be given more time to treat more cases. The clinical training course has to be arranged to provide the students with the proper skills in endodontics starting with the basic principles in clinical endodontics.
CONCLUSION
According to the results of this study, the acceptable technical quality of root canal obturation performed by 6th year undergraduate dental students was found in less than 50% of the cases. Thus, we suggest that the endodontic training courses of the dental students at the preclinical and clinical levels to be revised.
ACKNOWLEDGMENTS
This study financially supported by the Vice Chancellor for Research of Mashhad University of Medical Sciences. The authors would like thanks to Dental Research Center, Mashad University of Medical Sciences for supporting and bringing the opportunity for writing the paper.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Daly RM, Elsner RJ, Allen PF, Burke FM. Associations between self-reported dental status and diet. J Oral Rehabil. 2003;30:964–70. doi: 10.1046/j.1365-2842.2003.01169.x. [DOI] [PubMed] [Google Scholar]
- 2.Legan JJ, Brown CE., Jr Instrumentation enhances today's endodontic care. J Indiana Dent Assoc. 1998;77:30–4. [PubMed] [Google Scholar]
- 3.Jokinen MA, Kotilainen R, Poikkeus P, Poikkeus R, Sarkki L. Clinical and radiographic study of pulpectomy and root canal therapy. Scand J Dent Res. 1978;86:366–73. doi: 10.1111/j.1600-0722.1978.tb00639.x. [DOI] [PubMed] [Google Scholar]
- 4.Lazarski MP, Walker WA, 3rd, Flores CM, Schindler WG, Hargreaves KM. Epidemiological evaluation of the outcomes of nonsurgical root canal treatment in a large cohort of insured dental patients. J Endod. 2001;27:791–6. doi: 10.1097/00004770-200112000-00021. [DOI] [PubMed] [Google Scholar]
- 5.Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endod. 1979;5:83–90. doi: 10.1016/S0099-2399(79)80154-5. [DOI] [PubMed] [Google Scholar]
- 6.Buckley M, Spångberg LS. The prevalence and technical quality of endodontic treatment in an American subpopulation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79:92–100. doi: 10.1016/s1079-2104(05)80081-2. [DOI] [PubMed] [Google Scholar]
- 7.Saunders WP, Saunders EM, Sadiq J, Cruickshank E. Technical standard of root canal treatment in an adult Scottish sub-population. Br Dent J. 1997;182:382–6. doi: 10.1038/sj.bdj.4809394. [DOI] [PubMed] [Google Scholar]
- 8.Swartz DB, Skidmore AE, Griffin JA., Jr Twenty years of endodontic success and failure. J Endod. 1983;9:198–202. doi: 10.1016/S0099-2399(83)80092-2. [DOI] [PubMed] [Google Scholar]
- 9.Smith CS, Setchell DJ, Harty FJ. Factors influencing the success of conventional root canal therapy – A five-year retrospective study. Int Endod J. 1993;26:321–33. doi: 10.1111/j.1365-2591.1993.tb00765.x. [DOI] [PubMed] [Google Scholar]
- 10.Peak JD, Hayes SJ, Bryant ST, Dummer PM. The outcome of root canal treatment. A retrospective study within the armed forces (Royal Air Force) Br Dent J. 2001;190:140–4. doi: 10.1038/sj.bdj.4800907. [DOI] [PubMed] [Google Scholar]
- 11.Lin LM, Pascon EA, Skribner J, Gängler P, Langeland K. Clinical, radiographic, and histologic study of endodontic treatment failures. Oral Surg Oral Med Oral Pathol. 1991;71:603–11. doi: 10.1016/0030-4220(91)90371-i. [DOI] [PubMed] [Google Scholar]
- 12.Lin LM, Skribner JE, Gaengler P. Factors associated with endodontic treatment failures. J Endod. 1992;18:625–7. doi: 10.1016/S0099-2399(06)81335-X. [DOI] [PubMed] [Google Scholar]
- 13.Eckerbom M, Andersson JE, Magnusson T. Frequency and technical standard of endodontic treatment in a Swedish population. Endod Dent Traumatol. 1987;3:245–8. doi: 10.1111/j.1600-9657.1987.tb00631.x. [DOI] [PubMed] [Google Scholar]
- 14.De Cleen MJ, Schuurs AH, Wesselink PR, Wu MK. Periapical status and prevalence of endodontic treatment in an adult Dutch population. Int Endod J. 1993;26:112–9. doi: 10.1111/j.1365-2591.1993.tb00552.x. [DOI] [PubMed] [Google Scholar]
- 15.De Moor RJ, Hommez GM, De Boever JG, Delmé KI, Martens GE. Periapical health related to the quality of root canal treatment in a Belgian population. Int Endod J. 2000;33:113–20. doi: 10.1046/j.1365-2591.2000.00295.x. [DOI] [PubMed] [Google Scholar]
- 16.Barrieshi-Nusair KM, Al-Omari MA, Al-Hiyasat AS. Radiographic technical quality of root canal treatment performed by dental students at the dental teaching center in Jordan. J Dent. 2004;32:301–7. doi: 10.1016/j.jdent.2004.01.002. [DOI] [PubMed] [Google Scholar]
- 17.Dummer PM. Comparison of undergraduate endodontic teaching programmes in the United Kingdom and in some dental schools in Europe and the United States. Int Endod J. 1991;24:169–77. doi: 10.1111/j.1365-2591.1991.tb00127.x. [DOI] [PubMed] [Google Scholar]
- 18.Cheng L, Zhang R, Yu X, Tian Y, Wang H, Zheng G, et al. A comparative analysis of periapical radiography and cone-beam computerized tomography for the evaluation of endodontic obturation length. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112:383–9. doi: 10.1016/j.tripleo.2011.04.025. [DOI] [PubMed] [Google Scholar]
- 19.Decurcio DA, Bueno MR, de Alencar AH, Porto OC, Azevedo BC, Estrela C. Effect of root canal filling materials on dimensions of cone-beam computed tomography images. J Appl Oral Sci. 2012;20:260–7. doi: 10.1590/S1678-77572012000200023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dugas NN, Lawrence HP, Teplitsky PE, Pharoah MJ, Friedman S. Periapical health and treatment quality assessment of root-filled teeth in two Canadian populations. Int Endod J. 2003;36:181–92. doi: 10.1046/j.1365-2591.2003.00640.x. [DOI] [PubMed] [Google Scholar]
- 21.Helminen SE, Vehkalahti M, Kerosuo E, Murtomaa H. Quality evaluation of process of root canal treatments performed on young adults in Finnish public oral health service. J Dent. 2000;28:227–32. doi: 10.1016/s0300-5712(99)00076-7. [DOI] [PubMed] [Google Scholar]
- 22.Kirkevang LL, Hörsted-Bindslev P, Orstavik D, Wenzel A. A comparison of the quality of root canal treatment in two Danish subpopulations examined 1974-75 and 1997-98. Int Endod J. 2001;34:607–12. doi: 10.1046/j.1365-2591.2001.00436.x. [DOI] [PubMed] [Google Scholar]
- 23.Lupi-Pegurier L, Bertrand MF, Muller-Bolla M, Rocca JP, Bolla M. Periapical status, prevalence and quality of endodontic treatment in an adult French population. Int Endod J. 2002;35:690–7. doi: 10.1046/j.1365-2591.2002.00547.x. [DOI] [PubMed] [Google Scholar]
- 24.Benenati FW, Khajotia SS. A radiographic recall evaluation of 894 endodontic cases treated in a dental school setting. J Endod. 2002;28:391–5. doi: 10.1097/00004770-200205000-00011. [DOI] [PubMed] [Google Scholar]
- 25.Al-Yahya A. Analysis of student's performance in an undergraduate endodontic's program. Saudi Dent J. 1990;2:58–61. [Google Scholar]
- 26.Lynch CD, Burke FM. Quality of root canal fillings performed by undergraduate dental students on single-rooted teeth. Eur J Dent Educ. 2006;10:67–72. doi: 10.1111/j.1600-0579.2006.00397.x. [DOI] [PubMed] [Google Scholar]
- 27.Eleftheriadis GI, Lambrianidis TP. Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. Int Endod J. 2005;38:725–34. doi: 10.1111/j.1365-2591.2005.01008.x. [DOI] [PubMed] [Google Scholar]
- 28.Hayes SJ, Gibson M, Hammond M, Bryant ST, Dummer PM. An audit of root canal treatment performed by undergraduate students. Int Endod J. 2001;34:501–5. doi: 10.1046/j.1365-2591.2001.00421.x. [DOI] [PubMed] [Google Scholar]
- 29.Boucher Y, Matossian L, Rilliard F, Machtou P. Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. Int Endod J. 2002;35:229–38. doi: 10.1046/j.1365-2591.2002.00469.x. [DOI] [PubMed] [Google Scholar]
- 30.Er O, Sagsen B, Maden M, Cinar S, Kahraman Y. Radiographic technical quality of root fillings performed by dental students in Turkey. Int Endod J. 2006;39:867–72. doi: 10.1111/j.1365-2591.2006.01158.x. [DOI] [PubMed] [Google Scholar]
- 31.Chueh LH, Chen SC, Lee CM, Hsu YY, Pai SF, Kuo ML, et al. Technical quality of root canal treatment in Taiwan. Int Endod J. 2003;36:416–22. doi: 10.1046/j.1365-2591.2003.00672.x. [DOI] [PubMed] [Google Scholar]
- 32.Forsberg J. Estimation of the root filling length with the paralleling and bisecting-angle techniques performed by undergraduate students. Int Endod J. 1987;20:282–6. doi: 10.1111/j.1365-2591.1987.tb00628.x. [DOI] [PubMed] [Google Scholar]
- 33.Eriksen HM, Bjertness E. Prevalence of apical periodontitis and results of endodontic treatment in middle-aged adults in Norway. Endod Dent Traumatol. 1991;7:1–4. doi: 10.1111/j.1600-9657.1991.tb00174.x. [DOI] [PubMed] [Google Scholar]
- 34.Yoldas O, Topuz A, Isçi AS, Oztunc H. Postoperative pain after endodontic retreatment: Single- versus two-visit treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:483–7. doi: 10.1016/j.tripleo.2004.03.009. [DOI] [PubMed] [Google Scholar]
- 35.Balto H, Al Khalifah Sh, Al Mugairin S, Al Deeb M, Al-Madi E. Technical quality of root fillings performed by undergraduate students in Saudi Arabia. Int Endod J. 2010;43:292–300. doi: 10.1111/j.1365-2591.2009.01679.x. [DOI] [PubMed] [Google Scholar]
- 36.Cailleteau JG, Mullaney TP. Prevalence of teaching apical patency and various instrumentation and obturation techniques in United States dental schools. J Endod. 1997;23:394–6. doi: 10.1016/S0099-2399(97)80191-4. [DOI] [PubMed] [Google Scholar]
- 37.Qualtrough AJ, Whitworth JM, Dummer PM. Preclinical endodontology: An international comparison. Int Endod J. 1999;32:406–14. doi: 10.1046/j.1365-2591.1999.00253.x. [DOI] [PubMed] [Google Scholar]
- 38.Park H. A comparison of Greater Taper files, ProFiles, and stainless steel files to shape curved root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91:715–8. doi: 10.1067/moe.2001.114159. [DOI] [PubMed] [Google Scholar]
- 39.Pettiette MT, Metzger Z, Phillips C, Trope M. Endodontic complications of root canal therapy performed by dental students with stainless-steel K-files and nickel-titanium hand files. J Endod. 1999;25:230–4. doi: 10.1016/S0099-2399(99)80148-4. [DOI] [PubMed] [Google Scholar]
- 40.Pettiette MT, Delano EO, Trope M. Evaluation of success rate of endodontic treatment performed by students with stainless-steel K-files and nickel-titanium hand files. J Endod. 2001;27:124–7. doi: 10.1097/00004770-200102000-00017. [DOI] [PubMed] [Google Scholar]
- 41.Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni-Ti rotary GT files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001;34:476–84. doi: 10.1046/j.1365-2591.2001.00422.x. [DOI] [PubMed] [Google Scholar]
- 42.Qualtrough AJ, Dummer PM. Undergraduate endodontic teaching in the United Kingdom: An update. Int Endod J. 1997;30:234–9. doi: 10.1046/j.1365-2591.1997.t01-1-00072.x. [DOI] [PubMed] [Google Scholar]