

Abstract
Background:
This study sought to assess symphyseal morphology in adolescents with different mandibular growth patterns (MGPs) in order to see if a relation exists.
Materials and Methods:
In this study the symphyseal parameters (height, depth, and ratio) of normal subjects were compared with four groups with malocclusion (cl III vertical, cl II vertical, cl III horizontal, and cl II horizontal). These groups (15 samples each) were matched (for sex and cervical maturation stage [CVMS]) based on their cephalograms and patient charts. Growth patterns were differentiated by seven vertical parameters and the Wylie analysis. After confirmation of normality of the groups and similarity of their variances the two-way analysis of variance (ANOVA) was used for analysis of data assessed by adjusted chi-square (P < 0.001). The comparison of cases with the normal group was performed by the Dunnett method. Intraclass Correlation Coefficient (ICC) was used for evaluation of intraobserver reliability.
Results:
We found the symphyseal ratio to have a significant correlation with the MGP (P < 0.001). The symphyseal ratio (Height/Depth) was small in a mandible with vertical growth pattern Cl II or Cl III. Conversely, a horizontal growth pattern of a Cl II or Cl III mandible was associated with a larger ratio of the symphysis in comparison with the normal group. The symphyseal ratio was also found to be greater in females.
Conclusion:
The symphyseal ratio was found to be strongly associated with the MGP.
Keywords: Horizontal, mandibular growth, symphysis, vertical
INTRODUCTION
Prediction of mandibular growth pattern (MGP) plays an important role in orthodontic treatment planning; it is critical when managing the development of dentofacial structures.[1,2,3,4,5,6,7] Different methods have been introduced for predicting MGP and assessing, symphyseal morphology is one of them.[1,2,3,4,5,6,7,8,9,10,11,12] Ricketts and others stated that morphology of the symphysis may be used to predict the direction of mandibular growth. He associated a thick symphysis with an anterior growth direction.[9] Bjork[6] described multiple structural configurations in extreme types of mandibular rotators. He found that forward inclination of the condylar head was associated with forward mandibular rotation, along with a greater curvature of the mandibular canal compared with mandibular contour. A tendency toward backward mandibular rotation was associated with a pronounced apposition below the symphysis with more overall concavity of the inferior mandibular border. Proclination of the symphysis is an indicator of a backward rotating mandible. Jarabak's cephalometric analysis predicted the direction of mandibular growth by a facial polygon, including the saddle angle (N-S-Ar), articular angle (S-Ar-Go), and gonial angle (Ar-Go-Me); a sum of these three angles greater than 396 is predictive of a posterior MGP while a sum less than 396 was associated with anterior MGP. Also a ratio of posterior (S-Go) to anterior face height (N-Me) of 56-62% indicated a posterior MGP, whereas a ratio of 65-80% indicated an anterior growth tendency.[13] Although many cephalometric measurements have been introduced, it is still very difficult to accurately predict the direction of mandibular growth.[1,2,3,4,5,6,7,8,9,10,11,12,14,15] Lee et al..[16] studied the reliability of the Skieller's prediction method. Although, Skieller's four variables accounted for 86% of the variability of changes in the direction of mandibular growth (mandibular inclination, intermolar angle, shape of the inferior border of the mandible, and inclination of the symphysis); however, it accounted for only 8% in Lee's study. Thus, he concluded that predicting the direction of mandibular growth is very perplexing and problematic. Aki et al.[10] assessed symphyseal height, depth ratio (H/D) and angle. In his study, the morphology of the symphysis was found to be associated with the direction of mandibular growth. A mandible with an anterior growth direction was associated with a small height, large depth, small ratio, and large angle of the symphysis. Conversely, a posterior growth direction was associated with a large height, small depth, large ratio, and small angle of the symphysis. The purpose of this study was to evaluate symphyseal morphology (Height, Depth, and Height/Depth) in patients aged between 9 and 14 years with different sagittal and vertical MGPs.
MATERIALS AND METHODS
Lateral cephalometric radiographs and charts of adolescents aged between 9 and 14 years were used in this study. The first part of the study was conducted on 60 normal cephalograms taken from normal individuals according to normal occlusion defined by Moyer's[17] and appropriate facial proportions were approved by two orthodontists. The samples had no history of orthodontic treatment or history of systemic or developmental diseases.
To find normal value for vertical growth pattern of mandible vertical indices, that is, the sum of Bijork angles, Gonial angle and SN-Man angle were used. Wylie's analysis was also used for assessing sagittal growth pattern of mandible, which included mandibular length and lower mandibular length.[18] The second part of the study was to define case groups, which included Cl II vertical, Cl III vertical, Cl II horizontal, and Cl III horizontal patients with normal maxillae.
Samples were selected from the patients referred to the Orthodontic or Pediatric Departments.
Patients within the mean range (±2 SD) were defined as normal. The four case groups were those who were out of this range classified as horizontal or vertical growing patterns according to vertical indices[10] and as Cl II or Cl III skeletal growing patterns according to Wylie indices.[18]
There were 15 samples in each group that were matched to normal groups according to sex and cervical maturation stage (CVMS). Baccetti's method was used for CVMS determination[19,20] [Figure 1].
Figure 1.
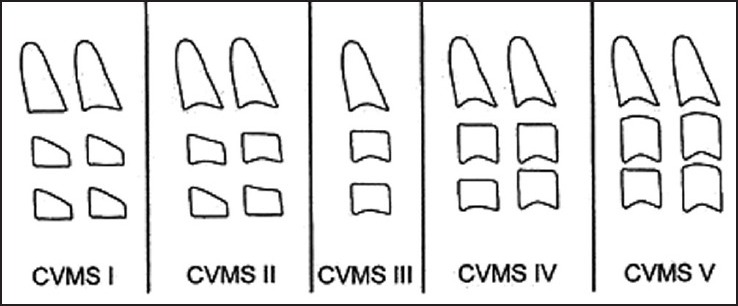
Baccetti's method for evaluation of the cervical maturation stage
The symphyseal measurement included height, depth, and ratio (H/D) measured according to the Aki et al. study.[10]
Linear measurements used the tangent drawn at point B and parallel and perpendicular lines drawn to this tangent. The method of measuring height and depth of the symphysis[10] is shown in Figure 2.
Figure 2.
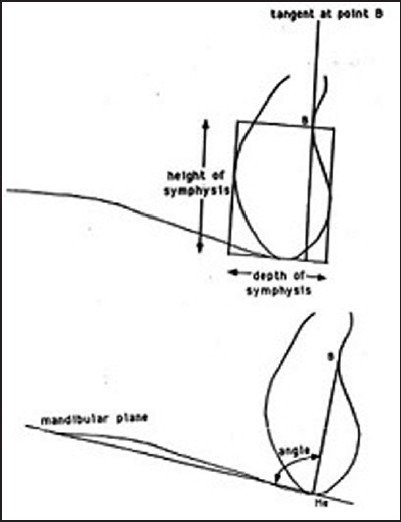
Cephalometric measurements used to quantify symphysis morphology
All radiographs were taken with the same panoramic radiographic device (PLANMECA Proline x, Helsinki, Finland). All of them were scanned and digitized (dpi 300), and the measurements were made using Dolphin imaging software, version 10 (Patterson Dental Supply, USA)
For symphyseal parameters, real size tracings were printed by Dolphin Imaging software and measured using a grid.
Statistical analysis
Normal data distribution was evaluated by one sample k-s test and the Levene test was performed to indicate variance equality between groups. After confirmation of normality of the groups and equation of their variances, the two-way analysis of variance (ANOVA) model was assessed by adjusted chi-square for analysis of data (P < 0.001), and the comparison of cases with the normal group was performed using the Dunnett method. For evaluation of intraobserver reliability, Intraclass Correlation Coefficient (ICC) was assessed and the reliability was approved (ICC coefficiency was between 0.0726 and 0.0871).
RESULTS
Evaluation of CVMS
Evaluation of 60 normal radiographs with the Baccetti method showed that 21 were in stage III, 29 were in stage II, and the remaining were in stage I. The case groups also were selected from the patients in stage III and matched to 15 samples with normal radiographs, which were in the same stage. Each group consisted of seven female and eight male patients.
Evaluation of sagittal and vertical analysis
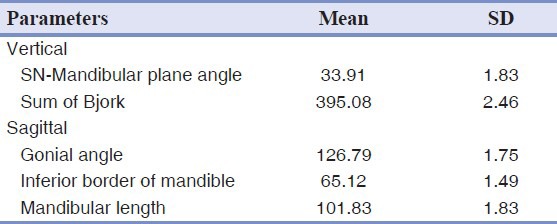
Mean and standard deviation of the sagittal and vertical parameters are shown in Table 1.
Table 1.
Mean and standard deviation of mandibular parameters of sagittal and vertical analysis
Comparison between subgroups
Table 2 lists the height and depth of the symphysis based on sex and growth pattern in study groups. Comparison of each case group with normal group showed only statistically significant differences between the normal group and Cl II horizontal and Cl III vertical groups in height (P < 0.001). There was no significant difference relevant to sex.
Table 2.
Mean and standard deviation of symphyseal height and depth in the normal group and four subgroups based on gender
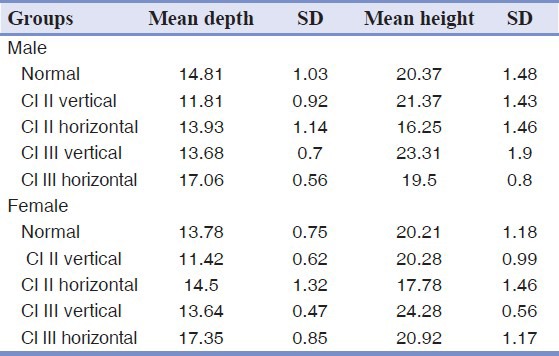
Comparison of each case group with the normal group showed only statistically significant difference between it and the Cl III horizontal and Cl II vertical groups in depth (P < 0.001) and no significant difference relevant to sex.
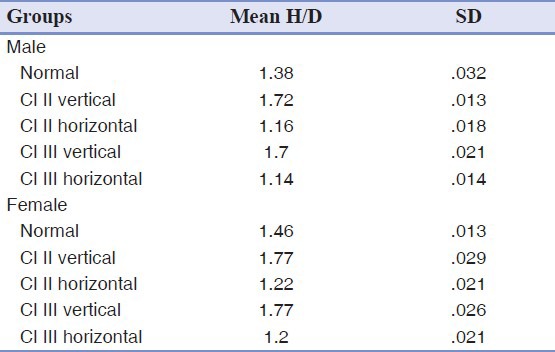
Table 3 shows the symphysis ratio relevant to sex and growth pattern. The female patients had significantly greater H/D compared with male patients. All four case groups had statistically significant differences compared with the normal group.
Table 3.
Mean and standard deviation of symphyseal ratio in the normal group and four subgroups based on gender
The intraobserver reliability was assessed by ICC of reliability.
DISCUSSION
Different approaches have been used for prediction of MGPs.[1,2,3,4,5,6,7,8,9,10,11,12,21,22] Quantification of skeletal data has been shown to be an effective and reliable method of demonstrating variation in human growth as well as for monitoring and interpreting the growth of various skeletal elements in the living.[23] Morphological changes in the mandibular body had been studied in previous researches, and it was found that the gonial angle became significantly smaller after the third molar eruption. Also, the posterior mandibular body length had a linear correlation with Gonial angle.[24]
One of the recent methods introduced by Aki et al.[10] is symphysis morphology. Due to ease in selection of landmarks for evaluating symphysis morphology in cephalograms, we used his measurements to evaluate their variation in four different MGPs. The characteristics of the normal subjects were mentioned in other studies.[25,26]
Despite wide variations in the size and shape of the human face, head, and body, there is remarkable consistency for quantifiable gender-specific facial traits.[27] In one study, significant relationships were found between the measures of mandibular incisor crowding and basal bone dimensions in female subjects. Except for the vestibular part of cancellous bone thickness, all mandibular incisor bone measurements were greater in the male subjects than in the female subjects.[28]
We matched our study groups according to the Baccetti's skeletal age, in order to lower the developmental age effect on the mandibular growth. The samples were also matched based on gender. In this way, the confounding effect of gender and skeletal age was minimized on mandibular growth.
It was also found that there was a sexual dimorphism on the morphology of the symphysis, with the mean symphyseal ratio being higher in the female samples than in the male samples. This difference has been indicated in all studies on mandibular growth, because bone deposition in the pogonion region is an x-linked trait.[10]
Symphyseal morphology differed significantly between normal subjects and the study subgroups. It was noticed that with horizontal growth patterns of the mandible whether in Cl II or Cl III, the symphyseal ratio was higher than in the normal group. In cases with vertical growth patterns either Cl II or Cl III, the ratio was lower. The depth increased from vertical growth to horizontal growth in the mandible.
Not all of the symphyseal measurements were significantly different between subgroups. The height of the symphysis was greatest in Cl III vertical and the least in ClII horizontal groups, with no significant difference in other subgroups. Regarding the depth of the symphysis, the greatest depth was measured in Cl III horizontal and the least was indicated in the Cl II vertical group.
The size and shape of the mandibular symphysis is an important consideration in evaluation of orthodontic patients.[6,10,29,30] With a prominent symphysis, more protrusion of the incisors is esthetically acceptable and therefore a greater chance that a nonextraction approach to treatment may be considered. Conversely, in patients with greater symphyseal height and small chin, an extraction approach is preferred for compensation of arch length discrepancies.[16,31] This concept was confirmed by the results of our study because we measured the deepest depth in horizontal growth patterns; therefore, we can use nonextraction approach in these individuals. Furthermore in vertical growth patterns it is better to extract teeth because of the decreased symphyseal depth.
Aki et al.[10] did a study to determine whether symphysis morphology could be used as a predictor of the direction of mandibular growth and to assess growth changes of the symphysis. They determined the direction of mandibular growth based on vertical parameters and divided it into anterior and posterior growth patterns. Consequently, they subdivided the size of the symphysis into large, small, and medium. Symphysis morphology was found to be associated with the direction of mandibular growth, especially in male subjects with symphysis ratio having the strongest relationship in adults. A mandible with an anterior growth direction was associated with a small height, large depth, small ratio, and large angle of the symphysis. Conversely, a posterior growth direction was associated with a large height, small depth, large ratio, and small angle of the symphysis. Symphyseal dimensions continued to change until adulthood with male subjects having a greater and later change compared with female subjects. Their findings were in accordance to our study. In addition, the ratio was low in horizontal growth (anterior growth direction) and the depth was greater. It seems that based on both studies, the symphysis morphology is different in various vertical growth patterns of the mandible.
CONCLUSION
In summary, we can conclude that female adolescents had greater symphyseal ratio in comparison to male adolescents. Also, symphyseal depth differed significantly in vertical and horizontal growth patterns in comparison to normal groups and symphysis ratio (Height/Depth) was strongly related to the vertical pattern of mandibular growth in both genders.
Footnotes
Source of Support: Author would like to thank orthodontics department of shaheed behashti dental school for their kind cooperation
Conflict of Interest: None declared
REFERENCES
- 1.Huggare J. The first cervical vertebra as an indicator of mandibular growth. Eur J Orthod. 1993;11:10–6. doi: 10.1093/oxfordjournals.ejo.a035959. [DOI] [PubMed] [Google Scholar]
- 2.Solow B, Siersback-Nielsen S. Cervical and craniocervical posture as predictors of craniofacial growth. Am J Orthod Dentofacial Orthop. 1992;101:449–58. doi: 10.1016/0889-5406(92)70119-u. [DOI] [PubMed] [Google Scholar]
- 3.Rossouw PE, Lombard CJ, Harris AM. The frontal sinus and mandibular growth prediction. Am J Orthod Dentofacial Orthop. 1991;100:542–6. doi: 10.1016/0889-5406(91)70095-E. [DOI] [PubMed] [Google Scholar]
- 4.Lundstrom A, Woodside DG. A comparison of various facial and occlusal characteristics in mature individuals with vertical and horizontal growth direction expressed at the chin. Eur J Orthod. 1981;3:227–35. doi: 10.1093/ejo/3.4.227. [DOI] [PubMed] [Google Scholar]
- 5.Chen F, Terada K, Saito I. Longitudinal intermaxillery relationships in Cl III malocclusions with low and high mandibular plane angles. Angle Orthod. 2007;77:397–403. doi: 10.2319/0003-3219(2007)077[0397:LIRICI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Bjork A. Prediction of mandibular rotation. Am J Orthod. 1969;55:585–99. doi: 10.1016/0002-9416(69)90036-0. [DOI] [PubMed] [Google Scholar]
- 7.Zhang M, Zhao Q, Chen YX. Dimensional differences in craniofacial morphologies of prepubescence Cl II patients with deep and shallow mandibular antegonial notching. Hua Xi Kou ing Yi Xue Za Zhi. 2006;24:142–5. [PubMed] [Google Scholar]
- 8.Kolodziej RP, Southard TE, Southard KA, Casko JS, Jakobsen JR. Evaluation of antegonial notch depth for growth prediction. Am J Orthod Dentofacial Orthop. 2002;121:357–63. doi: 10.1067/mod.2002.121561. [DOI] [PubMed] [Google Scholar]
- 9.Ricketts RM. Cephalometric synthesis. Am J Orthod. 1965;35:36–50. [Google Scholar]
- 10.Aki T, Nanda RS, Currier GF, Nanda SK. Assessment of symphysis morphology as a predictor of the direction of mandibular growth. Am J Orthod Dentofacial Orthop. 1994;106:60–9. doi: 10.1016/S0889-5406(94)70022-2. [DOI] [PubMed] [Google Scholar]
- 11.Tanaka R, Suzuki H, Maeda H, Kobayashi K. Relationship between and inclination of mandibular plane and a morphology of symphysis. Nippon Kyosei Shika Gakkai Zasshi. 1989;48:20–7. [PubMed] [Google Scholar]
- 12.Bushong PH, Julian K, Sachdeva R, Demirjian A. Childhood and pubertal growth changes of the human symphysis. Angle Orthod. 1992;62:203–10. doi: 10.1043/0003-3219(1992)062<0203:CAPGCO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Jaraback JR, Fizzell JA. Vol. 1. St Louis: CV Mosby; 1972. Technique and treatment with light-wire edge wise appliance; pp. 128–58. [Google Scholar]
- 14.Ochoa BK, Nanda RS. Comparison of maxillary an mandibular growth. Am J Orthod Dentofacial Orthop. 2004;125:148–59. doi: 10.1016/j.ajodo.2003.03.008. [DOI] [PubMed] [Google Scholar]
- 15.Eroz UB, Ceylan I, Aydemir S. An investigation of mandibular morphology in subjects with different vertical facial growth patterns. Aust Orthod J. 2000;16:16–22. [PubMed] [Google Scholar]
- 16.Lee RS, Daniell FJ, Swartz M, Baumrind S, Korn EL. Assessment of a method for the prediction of mandibular rotation. Am J Orthod Dentofacial Orthop. 1987;91:395–40. doi: 10.1016/0889-5406(87)90392-1. [DOI] [PubMed] [Google Scholar]
- 17.Moyers RE. 1st ed. Chap 6. Chicago: London Yearbook Medical Publisher; 1988. Handbook of Orthodontics c; pp. 114–21. [Google Scholar]
- 18.Wendell L, Wylie D. The assessment of anteroposterior dysplasia. Angle Orthod. 1947;17:97–109. [Google Scholar]
- 19.Baccetti T, Franchi L, Macnrmara JA. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Sem Orthod. 2005;11:119–29. [Google Scholar]
- 20.Franchi L, Baccetti T. Transverse maxillary deficiency in Cl II and Cl III malocclusions: A cephalometric and morphologic study on postero-anterior films. Orthod Craniofac Res. 2005;8:21–8. doi: 10.1111/j.1601-6343.2004.00312.x. [DOI] [PubMed] [Google Scholar]
- 21.Liu YP, Behrents RG, Buschang PH. Mandibular growth, remodeling and maturation during infancy and early childhood. Angle Orthod. 2010;80:97–105. doi: 10.2319/020309-67.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Leslie LR, Southard TE, Southard KA, Casko JS, Jakobsen JR, Tolley EA, et al. Prediction of mandibular growth rotation: Assessment of Skieller, Bjork and Linde-hansen method. Am J Orthod Dentofacial Orthop. 2005;114:659–67. doi: 10.1016/s0889-5406(98)70198-2. [DOI] [PubMed] [Google Scholar]
- 23.Hutchinson EF, L’Abbé EN, Oettlé AC. An assessment of early mandibular growth. Forensic Sci Int. 2012;217:233e1–6. doi: 10.1016/j.forsciint.2011.11.014. [DOI] [PubMed] [Google Scholar]
- 24.Ogawa T, Osato S. Growth changes of the mandibular body with eruption of mandibular third molars: Analysis of anatomical morphometry and quantitative bone mineral content by using radiography. Ann Anat. 2013;195:143–50. doi: 10.1016/j.aanat.2012.07.011. [DOI] [PubMed] [Google Scholar]
- 25.Nouri M, Saffar Pour M, Azimi S. Longitudinal cephalometric study of mandible growth in Qazvin children with normal occlusion. J Qazvin Univ Med Sci. 2006;10:9–16. [Google Scholar]
- 26.Nouri M, Mokhtari M, Jabouri M, Einollahi AR, Hassani N. Longitudinal cephalometric growth of 9-11 years normall occlusion Iranian children. J Qazvin Univ Med Sci. 2003;27:65–77. [Google Scholar]
- 27.Glowacki J, Christoph K. Gender Differences in the Growing, Abnormal, and Aging Jaw. Dent Clin North Am. 2013;57:263–80. doi: 10.1016/j.cden.2013.01.005. [DOI] [PubMed] [Google Scholar]
- 28.Uysal T, Yagci A, Ozer T, Veli I, Ozturk A. Mandibular anterior bony support and incisor crowding: Is there a relationship? Am J Orthod Dentofacial Orthop. 2012;142:645–53. doi: 10.1016/j.ajodo.2012.05.017. [DOI] [PubMed] [Google Scholar]
- 29.Forster CM, Sunga E, Chung CH. Relationship between dental arch width and vertical facial morphology in untreated adults. Eur J Orthod. 2008;10:323–9. doi: 10.1093/ejo/cjm113. [DOI] [PubMed] [Google Scholar]
- 30.Wagner DM, Chung CH. Transverse growth of the maxilla and mandible in untreated girls with low, moderate and high MP-SN angles: A longitudinal study. Am J Orthod Dentofacial Orthop. 2005;28:76–23. doi: 10.1016/j.ajodo.2004.09.028. [DOI] [PubMed] [Google Scholar]
- 31.Gaukroger MJ, Noar JH, Sanders R, Semb G. A cepholometric inter-center comparison of growth in children with cleft lip and palate. J Orthod. 2002;29:113–7. doi: 10.1093/ortho/29.2.113. [DOI] [PubMed] [Google Scholar]